
Abstract
Objective:
The aim of this study is to describe the main clinical phenotypes, laboratory findings, and severity of coronavirus disease 2019 (COVID-19) in patients hospitalized at the High Specialty Medical Unit # 71 of the Mexican Social Security Institute.
Methods:
Prospective observational cohort study with a total of 105 patients hospitalized with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection at the High Specialty Medical Unit # 71 (Torreón, Coahuila, Mexico), from May 15th to August 15th, 2020. The cases were confirmed to be COVID-19 positive through an RT-qPCR test. Clinical phenotypes and laboratory tests were evaluated to determine the degree of severity of the disease and the most frequent comorbidities.
Results:
The clinical characteristics of a total of 105 hospitalized patients (47 females and 58 males; median age being 52 years) with confirmed COVID-19 diagnoses were studied. The severity of the disease was classified as moderate grade (62.7%), severe grade (21.5%), and critical grade (15.6%). Among the most frequent underlying pathologies coexisted overweight (n = 75, 78.12%), obesity (n = 21, 21.87%), diabetes (n = 10, 9.52%), and hypertension (n = 6, 5.71%), some of these patients present more than one pathology. This association was found with diabetes (odds ratio [OR]: 1.42; 95% confidence interval [CI]: 1.23–1.97; p = 0.021) and high levels of D-dimer (OR: 1.01; 95% CI: 1.00–1.08; p = 0.001).
Conclusion:
In this retrospective cohort study of patients with COVID-19 from a specialty hospital in the northeast region of Mexico, it was observed that clinical phenotypes and D-dimer elevation were compatible with an inflammatory state by degree of severity; it was found that the hospitalized patients with underlying chronic medical conditions such as diabetes and elevated D-dimer levels were significantly associated with increased mortality from COVID-19. Age and sex (males) were two factors highly associated with mortality.
Introduction
On March 11, 2020, the World Health Organization (WHO) declared an outbreak of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) a pandemic due to a steady increase in cases outside of China (Organization 2020). Patients with SARS-CoV-2 infection can develop coronavirus disease 2019 (COVID-19), which has resulted in high rates of hospitalization and intensive care unit (ICU) admission (Grasselli et al. 2020a). Critically ill patients with COVID-19 present dyspnea accompanied by hypoxemia, and many of them develop acute respiratory distress syndrome (ARDS), septic shock, and multiple organ failure (MOF) that increase mortality rates (Grasselli et al. 2020a). Symptoms of COVID-19 infection appear after an average incubation time of 5.2 days (Li et al. 2020) and the range between symptom onset and death is between 6 and 41 days with a median of 14 days (Wang et al. 2020b). In its critical stage, COVID-19 presents itself as ARDS, which leads to invasive mechanical ventilation (Grasselli et al. 2020b). Although the epidemiological findings and clinical characteristics of patients with SARS-CoV-2 pneumonia have been described (Chen et al. 2020, Huang et al. 2020, Wang et al. 2020a), the clinical symptoms that define the course of transition from moderate to severe and critical stages are still not clear. Therefore, it is important to identify significant clinical signs or biomarkers that could be predictive of the evolution toward the stages with high mortality. This study aims to describe the clinical and biochemical characteristics in the moderate, severe, and critical stages of COVID-19 in hospitalized patients with SARS-CoV-2 infection admitted in the High Specialty Medical Unit # 71 of the Mexican Institute of Social Security located in northeast Mexico.
Materials and Methods
Study design and participants
In this prospective study of an observational cohort from a single hospital center, patients admitted from May 15th to August 15th, 2020, were consecutively recruited in the High Specialty Medical Unit # 71 of the Mexican Institute of Social Security (Torreon, Coahuila, Mexico). This medical unit provides services and receives patients from four neighboring states, as well as local population. For the diagnosis, routine laboratory studies, computed tomographies (CTs) of the thorax, and oropharyngeal and nasopharyngeal swab samples for RT-PCR (real-time polymerase chain reaction) were obtained from suspected patients. The diagnosis of COVID-19 was based on the WHO guide (Ghebreyesus 2020), visualization of clinical manifestations consistent with the infection such as fever and respiratory symptoms, or evidence of pneumonia findings on CT and/or positive PCR result for SARS-CoV-2. The study was approved by the Health Research and Ethics Committee under the registration number R-2020-501026.
