
Abstract
Background:
A history of Lyme disease can complicate the interpretation of Lyme disease serology in acutely symptomatic patients.
Materials and Methods:
We prospectively enrolled children undergoing evaluation for Lyme disease in the emergency department of one of eight participating Pedi Lyme Net centers. We selected symptomatic children with a Lyme disease history (definite, probable, or none) as well as an available research biosample. We defined a Lyme disease case with either an erythema migrans (EM) lesion or positive two-tier serology with compatible symptoms. Using a generalized estimating equation, we examined the relationship between time from previous Lyme disease diagnosis and current Lyme disease after adjustment for patient demographics and symptoms as well as clustering by center.
Results:
Of 2501 prospectively enrolled study patients, 126 (5.0%) reported a history of definite or probable Lyme disease. Of these children with previous Lyme disease, 47 met diagnostic criteria for Lyme disease at the time of enrollment (37.3%; 95% confidence interval [CI] 29.1–45.7%); 2 had an EM lesion, and 45 had positive two-tier Lyme disease serology. Over time from the previous Lyme disease diagnosis, the less likely the patient met diagnostic criteria for Lyme disease (adjusted odds ratio 0.62 per time period; 95% CI 0.46–0.84).
Conclusions:
For children with a history of Lyme disease before enrollment, one-third met the diagnostic criteria for acute Lyme disease with a declining rate over time from previous Lyme disease diagnosis. Novel Lyme disease diagnostics are needed to help distinguish acute from previous Lyme disease.
Introduction
Lyme disease serologic tests may remain positive indefinitely after successfully treated Lyme disease (Kalish et al. 2001, Glatz et al. 2006, Kannian et al. 2007). Protective immunity, however, is neither complete nor lifelong, and reinfection with Borrelia species after early Lyme disease is well described (Nadelman and Wormser 2007, Branda et al. 2018). When evaluating a patient for a suspected reinfection, the challenge for clinicians can be to determine whether a patient's antibody reactivity represents active versus previous infection.
We assembled an eight-center cohort of children undergoing emergency department evaluation for acute manifestations of Lyme disease. Our goals were to examine the proportion of children with a history of Lyme disease who had positive Lyme disease serology and to determine the relationship between seropositivity and the time from previous infection. We hypothesized that most children with a history of Lyme disease would have a positive two-tier Lyme disease serology and the proportion would decline with time from previous infection.
Materials and Methods
Study design
We performed a planned substudy of an ongoing prospective cohort study conducted by Pedi Lyme Net. We enrolled children undergoing evaluation for acute Lyme disease in one of eight participating emergency departments between June 2015 and October 2020 (Nigrovic et al. 2020). Enrollment ceased at all participating sites between March and July 2020 due to the coronavirus disease 2019 (COVID-19) pandemic (exact dates varied between centers). The study protocol was approved by the institutional review board at each participating institution with permission for data sharing.
Study patients
Study staff approached emergency department patients ≤21 years of age whose treating clinicians had decided to obtain Lyme disease serology to evaluate for acute Lyme disease. For this substudy, we limited our study population to children who provided a Lyme disease history and had a research serum sample collected.
Clinical factors
We obtained clinical history from medical providers as well as subjects and families, including the specific type and duration of current symptoms as well as Lyme disease history. Treating clinicians reviewed the clinical history with parents and patients as well as available medical and laboratory records to determine Lyme disease history classified in the following categories: definite (probable or confirmed Lyme disease), possible (possible Lyme but unable to confirm), or no (no history of Lyme disease). For those with a history of Lyme disease, we asked how long ago the diagnosis had been made: 1–3, 4–12, 13–24, or >24 months. Diagnoses made within the previous month were considered part of the current illness. All data were collected prospectively using standardized data collection instruments (RedCap™ hosted by Harvard University) (Harris et al. 2009).
