
Abstract
Background:
New risk areas for tick-borne encephalitis (TBE) are emerging and the spread of disease and vaccine coverage is unclear in Sweden. We wanted to study the prevalence and levels of TBE-virus (TBEV) antibodies in southern Sweden, and to investigate whether there were individuals with undiagnosed TBE.
Materials and Methods:
Two cohorts of sera were collected: One group of anonymous individuals in rural areas (AIRA) in Skåne and one group of volunteers who often got tick-bites (tick-bitten individuals [TBI]). An enzyme-linked immunosorbent assay for TBEV IgM and IgG was performed, as well as a TBEV neutralization test (NT) in selected individuals.
Results:
In the AIRA group, there was an IgG seropositivity of 5.3%. There were individuals with high antibody levels both in areas previously considered as risk areas (Bromölla and Knislinge), as well as in another area (Tyringe). In the TBI group, 45% of the individuals were vaccinated according to the questionnaires and IgG seropositivity was 28%. A lower seroprevalence and levels of antibodies were seen in the middle-aged group (50–69 years) compared with younger or elderly study participants. A positive NT revealed several individuals with suspected undiagnosed episodes of TBE.
Conclusion:
Subclinical or misdiagnosed cases have probably occurred in Skåne. Middle-aged individuals had lower levels of IgG, which could indicate either less tick exposure or a lower vaccine response. Less than half of the TBI were vaccinated, an indication that more information about the disease and vaccine might be needed. We conclude that the study motivates an increased awareness of TBEV in the region.
Introduction
Tick-borne encephalitis (TBE) was described as a potentially distinct disease in 1931, while the pathogen, TBE virus (TBEV), was described in far-eastern Russia by Zilber in 1937. TBEV belongs to the genus Flavivirus, with five different subtypes proposed: European, Siberian, Far-Eastern, and more recently Baikalian and Himalyan subtypes (Ruzek et al. 2019). The typical clinical symptoms follow a biphasic pattern with the first phase consisting of nonspecific symptoms such as mild fever, myalgia, nausea, and headache. The second phase may in some cases follow 1–2 weeks later. This phase includes potentially severe neurological symptoms due to meningitis or encephalitis. A vaccination program against TBE has been recommended in some risk areas in Sweden, but the coverage in the region of Skåne in the very southern part of Sweden is today uncertain (Charrel et al. 2004).
In southern Sweden, the primary vector for the European subtype is considered to be the Ixodes ricinus tick, even if recent reports from other parts of the country show presence of Ixodes persulcatus, which is the primary vector of the Siberian subtype of TBEV (Jaenson et al. 2012, Kjaer et al. 2019). Since the first described cases of TBE in Sweden in 1950s in the archipelago and coastal areas of Stockholm, both the annual number of cases and the geographical spread have increased considerably (Jaenson et al. 2012; Reports 1–2, 2020).
Both impact from migratory birds and roe deers have been proposed as important factors in spreading ticks and tick-borne diseases, including TBEV, and the abundance of ticks has increased in Skåne during the last decades (Jaenson et al. 2012). An increasing number of cases have been reported in several and distinct parts of Skåne, and during the past years, between 5 and 10 clinical cases had been found annually (Fält et al. 2006, Waldeck 2018), and in 2019, there were 13 registered cases (2020).
Suspected subclinical infections of TBEV have also been described in people with previous tick-bites and suspected tick-borne diseases in the same area (Fält et al. 2006, Lindblom et al. 2014), and in a risk area in the nearby region of Blekinge (Stjernberg et al. 2008). In the Åland islands (located between Sweden and Finland), considered as high incidence areas for TBE, a large number of subclinical cases are suspected since 5% of blood donors have IgG antibodies against TBE (Wahlberg et al. 2006), and in eastern parts of Russia, TBEV strains of the Far-Eastern subtype are suspected to cause milder forms of the disease (Belikov et al. 2014).
Because of the increasing concern of TBE in Skåne, we wanted to investigate the prevalence and levels of TBEV antibodies among people visiting health care centers in different rural areas, and among people in Skåne who self-report to often get tick bites, to get a better estimation of how common undiagnosed disease is, and also to get an idea of the coverage of vaccination in different populations since there are no vaccination registers in Sweden.
