
Abstract
Background:
Brucellosis is the most common zoonotic infection worldwide, and is caused by bacterial genus Brucella. The disease is rarely transmitted through human-to-human transmission. Few cases have been reported about vertical transmission of human brucellosis. Herein, we reported a case of congenital brucellosis, with clear evidence of pathogen detected in mother's placental specimen.
Case Presentation:
A 34-day-old girl was admitted to the department of pulmonology with fever for 8 days. Three blood samples and one sample of cerebrospinal fluid were positive for Brucella melitensis. The diagnosis of brucellosis and B. melitensis meningitis were established, along with hyperbilirubinemia and liver dysfunction. Treatment of rifampicin (for 6 weeks) and meropenem (for 2 weeks) was administered. However, the disease relapsed within 18 days. Thereafter, a combination therapy of rifampicin and sulfamethoxazole/trimethiprim (SMZ/TMP) was administered for 8 weeks. The disease relapsed again in 42 days. For chronic brucellosis, three courses of combination therapy of rifampicin and SMZ/TMP was administered. The mother had fatigue and arthralgia for 2 weeks, fever and membrane rupture 1 day before the baby was born. B. melitensis DNA was detected in the mother's placental specimen by next-generation sequencing and bacterial identification under microscope proved chorioamnionitis.
Conclusions:
We reported a confirmed case of congenital brucellosis. This disease should be closely monitored even in nonepidemic areas. The treatment of brucellosis in infancy faces challenges of drug choice and disease relapse.
Introduction
Brucellosis is the most common zoonotic infection worldwide, and is caused by bacterial genus Brucella (Hasanjani Roushan and Ebrahimpour 2015). There are half a million new cases annually in some countries (Franco et al. 2007). Zhejiang is not an endemic province, and no infection has occurred during 1983–2003. However, rare cases occurred after 2003. Symptoms of brucellosis are fever, arthralgia or arthritis, night sweats, asthenia, insomnia, anorexia, and headache. Physical examination reveals hepatomegaly and splenomegaly, lymphadenopathy, osteoarticular manifestations, genitourinary complications, neurological findings, mucocutaneous manifestations, and pulmonary manifestations.
The disease is transmitted through consumption of unpasteurized dairy products, direct contact with infected animals, inhalation of contaminated aerosols, and rarely human-to-human transmission (Hassouneh et al. 2019). Although intrauterine transmission, transmission during delivery, and transmission through breast milk are among the main routes of transmission in the mammalian reservoirs, few cases have been reported about vertical transmission of human brucellosis (Zhao et al. 2019; Palanduz et al. 2000; Giannacopoulos et al. 2002). Herein, a congenital brucellosis case was reported. This helps to provide a scientific basis for the prevention and control of brucellosis in pregnant women and their newborn babies.
Case Presentation
A 34-day-old girl was admitted to the department of pulmonology with fever from day 26. The peak body temperature was 37.6–37.7°C. She was born to a Chinese 25-year-old G1P0 at 37 weeks 4 days' gestation (3300 g birth weight without resuscitation). Her mother had visited and stayed for several periods in her parents' house, where 20 sheep were once kept. Although she had never fed or touched those sheep, the mother had fatigue and arthralgia for 2 weeks, fever and membrane rupture 1 day before the baby was born. Considering that the mother might have been experiencing chorioamnionitis, which was later confirmed by pathology, the baby was delivered by cesarean section. The baby was fed with mother's milk for 4 days until the mother's blood culture revealed a positive result of brucellosis. The mother was immediately started on 6 weeks' course of rifampicin and doxycycline. A screening of Rose Bengal plate test among her family showed that the mother's father was also positive and symptomatic, whereas other family members were negative. The grandfather had fatigue, arthralgia, and low-grade fever for 4 months, but did not seek medical help. He had killed and sold all the sheep because of his fatigue and arthralgia before the baby was born.