Research testing
As specific Lyme disease two-tier tests varied by participating clinical center (Maulden et al. 2020), we performed a research on first-tier enzyme immunoassay (EIA) for all enrolled patients using a biobanked serum sample: a C6 EIA between June 2015 and December 2019 (Oxford Immunetics, Marlborough, MA) when the manufacturer stopped selling this assay followed by a VlSe EIA (DiaSorin, Stillwater, MN) at a single research laboratory (Branda Laboratory, Massachusetts General Hospital, Boston, MA). Children with a positive or equivocal first-tier test had a supplemental IgG and IgM immunoblot performed at one of three commercial laboratories (ARUP Laboratories, Salt Lake City, UT [n = 1 center], Mayo Clinical Mayo Medical Laboratories, Rochester, MN [n = 2 centers], or Quest Diagnostics, Secaucus, NJ [n = 5 centers]) and interpreted using standardized criteria (Centers for Disease Control and Prevention 1995, Lipsett et al. 2016). A positive IgM immunoblot alone was only considered positive in patients with <30 days symptom duration (Lantos et al. 2016).
Lyme disease diagnosis
We defined a case of acute Lyme disease as either the presence of a physician-diagnosed erythema migrans (EM) lesion(s) or a positive two-tier Lyme disease serology in a child with clinical findings compatible with Lyme disease (e.g., facial palsy, meningitis, carditis, or arthritis) (Nigrovic et al. 2017). We defined a positive two-tier serology as a positive or equivocal first-tier EIA followed by a positive supplemental immunoblot (positive IgG required if symptom duration >30 days) (Sivak et al. 1996, Lantos et al. 2016).
Statistical methods
We compared proportions using a chi square test and medians using Mann Whitney test and present proportions with 95% confidence intervals (CIs). We used a generalized estimating equation to evaluate the relationship between time since previous Lyme disease diagnosis and likelihood of acute Lyme disease adjusted for age, gender, race, and ethnicity as well as clinical stage clustered by center.
We used IBM SPSS statistics (27.0.0) for all analyses.
Results