COVID-19 classification according to severity of symptoms
According to the severity of their symptoms, subjects were classified into three groups of COVID-19 patients (moderate, severe, and critical) following the guidelines for the diagnosis and treatment of the new coronavirus (2019-nCoV) published by the National Health Commission of China (Wu and McGoogan 2020). The moderate degree of illness was characterized by fever, respiratory symptoms, and presence of radiographic findings. Patients with severe COVID-19 presented one of the following symptoms: dyspnea with respiratory frequency higher than 30 times per minute, oxygen saturation lower than 93%, or quotient PaO2/FiO2 lower than 300 mm/Hg. The critical group presented some of the following symptoms: ARDS or respiratory failure, septic shock, and/or multiple organ dysfunction or MOF.
Data collection
Information on patients with moderate, severe, and critical stage COVID-19 was retrieved from clinical records. Data included demographic characteristics (age and sex), vital signs, disease symptoms, comorbidities, and laboratory tests. ARDS was defined according to the initiative of the European Society of Intensive Care Medicine endorsed by the American Thoracic Society and the Society of Critical Care Medicine (Force et al. 2012).
Statistical analysis
The data were described using median, interquartile range, number (n), and percentage (%). To evaluate the differences among COVID-19 severity groups, the chi-square test (χ2) was used for categorical variables and the Kruskal-Wallis test for continuous variables. Univariate and multivariate logistic regressions were used to find the relationship among risk factors associated with mortality in Mexican patients hospitalized with COVID-19. Statistical significance was determined with a value of p ≤ 0.05. All analyses were performed with STATA 15 statistical software (Stata Corp., College Station, TX). The study was approved by the Health Research and Ethics Committee under the registration number R-2020-501026.
Results
The study population included 105 hospitalized patients, out of which 44% (n = 47) were female and 56% (n = 58) were male (Table 1). As for the classification of severity based on the patients' symptoms, 62.7% were grouped into moderate grade, 21.5% into the severe grade, and 15.6% into the critical grade. The average age was 52 years; statistical significance was found between the degree of severity of the illness and age (p = 0.006). The mean time between the onset of symptoms and hospital admission was 6 days (on a range of 1 to 15 days), while the period from symptom onset to ICU admission was 10 days (IQR, 6–15). Regarding comorbidities, the percentage of patients presenting one or more comorbidities was 44.7% (n = 47). Obesity was the most frequent, with 21.87% (n = 21), followed by diabetes (9.52%, n = 10), other disease (9.52%, n = 10), and hypertension (5.71%, n = 6). It should be noted that diabetes, hypertension, overweight, obesity and other diseases were not statistical significant by degree of severity. The most common symptoms at the beginning of the disease were anosmia (77.10%, n = 81), fever (53.3%, n = 54), dyspnea (39.05%, n = 41), chest pain (38.10%, n = 40), cough (22.86%, n = 22), headache (18.10%, n = 19), arthralgia (13.33%, n = 13), myalgia (12.38%, n = 13), and rhinorrhea (1.92%, n = 2). Dyspnea and rhinorrhea presented significant differences (p = 0.048 and p = 0.026, respectively) by degree of severity (Table 1).
Clinical Phenotypes of Patients Hospitalized with Severe Acute Respiratory Syndrome Coronavirus 2 Infection in the Different Severity Groups of Coronavirus Disease 2019
COVID-19, oxygen saturation Kruskal–Wallis test, median and IQR defined as the range from the 25th percentile to the 75th percentile. Fisher's exact test.
Values in bold indicate statistical significance, p < 0.05.
COVID-19, coronavirus disease 2019; MAP, mean arterial pressure.
Considering the vital signs evaluated at the time of hospital admission—temperature, heart rate, and systolic blood pressure—they did not significantly differ among patients according to the degree of severity, but respiratory rate (p = 0.001), diastolic blood pressure (p = 0.019), and oxygen saturation (p = 0.001) did. Out of the 105 patients included in this study, 91 (86.67%) were discharged and 14 died (13.33%) (Table 1).
