
Abstract
Aim:
Echinococcosis, caused by Echinococcus species, is an important zoonotic disease causing major health problems in humans and animals. Herein, we aimed to evaluate the epidemiology, clinical and laboratory parameters, radiological, serological, pathological, and treatment protocols of followed-up cases of hydatidosis.
Methods:
A total of 550 patients diagnosed with hydatid cyst disease were included in this study. Patients who were positive for one or more of the enzyme-linked immunosorbent assay or indirect hemagglutination test, pathological results, or radiological findings were examined. The data analyzed were collected from nine centers between 2008 and 2020. Records were examined retrospectively.
Results:
Among the patients, 292 (53.1%) were women and 258 (46.9%) were men. The patients' mean age was 44.4 ± 17.4 years. A history of living in rural areas was recorded in 57.4% of the patients. A total of 435 (79.1%) patients were symptomatic. The most common symptoms were abdominal pain in 277 (50.4%), listlessness in 244 (44.4%), and cough in 140 (25.5%) patients. Hepatomegaly was found in 147 (26.7%), and decreased breath sounds were observed in 124 (22.5%) patients. Radiological examination was performed in all cases and serological methods were also applied to 428 (77.8%) patients. The most frequently applied serological test was IHA (37.8%). A single cyst has been found in 66% patients. Hepatic involvement occurred in 327 (59.4%), pulmonary involvement was found in 128 (23.3%), whereas both of them were recorded in 43 (7.8%) patients. Splenic involvement was only detected in nine (1.6%) patients. Echinococcus granulosus (72.5%) was most frequently detected. Cyst diameters of 56.9% of the patients were in the range of 5–10 cm. A total of 414 (75.2%) patients received albendazole as an antiparasitic. Mortality was noted in nine (1.6%) patients.
Conclusion:
Echinococcosis is an important public health problem in Turkey. It can affect the social, economic, and political structures of the community. Public education and awareness are extremely important.
Introduction
Echinococcosis is a parasitic zoonotic disease caused by Echinococcus species, including Echinococcus granulosus, Echinococcus multilocularis, Echinococcus vogeli, and Echinococcus oligarthus. E. granulosus cysts are unilocular, whereas E. multilocularis causes alveolar type disease (Eckert and Deplazes 2004). The life cycle involves a definitive host (dogs, wolves, jackals, and foxes) and an intermediate host. Humans are incidental hosts, and are not part of the cycle (Conraths and Deplazes 2015, Cerda et al. 2018). Cystic echinococcosis is frequently encountered in Mediterranean countries. It is considered as an important public health problem in Turkey and worldwide (Jenkins et al. 2005, Parlak and Tekin 2021).
The initial phase of the primary infection is asymptomatic. Infections are generally acquired in childhood, whereas symptoms appear in adulthood. Calcified and/or small cysts might remain asymptomatic for many years. Complications, such as compression effects, obstruction of blood and lymphatic flow, secondary bacterial infections, and rupture may occur in others (Frider et al. 1999). Transmission does not occur from human to human. The liver and lung are most frequently affected, although organs, such as kidney, spleen, brain, eye, bone, ovary, testis, pancreas, peritoneum, and the pleural cavity are rarely involved (Sari et al. 2009, Agudelo Higuita et al. 2016).
Imaging is crucial in the diagnosis of echinococcosis (Agudelo Higuita et al. 2016). It is recommended to combine imaging with serological tests to enhance the diagnostic value. Computed tomography and magnetic resonance imaging (MRI) are more valuable in the diagnosis of lesions occurring in other parts of the body, such as brain (McManus et al. 2003, Agudelo Higuita et al. 2016).
Zoonoses must be tackled in a decisive manner within the “one health” framework. The purpose of this multicenter study was to provide detailed information regarding the epidemiology of the disease, its diagnosis, clinical, laboratory and radiological findings, along with treatment in Turkey.
Materials and Methods
Study design and patient
A total of 550 patients with different clinical manifestations recruited between 2008 and 2020 were included in this study. We performed a retrospective, multicenter trial at nine centers. Ethical committee approval was granted by the Fatih Sultan Mehmet Education and Research Hospital in Istanbul, Turkey (Clearance No. 2020/89).