Of the 6757 eligible children over the study period, study staff approached 3862 children of which 2745 (71.1% of approached) consented to study participation (Fig. 1). Of those enrolled, 2501 (91.1%) had both a research Lyme disease test and history recorded. Of these, 126 children (5.0%) had previously been diagnosed with Lyme disease (92 definite and 34 probable previous Lyme disease). The previous Lyme disease diagnosis had been made 1–3 months ago (n = 11), 4–12 months (n = 6), 13–24 months (n = 22), or >24 months (n = 67). Children with a history of Lyme disease had symptoms similar to those without Lyme disease history (early disease 1.7% previous vs. 2.3% no history, early disseminated 56.2% vs. 47.0%, late 42.1% vs. 50.7%, p = 0.14).
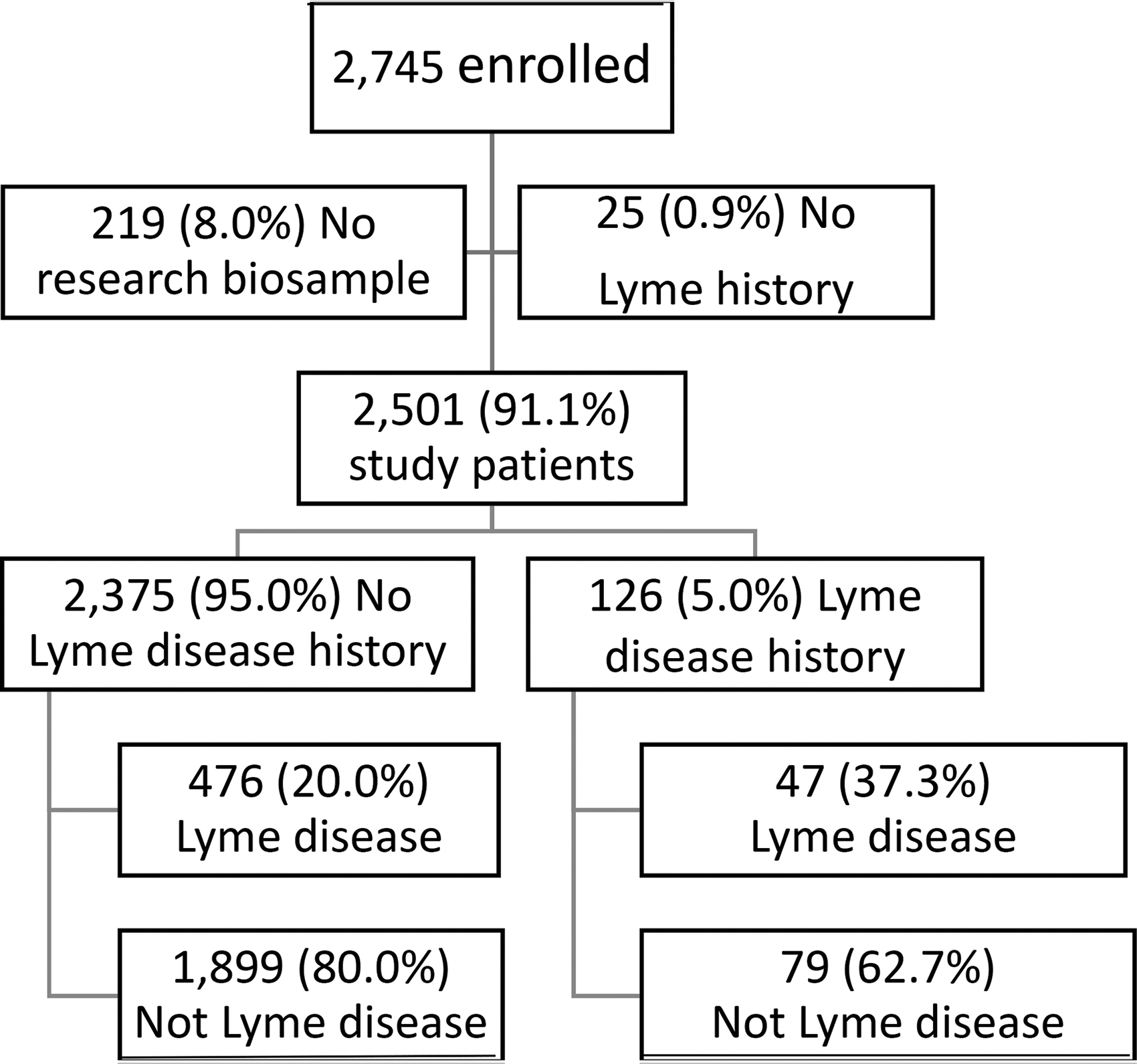
Patient enrollment.
Of the 126 children with a history of Lyme disease, the median patient age was 11 years (interquartile range 7–14 years), and 74 (58.7%) were male. Of these, 47 children (37.3%; 95% CI 29.1–45.7%) met the diagnostic criteria for Lyme disease at the time of enrollment. Of these, 2 (4.3%) had a single EM lesion and 45 had positive 2-tier Lyme disease serology (20 positive IgG alone, 8 positive IgM alone, and 17 both positive immunoblots), of whom 18 had early disseminated and 27 Lyme arthritis. A higher proportion of children with a Lyme disease history had Lyme disease than those without [47/126 (37.3%) vs. 476/2375 (20.0%); p < 0.001)]. The longer the time interval from the previous Lyme disease diagnosis, the less likely the patient had met diagnostic criteria for current Lyme disease (adjusted odds ratio 0.62 per time period; 95% CI 0.46–0.84).
Of the 79 children with a history of Lyme disease who did not meet the diagnostic criteria for acute Lyme disease, 4 had a positive and 1 an equivocal first-tier C6 EIA test. Of these, all five children had a negative supplemental immunoblot (Table 1).
Five Children with History of Lyme Disease with a Positive or Equivocal C6 Enzyme Immunoassay Index Value and a Negative Supplemental Immunoblots
Discussion
In our cohort of children undergoing emergency department evaluation for Lyme disease, approximately one-third of enrolled children with a history of Lyme disease met diagnostic criteria for current Lyme disease. The odds of testing positive for Lyme disease declined with time from prior diagnosis, likely reflecting recall bias, diagnostic confusion, and time-dependent seroreversion. In our cohort of children presenting to the emergency department for the evaluation of acute Lyme disease, the challenge for the treating clinician is to distinguish new from resolved infection (Nadelman and Wormser 2007).