The baby's father took her to the pediatric department at another hospital on the third day of fever, where acute upper respiratory tract infection was diagnosed and she was observed for one night. Blood samples were obtained for blood culture and Rose Bengal plate test. The baby's body temperature returned to normal on the second day, so she was discharged. However, fever returned after 3 days of normal body temperature. This time, she was agitated and often cried. She had a peak body temperature of 37.7°C, once a day. Her father immediately brought her to our hospital. She was admitted to the department of pulmonology after a short examination at the outpatient clinic, without any laboratory test or therapy. On physical examination, the girl was febrile (37.6°C), with heart rate 144 beats/minute, respiratory rate 34/min, blood pressure 74/43 mm Hg. She appeared acutely ill but nontoxic. Her oral mucosa was normal. Her lungs were clear in auscultation. Her abdomen was not distended. Liver and spleen were not palpable below the costal margin. Her joints were all normal. Findings of neurological and dermatological examinations were normal.
On the second day, the girl continued to have fever. The highest body temperature was 38.2°C. Moreover, she seemed lethargic. Bacterial meningitis was suspected and lumbar puncture was performed. The cerebrospinal fluid (CSF) contained 85 leukocytes/μL (86% mononuclear cells), with a protein level of 102.6 mg/dL and a glucose level of 40 mg/dL. The local hospital reported positive blood culture for Brucella melitensis and positive Rose Bengal plate test. Culture of two samples of blood and one sample of CSF also showed positive for B. melitensis (Fig. 1). The diagnosis of brucellosis and B. melitensis meningitis were established, along with hyperbilirubinemia and liver dysfunction. Since sulfamethoxazole/trimethiprim (SMZ/TMP) is forbidden for use in children <2 months according to its drug directions, we started treatment of rifampicin (for 6 weeks) and meropenem (for 2 weeks).

Blood culture showed positive for Brucella melitensis (Gram stain, 1000 × ).
Her body temperature returned to normal within 2 days of treatment but reoccurred on day 18 after discontinuing rifampicin. Laboratory tests, including positive blood culture with B. melitensis, positive Rose Bengal plate test, and >1:400 in serum agglutination test of brucellosis, suggested relapse of brucellosis. A combination therapy of rifampicin and SMZ/TMP was immediately started for 8 weeks. Her body temperature returned to normal on the third day.
She was normal for 42 days after which she became febrile and had positive blood culture for B. melitensis. The disease lasted for >6 months altogether, suggesting chronic brucellosis. So three courses of combination therapy of rifampicin and SMZ/TMP for 6 weeks each with 1 week's interval were started. Her body temperature returned to normal from the second day of therapy. At present, she is 10 months old, and is in the third course of chronic brucellosis therapy (Fig. 2). In the later two relapses, she also had liver dysfunction. However, besides fever, she had no other sign or symptom. Her liver function reverted to normal in 1–2 weeks after therapy every time. Results of brain magnetic resonance imaging, electroencephalogram, and ultrasonic sound of heart, liver, spleen, kidneys, uterus, and ovaries were normal.

The timelines of diagnosis and management.
B. melitensis DNA was detected in mother's placental wax specimen by next-generation sequencing and bacterial identification under microscope (Fig. 3) suggested that this was a congenital brucellosis case.
