
Abstract
Ticks transmit pathogens and parasitize wildlife in turn causing zoonotic diseases in many ecosystems. Argasid ticks, such as Ornithodoros spp., harbor and transmit Borrelia spp., resulting in tick-borne relapsing fever (TBRF) in people. In the western United States, TBRF is typically associated with the bite of an infected Ornithodoros hermsi tick found in habitats at high elevations (>1500 ft). This report describes the first TBRF cases in people in the Mojave Desert (Clark County, NV). Individuals documented in these case studies were exposed to Ornithodoros ticks during excavation of soil burrows associated with Mojave Desert tortoises (Gopherus agassizii), with bacteria from one of the human case's blood sample genetically matching to Borrelia turicatae as determined by quantitative PCR and sequencing. Our findings should serve as a precaution to individuals working with tortoises or animal burrows, or those in contact with Ornithodoros ticks in this region.
Introduction
Ornithodoros tick vectors of the causative agents of tick-borne relapsing fever (TBRF) (Borrelia hermsii and others) are widely distributed throughout the Mojave Desert; however, human cases of TBRF have yet to be documented in this region (Greene 1985, Donaldson et al. 2016). Most reported cases of TBRF in the western United States are caused by B. hermsii, the spirochete pathogen transmitted by Ornithodoros hermsi ticks, found primarily in forested habitats at high elevations (between 450 and 2400 m) (Forrester et al. 2015).
Reviews of TBRF cases in the western United States largely focus on TBRF cases caused by B. hermsii, and rarely mention cases involving the two remaining Ornithodoros species involved in the epidemiology of TBRF in other geographic regions of the country, namely O. parkeri and O. turicata and their respective Borrelia species (B. parkeri and B. turicatae) (Forrester et al. 2015, Osborne et al. 2019). O. parkeri and O. turicata are found in low elevation habitats across the southern portion of the country and have been identified in association with animal burrows in the Mojave Desert (Greene 1985, Donaldson et al. 2016). In the Mojave Desert, Ornithodoros ticks have not been reported in the transmission of TBRF in people, despite being competent vectors of TBRF group Borrelia (Berry and Christopher 2001). In this study, we report the first cases of TBRF disease contracted from Ornithodoros ticks associated with desert tortoise burrows in the Mojave Desert.
Borreliosis Transmission and TBRF Associated with Tortoise Burrows
Two adult individuals with TBRF linked to activities including handling tortoises and excavating their burrows in Clark County, NV, are described in the following cases: Case 1 (Universal Transverse Mercator coordinates: 680518 E, 4045986 N)
To identify the spirochete species, we sequenced a ∼650 bp portion of the 16S–23S intergenic spacer (rrs-rrlA, IGS) of the qPCR-positive sample (Bunikis et al. 2004). The sequence was then compared with other Borrelia sequences available from GenBank using BLAST (
Case 2 (Universal Transverse Mercator coordinates: 657645 E, 3983051 N)—In November 2018, also in Clark County, NV, a second biologist was bitten by an Ornithodoros spp. tick after handling captive tortoises and excavating burrows with notable numbers of ticks (200+) present and subsequently contracted TBRF. Ornithodoros ticks were observed on his clothing and equipment throughout the day and he reported a small, pruritic, dark and raised mark on the right hip described as sore and sensitive to touch (Fig. 1). The mark increased in size, developing a darker ring around the outer edge and remained visible for ∼30 days. The lesion healed completely without scarring. The individual reported three periods of febrile/afebrile cycles (relapses) with symptoms including high fever (103–105°F), muscle aches, and body chills that first appeared a week after the initial tick bite.