Laboratory findings of hospitalized patients with COVID-19 are shown in Table 2. During hospitalization, a decrease in lymphocyte levels (p = 0.003) was observed by degree of disease severity with median levels of 1.4 × 109 cells/L, respectively (Fig. 1). However, the concentration of neutrophils in the critical disease group (median 8.4 × 109 cells/L) was significantly higher than in the moderate disease group (median 5.7 × 109 cells/L) (p = 0.015). Leukocyte, monocyte, hemoglobin, hematocrit, and platelet levels were not significantly different by degree of severity. As for inflammatory mediators, a statistically significant difference was found in D-dimer levels (Fig. 2), which was higher in critical patients compared to those in the severe stage of the disease (858.5 ng/mL vs. 208 ng/mL, respectively) (p = 0.001). Significant differences (p = 0.002) of C-reactive protein concentrations, neutrophils (p = 0.015), lymphocytes (p = 0.003), and ferritin (p = 0.006) were also observed by severity grade (Table 2). Age and comorbidities were the main risk factors associated with severity of illness. As for the univariate regression analysis (Table 3), age (odds ratio [OR]: 1.04; 95% confidence interval [CI]: 1.01–1.08; p = 0.033), male sex (OR: 3.21; 95% CI: 1.05–4.91), diabetes as a comorbidity (OR: 1.42; 95% CI: 1.23–1.97; p = 0.021), and D-dimer level (OR: 1.01; 95% CI: 1.00–1.08; p = 0.001) were the factors that showed a strong association with the risk of mortality due to COVID-19. Interestingly, obesity was one of the main comorbidities in this group of patients, but it was not found to be associated with mortality. After adjusting for significant factors such as temperature, respiratory rate, and oxygen saturation, multivariate analysis showed that the sex factor (male, OR: 3.38; 95% CI: 1.05–5.46; p = 0.027) and D-dimer levels (OR: 1.56; 95% CI: 1.00–1.87; p = 0.002) remained significantly associated with mortality due to COVID-19 (Table 3).
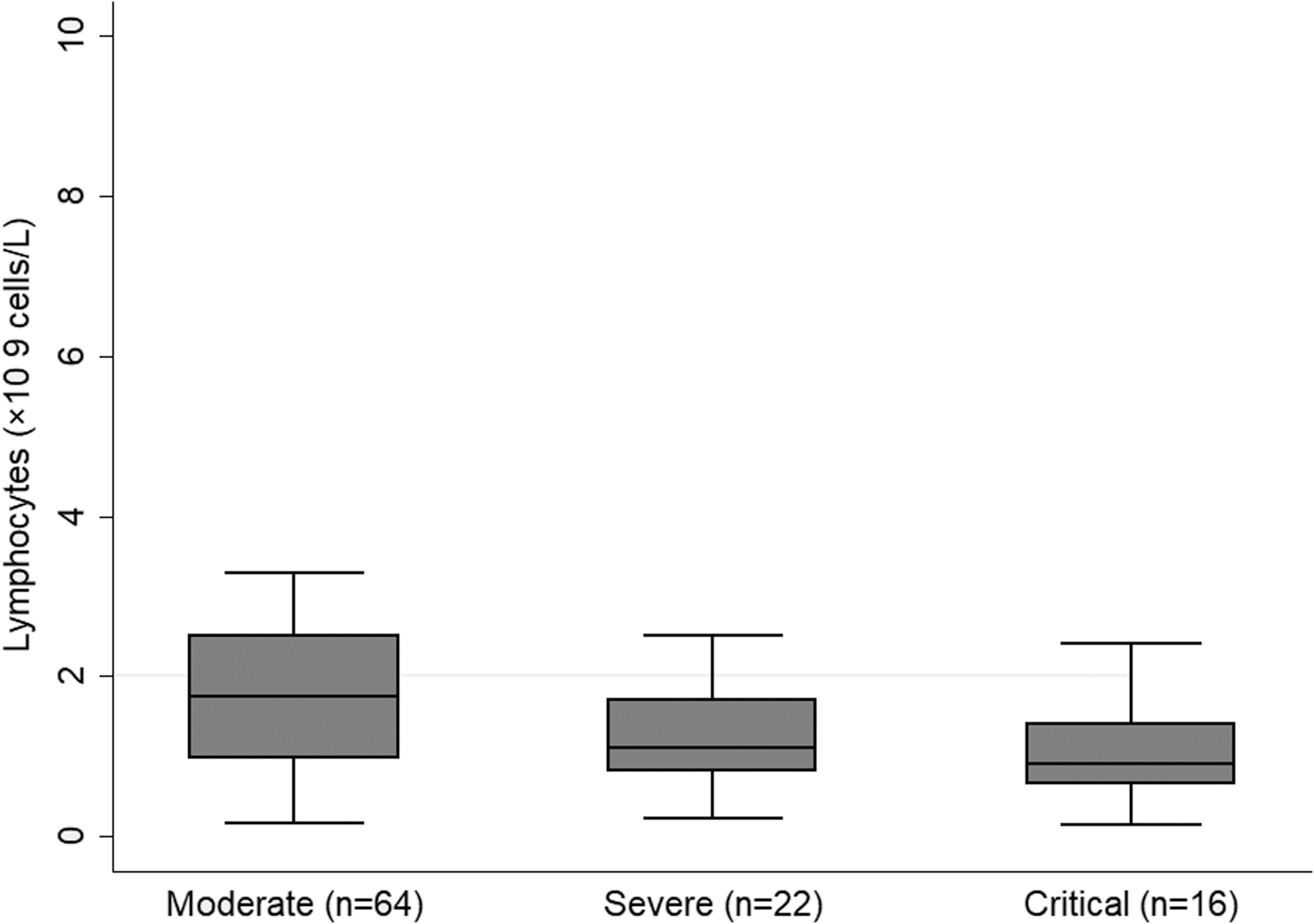
Lymphocyte count by degree of severity in Mexican patients with COVID-19. COVID-19, coronavirus disease 2019.