Materials and Methods
Serum samples
Serum samples were collected in 2017 in southern Sweden (Skåne County). The group of anonymous individuals in rural areas (AIRA) were collected from mid-July until mid-August 2017. The tick-bitten individuals (TBI) were collected from July to October 2017. Serum samples were collected in BD Vacutainer SST II Advance-tubes REF 366566 (Becton Dickinson Co). All samples were stored at −80°C.
Anonymous individuals in rural areas
These samples were obtained from individuals seeking medical care in primary health care centers. The selection was made in the hospital laboratories of Kristianstad and Hässleholm based on site of sampling, and neither age nor gender was taken into account. All personal data were eliminated by the laboratory staff before inclusion in the study. The primary health care centers were situated in northern and eastern parts of Skåne: Tyringe, Knislinge, Broby, Bromölla, and Osby. These centers are taking care of a general patient clientele without any specific considerations regarding gender, age or diseases, and they are located in relatively rural areas where some of the areas have had most of the clinical TBE cases in Skåne (Knislinge, Broby, and Bromölla).
Tick-bitten individuals
This group consisted of volunteers who according to themselves “often received tick-bites” and actively wanted to participate. They were recruited through public advertising and information to associations of orienteers. Information about the study participants such as age, gender, residence, and previous TBEV-vaccination was collected in a questionnaire.
Ethics
The study was ethically approved by the Regional Ethics Board in Lund, Sweden (reference 2017/177) and by the Regional Board for Quality Register (S-KVB). Informed consent was obtained from the participants.
Assay for TBEV IgG and IgM
The serum samples were analyzed for TBEV IgG and IgM in the routine laboratory of Clinical Microbiology, Lund University Hospital, during two different days in 2018. The test used was an enzyme-linked immunosorbent assay (ELISA) from Euroimmun AG, Germany. The cutoff for a positive test was set to ≥20 RU/mL for IgG, and for IgM, an index of ≥1.1 was considered positive, 0.8 to <1.1 was regarded as borderline positive, and <0.8 was negative.
Neutralization test
TBEV neutralization test (NT) was performed by the Public Health Agency of Sweden (Folkhälsomyndigheten), according to Vene et al. 1998, and a titer of ≥5 was regarded as positive. This test does not respond to vaccinations or infections by other flaviviruses. A positive response in this test indicates that the patient has had a TBEV infection if he/she has not been vaccinated against TBE. The test as such cannot clearly differ between a prior infection and a vaccination though (Baldovin et al. 2012, Albinsson et al. 2018).
Statistics
Analyses were performed with SPSS version 19.0 software (SPSS, Inc., Chicago, IL). P-Values were calculated with two-samples t-test when comparing different means of IgM and IgG between geographically and age-divided populations. The chi-squared statistical test was used to compare the results of the seropositive cohorts in percentages. A p value of <0.05 was considered as statistically significant.
Results
AIRA: geographical profile and comparison
In total, 491 samples were collected from five different primary health care centers in Northern Skåne County (Fig. 1). When analyzing the IgM-index, three samples were positive for TBEV (0.6%) and three samples had borderline results (0.6%). For IgG, 27 individuals (5.4%) were positive.