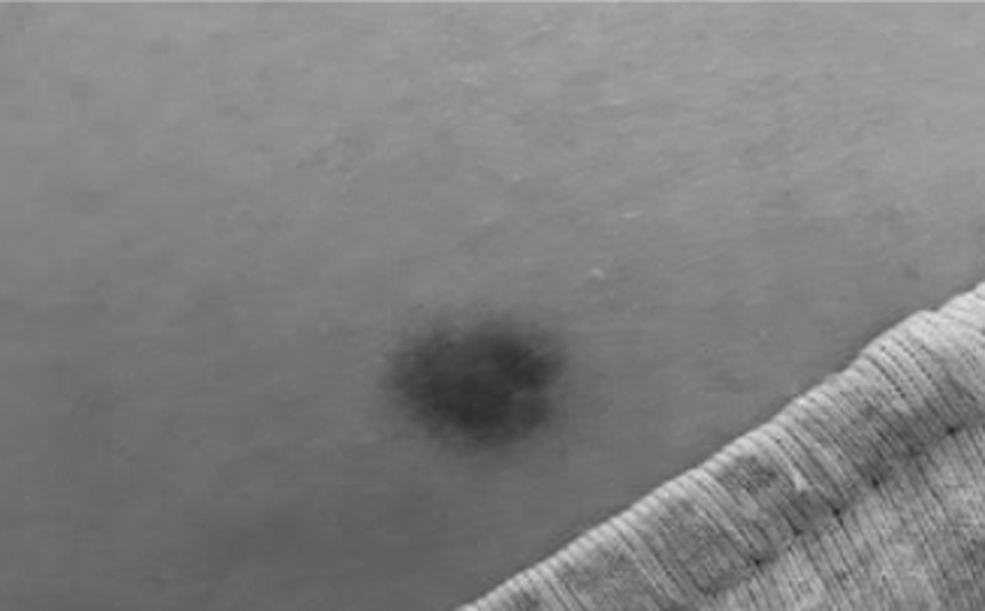
Picture of possible tick bite taken by Case 2 patient. Patient noticed this raised mark on his right hip that was sore and sensitive to touch after exposure to Ornithodoros ticks while digging up captive desert tortoise burrows.
The first febrile cycle began 7 days after tick bite and lasted for 3 days, followed by a short afebrile period of 2 to 3 days duration without symptoms. A second symptomatic febrile cycle that lasted 3 days was again followed by an afebrile period of 2 to 3 days without symptoms. The subsequent third febrile cycle, and reportedly the most severe relapse, resulted in a fever of 105°F and prompted the patient to visit an emergency medical facility in Clark County, NV, for clinical evaluation and diagnosis. Blood smears indicated TBRF Borrelia spp. spirochetes present in circulating blood and IgG/IgM enzyme-linked immunosorbent assay (ELISA) diagnostic tests confirmed the presence of antibodies specific to Borrelia spp. Genetic characterization of TBRF Borrelia species was not performed in the case. The patient was treated with an antibiotic (doxycycline) and recovered without subsequent relapses.
Discussion
TBRF is endemic in the western United States (Schwan et al. 2009); however, little is known about its vectors or wildlife reservoirs in the Mojave Desert. Two tick species, O. parkeri and O. turicata, are common ectoparasites for tortoises and other desert wildlife and are responsible for transmitting their respective TBRF Borrelia spp. in other parts of North America (Greene 1985, Lopez et al. 2016). Both tick species are nidicolous and spend the majority of their lives in nests and burrows of their vertebrate hosts (Sonenshine and Roe 2014). In fact, both Ornithodoros species have been found in desert tortoise burrows, which likely provide suitable microenvironments in a harsh xeric landscape.
TBRF should be considered as a potential disease for people in the Mojave Desert with related symptoms. Hospitalizations occur frequently in TBRF patients, evidenced by case reports in Washington and California stating that 46–80% of infected patients required admission to hospitals (Schwan et al. 2009). In fact, our Case 2 patient was discouraged from receiving a confirmatory ELISA test as medical professionals did not think that TBRF was likely a risk in this area. A surveillance study of the tick species and the Borrelia pathogens they may carry in the areas where these cases have occurred is currently ongoing. We posit that TBRF transmission in the Mojave Desert, as in other regions, is likely underreported and may be a larger human health risk than previously understood.
Conclusion
TBRF cases may increase as human recreation and development continue to encroach on native desert ecosystems. Ornithodoros ticks are commonly found within animal burrows and on tortoises in the Mojave Desert. As such, pet owners, biologists, and enthusiasts working with tortoises or individuals in contact with Ornithodoros ticks in this region should be aware of the associated TBRF symptoms. Experienced medical staff and available diagnostics are limited in regions such as the Mojave Desert, because TBRF has not been documented as a potential risk in the area. Additional research and accurate case diagnoses will improve our understanding of this disease and may enhance our public health strategies, including widespread ability to treat and diagnose patients who may have contracted TBRF in the Mojave Desert region.
Footnotes
Acknowledgments
We thank our colleagues for continued discussion on this topic and to D. Salkeld for reviewing and improving this short communication. Any use of trade, product, or firm names is for descriptive purposes only and does not imply endorsement by the U.S. Government.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
We also acknowledge funding support provided by the Pacific Southwest Center for Excellence in Vector-Borne Disease funded by the U.S. Centers for Disease Control and Prevention (Cooperative Agreement: 1U01CK000516), which has allowed us to write this short communication.