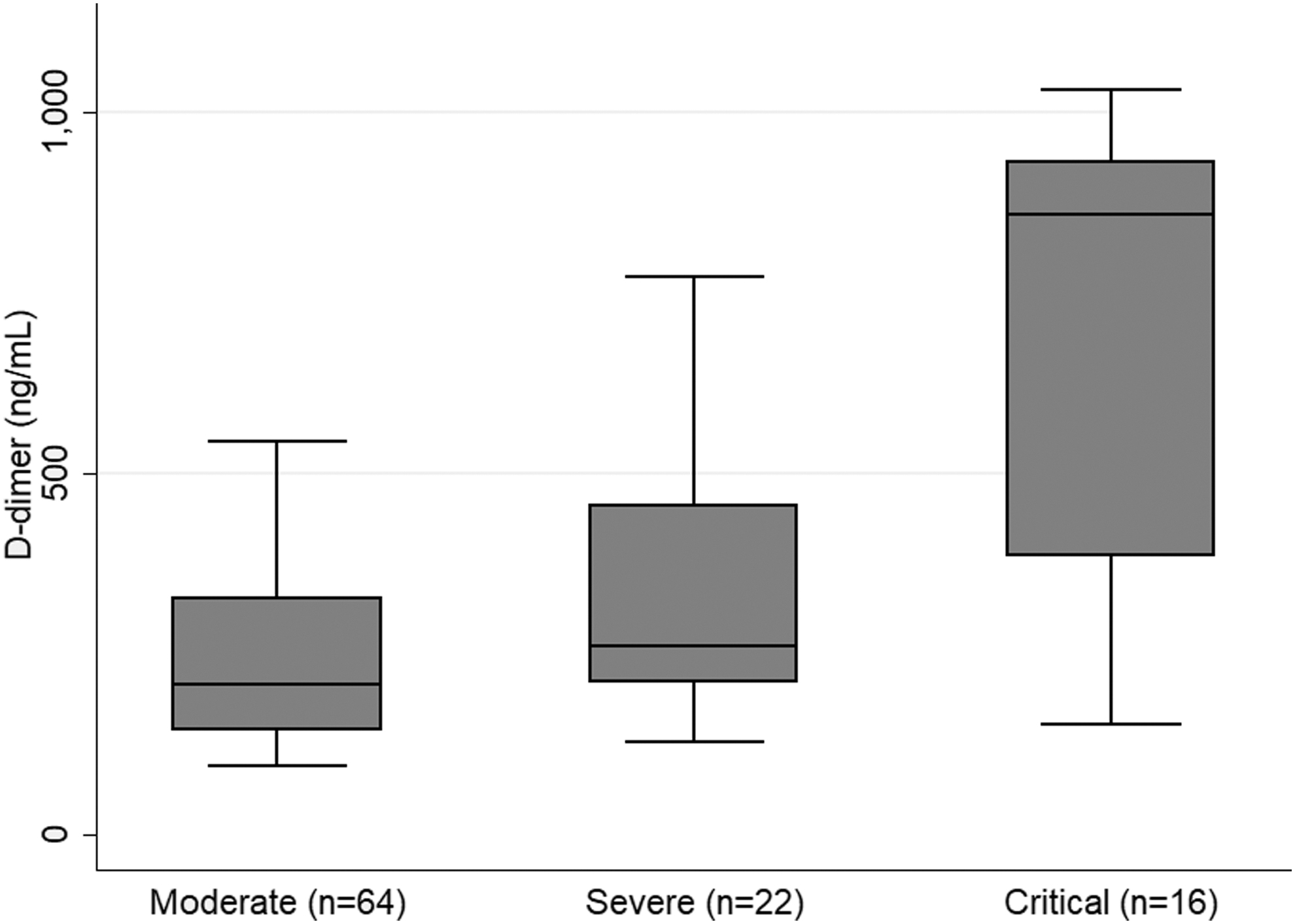
D-dimer concentrations by degree of severity in Mexican patients with COVID-19.