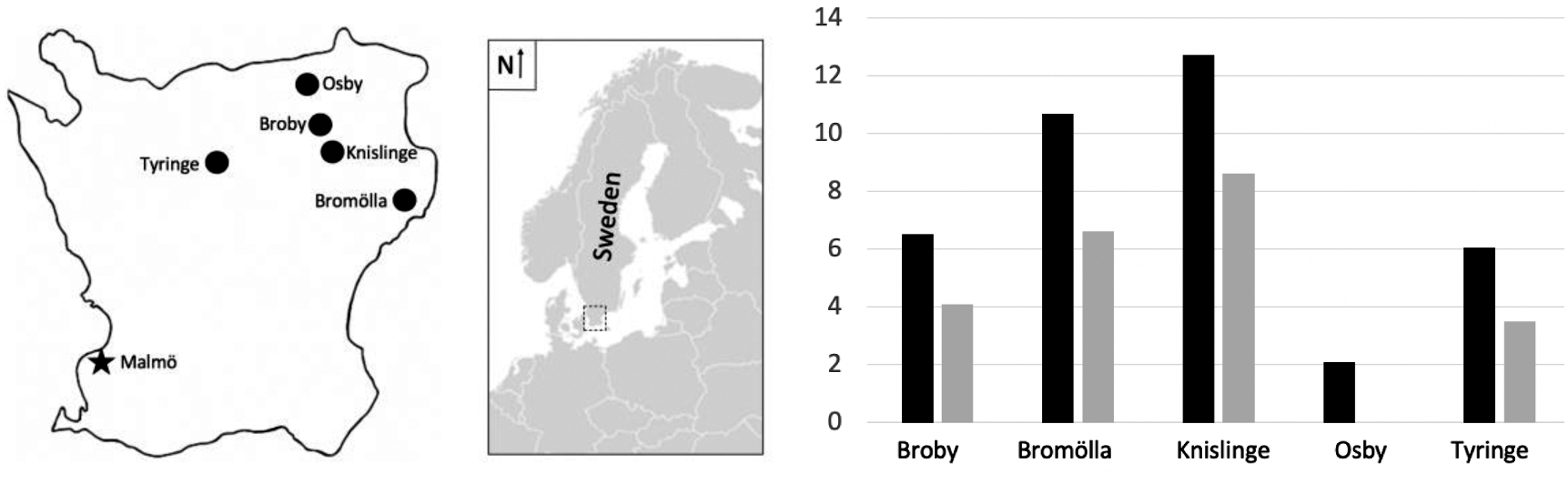
Left: geographical location of sampling in the northeastern part of the Skåne County for the AIRA group. Right: results in the AIRA group for means of IgG in black bars (RU/mL) and seropositive proportions (%) in gray bars, divided into different geographical areas. AIRA, anonymous individuals in rural areas.
The overall mean and median for the IgM-indices were 0.09 and 0.05. Since the IgM indices in general were very low, no further comparisons were made.
The overall IgG seropositivity was 5.3%, ranging from 0% to 8.6% in different geographical locations (Fig. 1). There was no significant differences between the locations. The overall mean and median for IgG was 8.6 and 2.0 RU/mL, respectively. The mean values for the different locations were compared and differences were found when Bromölla (IgG = 10.7 RU/mL, n = 152), Knislinge (IgG = 12.7 RU/mL, n = 105), and Tyringe (IgG = 6.1 RU/mL, n = 142), which all had higher values, were compared with the lower mean value in Osby (IgG = 2.1 RU/mL, n = 44). Broby had a mean value in between of IgG 6.5 RU/mL (n = 48). Statistically significant differences between the IgG means were also found between Bromölla and Osby (p = 0.001), between Knislinge and Osby (p = 0.006), and between Tyringe and Osby (p = 0.002) (Fig. 1).
Tick-bitten individuals
Hundred ninety-eight individuals volunteered. The overall TBE vaccination coverage in the TBI group was 45% according to the study questionnaires. Ninety-two individuals were vaccinated, 99 were unvaccinated, and 9 had no or unclear response to prior completed vaccination.
When the IgM-indices were measured, two samples were positive for TBEV (1%) and three samples had borderline results (1.5%). The overall mean and median for the IgM-indices were 0.12 and 0.07, respectively, and due to the low values, no further comparisons were made.
For IgG, 57 individuals (28%) were positive. The overall mean and median for IgG were 28.2 and 4.0 RU/mL, respectively. IgG means for vaccinated and unvaccinated were 55.5 and 3.7 RU/mL, respectively (p value <0.001) (Fig. 2). The TBI group was further divided into three age cohorts with IgG means of 37.3 RU/mL in the youngest group (<50 years, n = 68), while the middle-aged group (50–69 years, n = 86) had a considerably lower mean level of IgG, 19.2 RU/mL (p = 0.018 compared with the group <50 years). The oldest individuals (>69 years, n = 44) had an IgG level of 34.2 RU/mL. There was no statistically significant difference in vaccination coverage between the age groups: 44% in the youngest, 44% in the middle-aged, and 55% in the oldest, respectively.

The TBI groups was divided into different age groups, and IgG means (RU/mL) for unvaccinated and vaccinated (gray and black bars, respectively) are shown as well as seropositie percentages (diagonal striped bars). For comparison, to the far right, the AIRA group's IgG mean (RU/mL; dotted bar, unknown vaccination status) and the seropositie percentage (diagonal striped) is shown. TBI, tick-bitten individuals.