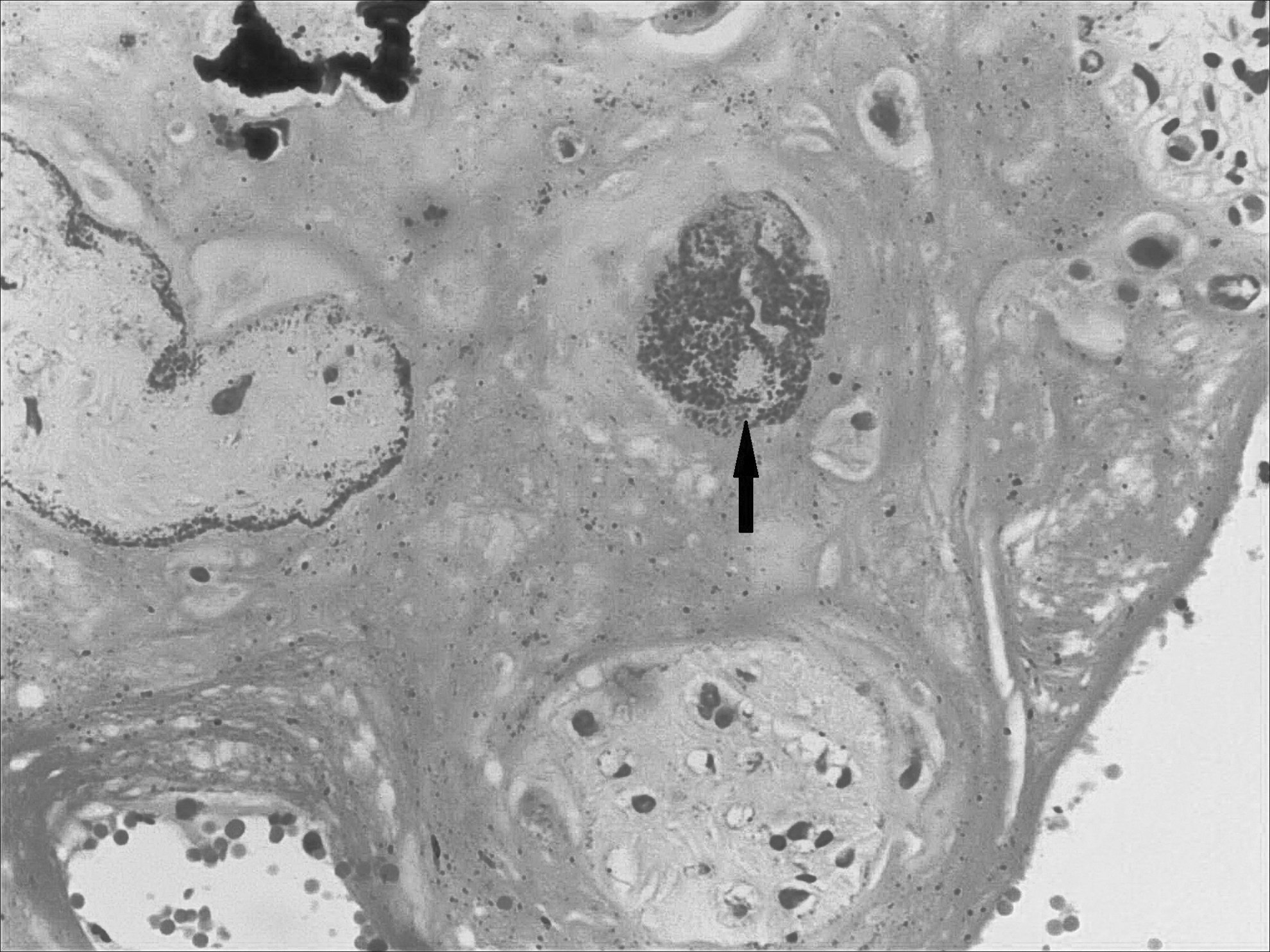
HE staining (400 × ) shows clusters of coccobacilli in the connective tissue of chorioamnion (arrow).
Discussion and Conclusions
Before first acute brucellosis case in 1983, Zhejiang kept zero in incidence for about 20 years (Xu et al. 2007). After that, incidence and prevalence of brucellosis in Zhejiang has been increasing slightly (Xu et al. 2007; Yang et al. 2020). The incidence was 0.18/100,000 in Zhejiang in 2015 (Shi 2017). There are many reasons for the increase. First, the prevalence of brucellosis in humans mainly depends on the epidemic situation in animals. Prevalence increased of brucellosis both in human and animals in northern China at the same period. Second, an increasing demand of meat and milk increased introduction of northern livestock and also the risk of people's exposure to contact with raw lamb or beef. Third, insufficient quarantine immunity may also increase the epidemic intensity of the disease in Zhejiang (Xu et al. 2007; Yang et al. 2020).