Laboratory Findings in Hospitalized Patients with Coronavirus Disease 2019 According to Severity
Data are presented as n, Median,
IQR (interquartile range)
Bold values indicate statistical significance, p < 0.05.
Logistic Regression Analysis of Risk Factors Associated with Coronavirus Disease 2019 Mortality
Values in bold indicate statistical significance, p < 0.05.
CI, confidence interval; OR, odds ratio.
Discussion
The findings showed that age, sex (males), elevated levels of D-dimer, and diabetes mellitus type-2 were the main risk factors associated with mortality due to COVID-19. A recent study (Zhang et al. 2020a) found that older age, high numbers of comorbidities, and more prominent laboratory abnormalities were associated with severe cases. The causes underlying the transition from mild symptoms to severe or critical conditions are not yet fully understood. It was observed that among the most frequent comorbidities, overweight was present in 78.12% of the patients, obesity in 20.71%, diabetes in 9.52%, hypertension in 5.71%, and 9.5% had other diseases. The clinical course of the disease is unpredictable due to the heterogeneity of its manifestations, ranging from asymptomatic and/or subclinical forms to critical disease with ARDS or multiorgan failure. Prognostic biomarker is not currently available to identify patients who require immediate medical attention and to estimate their associated mortality rate (Yan et al. 2020).
Some patients also report the presence of symptoms of olfactory dysfunction, such as anosmia and dysgeusia. These symptoms become more prominent in patients with COVID-19 infection.
In one meta-analysis of 15 studies involving 3739 patients, gustatory and olfactory disorder rates were estimated to be 49.1% and 61.3%, respectively (Hajikhani et al. 2020). In another meta-analysis of 24 studies with data from 8438 patients, the pooled proportions of those presenting with olfactory and gustatory dysfunction were 41.0% and 38.2%, respectively (Agyeman et al. 2020). A recent European multicenter study had 417 patients with COVID-19 with mild to moderate symptoms (mean age: 36.9 years; 63% female, n = 263) (Lechien et al. 2020). Olfactory dysfunction was reported in 11.8% of the cases before any other symptom. In our experience, anosmia was a very frequent symptom.
In this study, an association was found between underlying conditions, such as age and chronic medical conditions (diabetes and elevated D-dimer levels) and mortality from COVID-19. There are some other studies with similar results, as (Hernández-Vásquez et al. 2020), in which it is reported that various underlying chronic conditions and multimorbidity are associated with pneumonia and death in Mexican patients with COVID-19. A recent study in the Mexican population (Parra-Bracamonte et al. 2020) describes that male patients and patients older than 41 years have an increased risk of mortality due to COVID-19. Diabetes, hypertension, and obesity are the most frequent comorbidity traits associated with the highest risk of mortality in the Mexican population. Several underlying mechanisms possibly explain the relationship between obesity and COVID-19 severity. One possible hypothesis is related to the mechanical nature (restrictive pulmonary ventilatory defect), proinflammatory or immune dysregulation, or even a higher prevalence of other comorbidities such as diabetes and hypertension among obese patients (Kass et al. 2020).The association between BMI and COVID-19 severity could be of utmost importance in Mexico, where the prevalence of overweight and obesity among adults is 39.1%. However, in our study population, only 21.8% of individuals were obese.
It has been postulated that the development and severity of pneumonia may be influenced by the use of antihypertensive medication, commonly prescribed to patients with hypertension and diabetes. These medications may lead to elevated lung tissue concentrations of angiotensin-converting enzyme 2, which acts as the receptor for the entry of SARS-CoV-2 (Diaz 2020, Sun et al. 2020). However, other authors have reported that elevated angiotensin-converting enzyme 2 levels are not associated with an increased risk of pneumonia (Bravi et al. 2020). This suggests the need for further investigation about the influence of chronic conditions on the development of COVID-19.