Serologic testing for Lyme disease is indicated when clinicians suspect disseminated Lyme disease. Because serologic tests measure a host immune response rather than the presence of an infecting organism, the clinician must use clinical context to determine whether a positive test represents active or past infection. In the case of Lyme disease, prior infection does not guarantee protective immunity from a subsequent infection (Aguero-Rosenfeld et al. 1993). Thus, a challenge for clinicians is to determine whether positive serologic testing results after previous Lyme disease represent new infection or an immune response from prior exposure (Branda et al. 2013). In children with a history of Lyme disease, novel methods to directly detect the Borrelia pathogen will provide the most accurate way to distinguish between active and previous infection (Schutzer et al. 2019).
Our findings highlight an important obstacle clinicians may face when evaluating children for Lyme disease. Interestingly, two-thirds of children with a history of Lyme disease did not have positive two-tier serology. Some individuals who are treated for Lyme disease early in their infection may never become seropositive, whereas other treated individuals may have eventual (but unpredictable) decline and disappearance of the specific antibodies detected by these tests (Kalish et al. 2001, Kannian et al. 2007). In addition, many individuals who report prior Lyme disease lack definitive testing to support this history. In several treatment trials for symptoms persisting after Lyme disease, few screened subjects had adequate documentation of prior Lyme disease that the studies had difficulty meeting enrollment targets (Klempner et al. 2001, Krupp et al. 2003, Fallon et al. 2008). Thus, a stated history of Lyme disease should be critically examined, especially when previous medical records are not available for review. Despite these limitations, patient history is frequently the most accurate information available to treating clinicians when evaluating a patient for Lyme disease.
Diagnosing Lyme disease in a patient with prior seropositivity presents a diagnostic challenge. Serology should be interpreted in the context of a patient's prior probability of a diagnosis. In the case of Lyme disease, an intermediate prior probability can be “promoted” to a more confident diagnosis with a positive two-tier serologic test result (Tugwell et al. 1997). If one does not take past infection into account when evaluating a patient for Lyme disease, one may erroneously diagnose current Lyme disease based on an uninformative laboratory result. By contrast, if one discounts a positive serologic test as past infection, the diagnosis of active Lyme disease may be missed. This places a greater diagnostic burden on other sources of information, such as clinical evaluation to avoid both Lyme disease overdiagnosis and delays in making alternative diagnoses.
Our study has several important limitations. First, we obtained the history of Lyme disease from the patients and/or their caregivers and we were unable to confirm the previous diagnosis with either medical record or laboratory review. Although recall bias may have resulted in either under- or over-reporting of prior diagnoses, we utilized the best available clinical information available to the treating team evaluating a symptomatic child. In addition, we were unable to determine the adequacy of antibiotic treatment for the previous Lyme disease. Second, given the challenge for most parents to recall exactly when an event occurred, we collected the time from previous Lyme disease diagnosis in categories that limited our ability to quantify the time-based association between Lyme disease history and current criteria for Lyme disease. Last, as we did not follow children prospectively from the time of initial Lyme disease diagnosis, we cannot determine risk of reinfection.
Conclusions
Two-tier Lyme disease serology suffers from several well-recognized limitations, including the challenges of distinguishing past from current infections. Novel approaches to Lyme disease diagnosis including direct pathogen detection methods are needed to accurately discriminate between these clinical scenarios to avoid both under- and overdiagnosis of Lyme disease.
Footnotes
Acknowledgments
We thank the patients and families who agreed to study participation as well as study staff at each enrolling institution.
Authors' Contributions
P.M.L. and L.E.N. conceived the study and drafted the article. F.B., J.B., A.C.G., M.N.L., D.N., L.E.N., A.B.K., and A.D.T. supervised patient enrollment and data collection at each participating site. All performed critical article review and approved the final article draft. J.A.B. conducted the sample analysis, performed critical article review, and approved the final article draft.
Author Disclosure Statement
Dr. Branda has received research support from Pfizer, Zeus Scientific, bioMerieux, Immunetics, Alere and DiaSorin and has also received consulting fees from Roche Diagnostics, T2 Biosystems and DiaSorin.
Funding Information
This study was supported by the Global Lyme Alliance (Stanford, CT). The funder had no role in study conduct.