Serological methods (enzyme-linked immunosorbent assay [ELISA], the indirect hemagglutination test [IHA], immunofluorescence antibody test [IFAT], and other serological techniques—radioimmunoassay, immunoelectrophoresis, the indirect fluorescent antibody [IFA] test, and the direct fluorescent antibody [DFA] test) were used.
Patients older than 18 years with suspicion based on clinical characteristics, and patients diagnosed based on radiological examinations (ultrasonography and MRI) and/or with serological method positivity or with protoscoleces or parasites identified in specimens (obtained by surgery or puncture) were included.
Statistical analyses
The data were recorded and analyzed by SPSS 20.0 for Windows software (SPSS, Inc.). Data were expressed as number and percentage for categorical variables, and as mean ± standard deviation for numerical variables. Chi-squared tests were used for data analysis. Compatibility with normal distribution was assessed using the Kolmogorov–Smirnov test. The Kruskal–Wallis test was applied to non-normally distributed numerical variables. The Mann–Whitney U-test was used for two-way group comparisons. A value of p < 0.05 was considered significant for all tests.
Results
A total of 292 (53.1%) of the 550 patients recruited in this study were women (p = 0.159). The patients' mean age was 44.4 ± 17.4 years; 148 (26.9%) were aged 18–29 years, versus 93 (16.9) aged 30–39 years, 98 (17.8%) aged 40–49 years, 106 (19.3%) aged 50–59 years, and 105 (19.1%) aged 60 years or older. More participants were living in rural areas (n = 321, 57.4%) than urban centers (n = 229, 41.6%; p < 0.001). The most urban areas were Izmir (29.1%), Erzurum (19.8%), Ağrı (8.9%), and Antalya (5.5%).
In terms of occupation, 145 (26.4%) participants were farmers, 83 (15.1%) working in animal husbandry, 80 (14.5%) were housewives, 2 (0.4%) were forestry workers, 2 (0.4%) hunters, and the rest (13.1%) were from different occupational groups. The remaining patients were without record.
Four hundred thirty-five patients (79.1%) exhibited symptoms. Symptoms and physical examination findings are given in Table 1. The most common symptoms were abdominal pain, listlessness, lack of appetite, cough, fever, and chest pain. A physical finding was present in 450 (81.8%) patients; hepatomegaly, diminished breath sounds, fever, and hemoptysis are the most common signs. A total of 115 (20.9%) patients were asymptomatic at time of monitoring, and physical examination was normal in 18.2% of patients. Urticaria was also found in 6.9% of patients. Eosinophilia was detected in 54 (9.8%) and high C-reactive protein levels in 2.9% patients.
Symptom and Finding Distributions in the 550 Patients
E. granulosus was detected in 399 (72.5%) and E. multilocularis was identified in 6 (1.1%) patients using imaging techniques, serologic tests used to confirm the diagnosis. A total of 125 patients (22.7%) had contact with animals as reported in their records. Contact with dogs (23.2%), dogs, cats, and cattle (35.2%), and dogs, cattle, and sheep (22.4%) was the most common animal species.
Bilateral hepatic lobe involvement occurred in 174 (31.6%) patients, whereas right lobe and left lobe involvement were recorded in 119 (21.6%) and 34 (6.2%) patients, respectively. Pulmonary left lobe, right lobe, and bilateral lobe involvement were noticed in 58 (10.5%), 57 (10.4%), and 13 (6.2%) patients, respectively. The presence of hydatid cyst both in liver and lungs was determined in 43 (7.8%) patients. Cyst sites are given in Table 2. A 15 cm diameter cystic lesion in the liver is given in Fig. 1. Serological examinations used in diagnosis are given in Table 3.

A 15 cm diameter cystic lesion in the liver.
Cyst Sites Shown in the Table
Serological Tests
ELISA, enzyme-linked immunosorbent assay; IFAT, immunofluorescence antibody test; IHA, indirect hemagglutination test.
Ultrasound lesion classifications were available for 387 patients. Ninety-two (23.8%) were type CE1, 74 (19.1%) were CE2, 67 (17.3%) were CE3a, 56 (14.5%) were CE3b, 54 (14%) were CE5, and 44 (11.4%) patients were CE4. Classification has not been noted for 163 (29.6%) patients despite undergoing imaging. A comparison of organ involvements is given in Table 4.