Recent studies have also reported these pathologies in COVID-19 patients (Garg et al. 2020, Grasselli et al. 2020a, Richardson et al. 2020). Regarding sex, more men (55.2%) than women (44.7%) were found to have SARS-CoV-2 infection in this study. Previous studies (Badawi and Ryoo 2016, Channappanavar et al. 2017) have reported that Middle East respiratory syndrome coronavirus (MERS-CoV) and SARS-CoV also affected more men. A lower susceptibility of women to viral infections could be attributed to the protection of the X chromosome and sex hormones, which play an important role in innate and adaptive immunity (Jaillon et al. 2019). Our results suggest that the causative agent SARS-CoV-2 is more likely to infect older men with coexisting comorbidities, as reported in several studies worldwide. A recent study in Mexican patients documented that obesity, diabetes, and hypertension were significantly associated with severe COVID-19 on admission and the association to obesity was stronger in patients <50 years old (Denova-Gutiérrez et al. 2020). In this investigation, laboratory findings showed lymphopenia and neutropenia. Another study reported that damage to T lymphocytes may be a major factor leading to the severity of the patients' disease (Liu et al. 2017). In this group of Mexican patients, it was observed that as the degree of severity of the disease increased, nonspecific inflammatory markers, including C-reactive protein, D-dimer, and ferritin, were found to be elevated, which is consistent with previous studies (Mehta et al. 2020, Wang et al. 2020a). Older age and comorbidity have been documented to carry a higher risk of mortality (Zhou et al. 2020). A study within the Wuhan population found that older age, elevated SOFA (Sequential Organ Failure Assessment) scores, and an elevated D-dimer were risk factors for mortality from COVID-19 (Zhou et al. 2020).
In the analysis of univariate and multivariate logistic regressions, it was observed that age, being male, diabetes as comorbidity, and a D-dimer increase are strong predictors of death in hospitalized patients with COVID-19 in the area where this study was conducted. Our findings also support the observations of previous studies, which have found a greater number of hospitalized elderly patients with pre-existing conditions, diabetes being one of the most frequent (Richardson et al. 2020, Rodriguez-Morales et al. 2020). Similarly, studies have shown that elevated D-dimer levels are a prognostic factor for adverse outcomes in respiratory diseases. In addition, many patients with COVID-19 have been observed to have elevated D-dimer, findings that have been suggested to reflect the underlying thromboembolic burden and have been associated with increased mortality among these patients (Naymagon et al. 2020, Wang et al. 2020a, Zhang et al. 2020b). This study has several limitations. First, it was conducted at a single specialty hospital (High Specialty Medical Unit No. 71) located in the northern region of Mexico, which receives patients from four states. Second, only 105 hospitalized patients confirmed with SARS-CoV-2 were included. Suspected, but undiagnosed cases were ruled out in the analyses. Therefore, for future investigations, it is recommended to increase the sample size and the follow-up of this group of patients. However, the sample size was achieved in the early stages of COVID-19 spreading in Mexico, not during the peak. Finally, it is important to continue carrying out prospective research in different populations of the world to evaluate the epidemiology, pathogenesis, and clinical course of the disease associated with SARS-CoV-2 infection.
Conclusion
In this retrospective cohort study of patients with COVID-19 from a specialty hospital in the northeast region of Mexico, it was observed that clinical phenotypes and D-dimer elevation were compatible with an inflammatory state by degree of severity. It was found that the hospitalized patients with underlying chronic medical conditions such as diabetes and elevated D-dimer levels were significantly associated with increased mortality from COVID-19, with age and sex (male) as influencing factors.
Ethical Approval
Reference number (R-2020-501026).
Footnotes
Authors' Contributions
F.J.G.-A., M.A.M.-H., E.M.G., and M.A.M.C. and H.A.D.-A.: study design, data collection, data interpretation, article preparation, and literature search; F.J.G.-A. and H.A.D.-A.: data collection and literature search; and F.J.G.-A., M.d.R.G.-M., and M.A.M.C.: statistical analysis. All authors read and approved the final version of the article.
Acknowledgments
We thank all the health personnel of the High Specialty Medical Unit # 71 of the Mexican Institute of Social Security (UMAE) No. 71, and IMSS and CONACYT for the research stay in Mexico in response to the COVID-19 contingency.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.