Within the TBI group, there was a similar distribution between men and women and no significant differences according to sex for means of IgM indices or IgG levels (IgG means was 58.5 RU/mL for men and 54.5 RU/mL for women). Forty-four percent of females and 57% of males were vaccinated and had completed the vaccination program.
The IgG mean value for the TBI group was significantly higher compared to the AIRA group (p value <0.001).
Neutralization test
In the TBI group, six individuals had positive or borderline values for IgM or IgG, despite that they had reported not to have been vaccinated (Table 1, ID 1–6). Samples from these individuals were analyzed using a TBEV NT, and we found two individuals who had positive results (which they were informed about according to the study protocol).
Results of Neutralization test
In the Tick-Bitten Individuals Group, Sample ID 1–6, the Individuals with Elevated or Borderline Results in the Antibody Assays for IgG/IgM and Without Previous Tick-Borne Encephalitis-Virus Vaccination, Were Analysed Using Neutralization Test. Two samples were found to be positive (cutoff is ≥5), indicating earlier nonvaccine exposure to the virus. In the AIRA group, sample ID 7–12, the individuals with elevated or borderline IgM index results, were analyzed using NT. ID 12 was found with a very high NT titer, >160.
AIRA, anonymous individuals in rural areas; limit, borderline; n/a, no available information; neg, negative; NT, neutralization test; pos, positive; TBEV, tick-borne encephalitis virus.
In the AIRA group, the vaccination status was unknown, but the samples that were positive or borderline for IgM were analyzed using the NT (Table 1, ID 7–12). ID 12 was found to have a clearly elevated titer of >160.
Discussion
In this serosurvey among two cohorts in southern Sweden, we found a considerable number of individuals with elevated levels of IgG and a few with elevated IgM-indices. In the AIRA group, sera from AIRA were investigated. In some of the areas, an accumulation of clinical TBE cases have been seen in the past, for instance, in the areas around Knislinge and Bromölla, while Osby and Tyringe have been more spared from the disease (Fält et al. 2006, Waldeck 2018).
We found a significantly higher levels of IgG in Bromölla, Knislinge, and Tyringe areas compared to the Osby area. This could indicate higher vaccination coverage in these areas, perhaps affected by publicity around earlier cases. Many of the primary health care centers in these areas offer TBE vaccinations. A limitation is here, of course the small study groups, but since there are no vaccination registers in Sweden, it is of interst. It is noteworthy that even if there has been known cases of TBE in the area, the total prevalence of IgG antibodies in the area was only 5.3%, indicating that vaccine coverage in general is quite low. IgG levels after a vaccination have before been shown to persist for at least a couple of years (Albinsson et al. 2018).
In the cohort of previous TBI, 45% of the participants had been vaccinated. Even though there are no registers to show how accurately they have followed the rather frequent vaccination program (three vaccinations during the first year, followed by a booster vaccination every 3–5 years depending on age), these individuals have stated that they have been vaccinated, and it seems plausible since they are people who frequently move around in areas where there are many ticks, and their knowledge about the disease might be better compared to the average population. However, only 28% showed presence of IgG antibodies, indicating that the levels drop after a couple of years. Another limitation is the lack of information about other flavivirus infections in the medical history, or more likely, previous vaccinations against those viruses, even if most of them are not of immediate relevance in a Northern European perspective. Crossreactivity could occur in the ELISA we have used if a very recent infection (or vaccination) had occurred, but not in the NT (Maeki et al. 2019). Even if vaccination against Yellow Fever had occurred, most individuals would not react in the TBEV ELISA (Allwinn et al. 2002).
Regarding the individuals in the different age groups (Fig. 2), the middle-aged group of 50–69 years had lower levels of IgG. This may be explained by a lower exposure to TBE from tick-bites, as well as lower immunoglobulin-levels. Adding this to the fact that the oldest individuals (>69 years) had a higher vaccination frequency (55% compared with 44% in the other two groups), this could explain our results. Other studies have shown that older people (>60 years) develop lower levels of IgG (Lock and Unsworth 2003) and vaccinees 50–90 years of age develop lower IgG levels (Weinberger et al. 2010).