A Comparison or Organ Involvements and Various Parameter Values
A single cyst lesion was present in 363 (66%) of the 550 patients and more than one lesion has been recorded in 44%. Three or fewer lesions were detected in 94% patients. Lesions were <5 cm in diameter in 101 (18.4%) patients, 5–10 cm in 319 (58%), and >10 cm in 130 (23.6%) patients. Duration of symptoms was <45 days in 81.1% patients. Numerous cystic lesions were observed inside muscle tissue (Fig. 2).
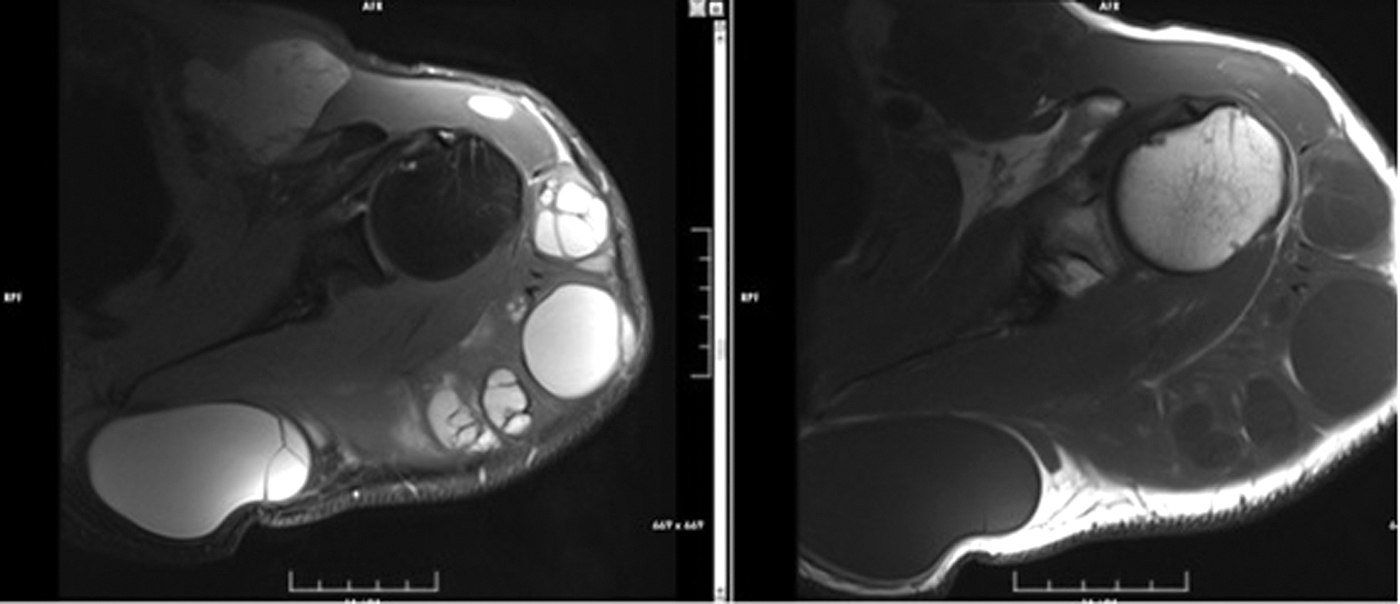
Numerous cystic lesions inside muscle.
Macroscopic appearance was compatible with echinococcosis in 49.3% patients. Pathological examination was performed on specimens taken from 390 (70.9%) patients.
Records were available for 390 (70.9%) patients from whom specimens was subjected to pathological examination. A lamellar membrane was revealed in pathological examination of 86 (15.6%), cuticular membrane in 63 (11.5%), cyst membrane in 32 (5.8%), pseudocapsule in 30 (5.5%), lamellar membrane and pseudocapsule in 26 (4.7%), germinal membrane in 26 (4.7%), scolex in 19 (3.5%), scolex and lamellar membrane in 16 (2.9%), and necrosis in 11 (2%) patients.
Treatment
A total of 414 (75.2%) patients received albendazole as an antiparasitic before or after surgery. Antiparasitic remedy was initiated within 60 days before surgery in 94.8% patients. Medication was maintained for 104.1 ± 90.1 days after surgery. Total duration of treatment was 93.7 ± 96.2 days. Medical treatment in 256 (46.5%) patients was interrupted for 15 days following administration for 28 days. One hundred sixty (29.1%) patients were observed for some period of time without treatment. Complications among 107 (22.7%) follow-up patients were recorded. The most common complications were cyst rupture in 24 (11.7%), followed by secondary infection in 23 (19.2%), biliary fistula in 12 (10%), cyst rupture and secondary infection in 11 (9.2%), and liver damage in 5 (4.2%) patients.