Alsaif et al. (2018) systematically reviewed 44 cases of congenital brucellosis dating back to 1941. Among these cases, only one infant had cord blood bacteremia, which was clearly congenital. Other cases were diagnosed mainly based on positive blood culture from 1 day to 3.5 months, in which seven cases had mothers infected with brucellosis during pregnancy. We described a case of congenital brucellosis with clear evidence of intrauterine transmission. In our case, positive blood culture in mother suggested the mother's infection. Positive blood and CSF culture, and serological results suggested baby's infection. There is a small chance that transmission also occurred from breast milk even though the infant was only breastfed for 4 days. However, chorioamnionitis, bacterial identification by microscopy, and B. melitensis DNA detected in the mother's placental specimen established the diagnosis of congenital brucellosis. The incubation period of brucellosis is usually between 1 and 3 weeks. In our case, the baby had symptom onset on day 26.
The World Health Organization has not updated its recommended treatment regimens for brucellosis in >30 years (No authors 1986). The Ministry of Health of the People's Republic of China (2012) released a 2012 version of “Guidelines for diagnosis and treatment of brucellosis (Trial)” in Chinese. The clinical management of brucellosis is challenging because of high initial treatment failure and relapse rates (Franco et al. 2007). The treatment failure and relapse rates range from 4.6% to 24% for the oral regimen and 5–8% for the oral/parenteral regimen (Franco et al. 2007). The independent predictors of relapse were temperatures of ≥38.3°C, positive blood cultures at baseline, and a duration of symptoms before treatments of <10 days (Solera et al. 1998).
In this case, we had difficulty in choosing the antibiotics because of the patient's age. According to the Chinese version of guidelines (Ministry of Health of the People's Republic of China 2012), the recommended drugs are rifampicin plus SMZ/TMP for children aged 6 weeks and older. There is no guideline for children aged 6 weeks and younger. Moreover, SMZ/TMP is forbidden for use in children <2 months according to its drug directions. The baby was only 34 days old. Moreover, she had positive skin tests to penicillin and cephalosporin. So in the first course, we chose rifampicin (for 6 weeks) and meropenem (for 2 weeks). Meropenem was previously used in some cases of brucellosis (Ay et al. 2018; Mohzari et al. 2020). In children, rifampicin monotherapy can be used but is not recommended, because it is associated with a high relapse rate (Khuri-Bulos et al. 1993). The disease relapsed only 18 days after discontinuing rifampicin. Her parents were disappointed. She was 3 months old at that time. Extending the antibiotic treatment helps to prevent relapse (Franco et al. 2007). So we administered rifampicin and SMZ/TMP for 8 weeks for the second time. The disease relapsed again after 42 days. For chronic brucellosis, three courses of combination therapy of rifampicin and SMZ/TMP were administered.
In summary, we reported a confirmed case of congenital brucellosis. This disease should be closely monitored even in nonepidemic areas. The management of brucellosis in infancy faces the challenges of drug choice and disease relapse.
Footnotes
Authors' Contributions
D.X. designed the study and drafted the article. X.L., B.C., Y.Z., M.Z., and W.G. collected the clinical data and participated in data analysis. Y.W. and Z.C. coordinated all the work related to the study and revised the article. All the authors read and approved the final article.
Acknowledgments
We thank all colleagues in the department of clinical laboratory at our hospital.
Ethical Statement
This research was conducted according to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Children's Hospital, Zhejiang University School of Medicine (2020-IRB-152). No animal work was carried out as part of this study.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.