Six individuals who denied previous TBEV vaccination, but showed either positive/borderline IgM-index or positive for IgG, were followed up with a NT. Two individuals (Table 1, ID 1 and ID 4) were positive in NT with relatively low titers. Symptoms of TBE may in the first viremic stage include fever and general malaise, but in the second phase, the central nervous system could be affected and high age seems to be a risk factor for developing more severe forms of TBE (Gustafson et al. 1992, Hunfeld et al. 1998, Cizman et al. 2000, Gunther and Haglund 2005).
Another study participant from the AIRA group (Table 1, ID 12) had a very high NT value of >160 and was included from the area of Knislinge. This result could be due to a relatively recent case of TBE, since this individual had high levels of IgG and also a positive result for IgM antibodies. However, because it is from an anonymous study participant, we do not know if this probable case may have been diagnosed or not. In total, five cases of TBE were confirmed in the whole region of Skåne, during the sampling period. We cannot exclude the possibility that this is one of these cases, but it could also be an undiagnosed case with a patient seeking medical care due to symptoms not correctly diagnosed.
Despite the fact that some serological elevations seen in our study may be caused by previous vaccinations and may also have been affected by analytical or immunological cross reactivity after vaccinations against other flaviviruses, there is also the suspicion of subclinical or asymptomatic TBE cases. This has been described in studies from southern Sweden (Fält et al. 2006, Stjernberg et al. 2008) as well as more northward in Sweden and Finland and even stated to be rather common (Gustafson et al. 1992, Wahlberg et al. 2006). One study from Slovenia in an area which was endemic for tick-related infections such as Borrelia burgdorferi sensu stricto, and where children and young adults were investigated, 4% had elevations of TBEV IgG (Cizman et al. 2000). A study of Lyme borreliosis patients and control groups in midwestern Germany showed 1% of TBEV IgG seroreactivity (Hunfeld et al. 1998).
Our serological results showed a total IgG seroprevalence of positives with 5.3% from the AIRA group. Another serological investigation from southern Sweden showed that 7.1% had elevated levels of IgG (Fält et al. 2006). But these samples were collected among people with a clinical suspicion of tick-borne disease in an area overlapping with where the samples from our AIRA group was collected. In a limited tick endemic area on a small island in south-eastern Sweden, 8.3% were IgG seropositive (Stjernberg et al. 2008). This can be compared to our TBI group where 28% had positive values for IgG, although in this group, we believe that vaccinations are the main reason for the high seroprevalence.
Our findings show different levels of TBEV antibodies in different geographical locations. The risk areas of TBE based on previous clinical cases are considered to be very scattered in Skåne (Waldeck 2018). Both these facts are also corresponding to the observations that the pattern of geographical spread includes new areas being discovered. Reasons are probably multifactorial, even if climate and environmental causes definitely seem to be involved (Lindgren and Gustafson 2001, Gunther and Haglund 2005).
A country which has been affected considerably by TBE infections is Austria. They have noticed a major geographical shift. In the 1970s big numbers of clinical cases were seen in the lowland regions, while in later decades a substantial number of cases have appeared in the mountain regions. One explanation has been proposed to be raised temperatures, especially during springtime. Austria has managed to fight the overall increase of TBE cases using vaccine campaigns (Heinz et al. 2015). Other European countries that have had high numbers of cases are Russia and Germany, The Czech Republic, Slovenia, Poland, and the Baltic countries (Lindquist and Vapalahti 2008).
Conclusion
Overall, our study shows major differences in TBEV IgG between different groups of people. We found high IgG levels both in areas previously considered as risk areas and in other areas. This could not only be due to different vaccination coverage but also due to differences in immune response for different age groups. Among anonymous samples, the seroprevalence was 5.3%, but in a group who often got tick-bites and where the awareness of vaccination was probably high (45% self-reported as vaccinated), the seroprevalence was 28%. Our results motivate an increased awareness of TBE in southern Sweden. TBEV vaccination should be considered for people who are often outdoors in risk areas.
Footnotes
Authors' Contributions
J.S. was responsible for collection of the samples and wrote the article, K.E.M.P. was main supervisor, and J.S., C.B.C., and K.E.M.P. together planned the outline of the study and helped with writing the article.
Acknowledgment
We are grateful to the participants and the funders of the study.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This study was supported by grants from the governmental Avtal om Läkarutbildning och Forskning (ST-ALF), ALF and ALF Innovation grants to the university health care in Region Skåne, Alfred Österlunds Stiftelse and Crafoordska Stiftelsen.