Surgical procedures
“Puncture, aspiration, injection, respiration” (PAIR) was performed in 102 cases. Twenty-five (4.5%) patients underwent modified catheterization. Open surgery was performed in 227 (82.5%) of the 270 patients with hepatic hydatid cyst. Thoracotomy, cystectomy, and capitonnage were carried out in 144 (88.3%) of the 163 patients with pulmonary hydatid cyst. Thoracotomy was implemented in nine (5.5%), cystectomy in five (3.1%), and cystectomy-capitonnage in three (1.8%) patients.
Twenty percent NaCl was used as a scolicidal agent in 242 (44%) cases, povidone–iodine in 90 (16.4%), 30% NaCl–95% ethanol in 14 (2.5%), 95% ethanol in 12 (2.2%), 30% NaCl-95% ethanol–baticon in 6 (1.1%), and H2O2 in 6 (1.1%) patients.
Mean length of hospital stay was 10.3 ± 9.8 days. Mean duration of follow-up was 16.6 ± 21.9 months. A total of 438 (79.6%) patients resolved with treatment; 103 (18.7%) patients were lost to follow-up for various reasons. Recurrence was observed in 70 (12.7%) patients and it was 83.9% for the same location. Mean time elapsing to recurrence was 436.4 ± 595.8 days. Abdominal pain (35.6%), pulmonary abnormalities (4.4%), and abdominal pain and auscultation abnormalities (4.4%) were present at the time of recurrence. Mortality occurred in nine (1.6%) patients during follow-up.
Discussion
Echinococcosis is among the most neglected tropical parasitic diseases targeted for elimination by the World Health Organization (WHO 2012, Tamarozzi et al. 2018). It is frequently spreading in areas where extensive system of animal husbandry is widespread (Eckert and Deplazes 2004, Sari et al. 2009). Alveolar, cystic, or polycystic echinococcosis occur, depending on the species of parasite in intermediate hosts and humans (Cerda et al. 2018).
The epidemiology is affected by socioeconomic levels, climatic conditions, nutritional status, and livestock production. The proximity between humans and dogs is very important in this high prevalence (Yazar et al. 2006). The disease is endemic in Turkey (Sari et al. 2009). High prevalences have been documented in endemic rural areas of some countries (Moro and Schantz 2006). In the present study, 57.4% of the patients are living in rural areas.
Women represent the majority of adult cases (Botezatu et al. 2018, Tamarozzi et al. 2018, Aydin and Adigüzel 2019). In this context, Aydın and Adigüzel (2019) found that 65.6% of their 482 patients were women, whereas Mor et al. (2018) have reported a figure of 79.1%. However, a predominance of male cases has also been documented in some studies (Shams-Ul-Bari et al. 2011, Tartar et al. 2020). In this study, women constitute 53.1% of the cases, although this was not statistically significant. This could be attributed to the fact that the majority of those engaged in agriculture, animal husbandry, and food preparation are women.
The most important risk factors are intensive livestock farming, poor socioeconomic status, and inadequate education (Aydin and Adigüzel 2019). The disease is more commonly seen in hunters, farmers, shepherds, slaughterhouse employees, veterinarians, and pet owners (Mandell et al. 2014). In this study, the reported occupations were farming (26.4%), animal breading (15.1%), and housewifery (14.5%). The most common mode of transmission includes contact with dogs and contaminated water and foods (Torgerson et al. 2020). In this study, contact with dogs among our patients, either singly or together with other animals, was addressed at a rate of 86.4%. This was in line with previous literature.
Studies have reported that the incidence increases with age (Cohen et al. 1998, Mirshemirani et al. 2011, Wang et al. 2020). The increased incidence with age is associated with gradual emergence of the disease (Aydin and Adigüzel 2019). Alveolar echinococcosis produces late clinical symptoms, owing to its long incubation period. Monitoring women and over 30-year-old age group are very crucial in terms of preventing alveolar echinococcosis (Wang et al. 2020). In this study, 43.8% of the patients were aged 18–40 years, and 37.1% were aged 40–60 years. Herein, a high frequency of cyst was observed in middle age. We attribute this to early diagnosis and use of imaging methods.
As elsewhere in the world, hepatic and pulmonary echinococcosis are most commonly seen in Turkey (Botezatu et al. 2018, Mor et al. 2018, Tartar et al. 2020). A single lesion in a single organ occurs in the majority of the cases (40–80%). The liver is the most frequently affected organ (70%), and the right lobe is affected more often than the left lobe. The lung is the second most frequently affected (20%) organ (Agudelo Higuita et al. 2016, Wen et al. 2019). Other organs (such as, heart, kidney, spleen, brain, bone, muscle) may be involved at rates of 10–20% (Mandell et al. 2014). In this study, liver was affected in 59.4% and then lung in 23.3% of the patients. Single organ involvement was consistent with previous literature. The presence of hydatid cyst both in liver and lung was detected in 7.8% patients. Multiple organ involvement was determined in 10.5% patients, and splenic involvement in nine. Hepatic involvement should be investigated in cases of nonhepatic echinococcosis.
Patients symptoms and findings vary depending on the site and size of the cyst. Cases in which the cyst is small, peripherally located, and unruptured are asymptomatic (Frider et al. 1999, Rinaldi et al. 2014). Hepatic and pulmonary involvements produce no symptoms for many years. Large cysts give rise to compression symptoms (Sarı et al. 2009). Pain in the right hypochondrium, nausea, vomiting, and jaundice may be observed. Findings may be observed earlier in cysts involving organs, such as the eye and brain. A tumor-like mass, abdominal distension, and hepatomegaly may be palpable (Chaabouni et al. 1999, Wen et al. 2019). Pulmonary echinococcosis tends to exhibit slow growth, and can give rise to respiratory difficulty, cough, phlegm, hemoptysis, and chest pain. Cyst rupture in an organ can cause fever, urticaria, eosinophilia, and anaphylactic shock (Santivanez and Garcia 2010, Wen et al. 2019). In this occasion, Tartar et al. (2020) reported abdominal pain, abdominal mass, chest pain, and fever in his study. Active infection findings emerged in approximately one in three cases in the HERACLES study (Tamarozzi et al. 2018). Abdominal pain (50.4%), listlessness (44.4%), cough (25.5%), chest pain (22%), and fever (12.9%) were reported during examination of our cases. During physical examination, we found hepatomegaly (26.7%), decreased respiratory sounds (22.5%), fever (12.9%), and hemoptysis (7.5%) in our patients. Urticaria was detected in 6.9% patients.
Laboratory tests are not diagnostic in hydatid cyst disease. Anomalies in liver tests, leukopenia, thrombocytopenia, and mild eosinophilia can be seen. Eosinophilia is present in 25% cases. The probability increases in the presence of antigen leakage (Keong et al. 2018). Rates >39% have been reported in the literature (Botezatu et al. 2018). In this study, eosinophilia was detected in 54 patients (9.8%). This figure is lower than that reported in the literature. This could be ascribed to absence of rupture and cyst leakage in our patients. Eosinophilia is not specific for diagnosis.
One of the ELISA-based serological tests is used. Sensitivity is 85–98% in hepatic involvements, but lower in pulmonary involvement (50–60%). Sensitivity is higher (90–100%) in multiple organ involvements (Barnes et al. 2012). IHA test positivity is significant; however, negative results do not exclude the disease. IHA (37.8%), ELISA+IHA (15.5%), and ELISA+IFAT (10%) were used in this study. These tests are not suitable for follow-up as they remain positive for extended periods. Serology values do not affect the treatment decision.
Botezatu et al. (2018) reported a cyst diameter of 5 cm or more in 82% cases. Studies have described medical treatment is sufficient in cysts smaller than 4 cm with a thin wall and in the young (Shams-Ul-Bari et al. 2011, Mandell et al. 2014, Keong et al. 2018). Single cysts were determined at a rate of 66% in this study. Four or more cysts were found in 6% cases. Consistent with the previous literature, the highest proportion of patients (58%) was in 5–10 cm diameter group.
The benzimidazole compounds (albendazole and mebendazole) are effective for treatment. The first choice in treatment is albendazole (Mandell et al. 2014, Botezatu et al. 2018). This causes the disappearance of 48% cysts, and shrinkage in 24%. Mebendazole to a lesser extent are used in treatment. Because toxicological examinations cannot be performed, usage is recommended for 4 weeks, followed by a 2-week discontinuation. However, recent publications have shown that is of equivalent, or even more effective, with no increasing the risk of side-effects. Cyst numbers decreased markedly with increasing the duration of usage. Ninety-four percent of cysts were found dead after 3 months (McManus et al. 2003, Velasco-Tirado et al. 2018). Albendazole was given to 75.2% of our patients. The mean length of treatment was 93.7 days. The drug was initiated 1 month before surgery in 83.7% cases. Drug therapy was maintained on average, 104.1 days, postoperatively. Twenty-eight day courses were given to 46.5% patients, with a 14-day interval between courses.
The reported recurrence rate in the literature is 2–25% (Shams-Ul-Bari et al. 2011, Mor et al. 2018). The recurrence rate in this study was comparable with previous studies at 12.7%. Abdominal pain and pulmonary findings were most frequently present at the time of recurrence.
Asymptomatic cases are commonly seen in endemic cases (Frider et al. 1999). Up to 60% of cystic echinococcosis cases were reported to be asymptomatic (McManus et al. 2003). Seventy-five percent of asymptomatic cases remained symptom free over 10- to 12-year follow-up, irrespective of size. No cyst growth occurred in 57.1 of the nonoperated cases (Frider et al. 1999).
Surgery represents the basis of treatment (Mandell et al. 2014). Surgery is employed for active, symptomatic, and complicated cysts, and for cysts >5 cm in size. Medical treatment or PAIR can be used (Keong et al. 2018). Laparoscopic intervention is feasible in cysts <6 cm located superficially. The objective of surgery is to remove the cyst and effectively obliterate the remaining space. The open surgery most commonly performed on the liver (88%) is partial pericystectomy (Botezatu et al. 2018). Open surgery was performed on 227 (93%) of 244 patients with hepatic involvement in this study. A total of 102 patients received medical treatment plus PAIR. Thoracotomy, cystectomy, and capitonnage were performed on 88.3% of the 163 patients with pulmonary involvement.
Scolicidal agents can be used intraoperative or during PAIR. Betadine (povidone–iodine), 20% hypertonic saline, 20% Savlon (1.5/0.15% cetrimide–chlorhexidine), and 95% ethyl alcohol have been described as effective scolicidal agents (Keong et al. 2018). The most frequently used scolicidal agents in this study were 20% NaCl (64.7%), povidone–iodine (24.1%), and 30% NaCl-95% ethanol (5.3%).
Echinococcosis rupture into the biliary tract, opening into the peritoneal cavity, acute abdomen, rupture into cutaneous tissue, and vascular complications are the frequent common complications of hepatic hydatid cysts (Dziri et al. 2009). Cystobiliary fistula has been reported at a rate of 5–42%. A cyst diameter >10% is the only independent predictor of this complication (El Nakeeb et al. 2017). Complications, such as intrapulmonary rupture, pleural rupture, pleural thickening, ruptured cyst infection, biliobronchial fistula, pneumothorax, pleural effusion, and empyema have been highlighted in pulmonary cysts. Cysts can lead to pulmonary abscess caused by secondary infection (Dziri et al. 2009, Turgut et al. 2009). Complications have been developed in 120 (21.8%) patients in this study. Cyst rupture was determined in 24 (20%), secondary infection in 23 (19.2%), biliary fistula in 12 (10%), cyst rupture and secondary infection in 11 (9.2%), and liver damage in 5 (4.2%) patients.
Conclusions
The principal limitation of this study is its retrospective design. Echinococcosis is endemic in Turkey. Awareness of echinococcosis from physicians, radiologists, and laboratory staff point of view is very important in terms of public health. Echinococcosis should be remembered in mass lesions in endemic regions. Hepatic involvement is most frequently seen. Hepatic involvement must also be investigated when involvement of another organ was detected. Albendazole is most frequently used in treatment. Multidisciplinary activity is essential for diagnosis, imaging, and treatment. Early diagnosis, radical surgery, and antiparasitic treatment are highly recommended. There is no vaccine for the disease. Prevention or control of the disease in humans depends on its control or elimination in dogs. Regular screening must be performed to prevent the disease. Public education and information are also essential. Better quality epidemiological research and surveillance programs are required.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this study.