
Abstract
Background:
Mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) is a rare clinicoradiological syndrome characterized by transient mild encephalopathy and magnetic resonance imaging (MRI) findings of a reversible lesion in the splenium of the corpus callosum (SCC). Multiple causes have been proposed for the pathogenesis of MERS, with infection as the most pre-eminent.
Case Presentation:
We report the case of a 10-year-old girl with MERS due to scrub typhus. Her clinical manifestations of headache and drowsiness, together with lesions involving the SCC, as shown by MRI, and their complete resolution upon follow-up fulfilled the diagnosis of MERS. At the same time, the characteristic eschar of the skin and the positive Weil-Felix test result confirmed the existence of scrub typhus infection.
Conclusions:
To the best of our knowledge, we described the first pediatric case of MERS associated with scrub typhus. The case indicated that an MERS patient with fever should be considered as possibly having a scrub typhus infection. The characteristic black eschar of scrub typhus generally occurs after bite of mite that is important and useful to the doctor for making proper diagnosis.
Introduction
Scrub typhus, a zoonosis caused by Orientia tsutsugamushi, is characterized by high fever, eschar, rash, and lymphadenopathy. The neurological manifestations of scrub typhus are not uncommon, especially in the form of meningitis or meningoencephalitis.
Mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) is a clinicoradiological syndrome that was first identified by Tada et al. (2004). Its magnetic resonance imaging (MRI) findings are characterized with a reversible lesion in the splenium of the corpus callosum (SCC). The presence of reversible lesions involving the SCC has also been broadly named as reversible splenial lesion syndrome since 2011 (Garcia-Monco et al. 2011). The common symptoms include fever, headache, delirious behavior, disturbance of consciousness, and seizures. Complete resolution of the splenial lesions upon MRI repetition with full clinical recovery is the hallmark of this syndrome (Hoshino et al. 2012).
We report a case of a 10-year-old girl with MERS due to scrub typhus. To our knowledge, there is no report to date of MERS associated with scrub typhus in children. Therefore, we present herein the first case of MERS associated with scrub typhus in a child.
Case Presentation
A 10-year-old girl was admitted to our unit due to fever and headache for 6 days and rash for 3 days on August 5, 2020. She is the first child of her parents with an uneventful birth history. The parents were nonconsanguineous and healthy.
Physical examination at the time of admission revealed a body temperature of 39.9°C, pulse of 128/min, respiration of 34/min, and blood pressure of 98/60 mmHg. There were neck lymphadenopathy and erythematous maculopapular rash on her trunk and limbs. Neurological examination revealed drowsiness and lethargy but focal neurological and meningeal irritation signs were absent. Laboratory data (Table 1) showed low white blood cell count of 3.3 × 109 cells/L with 55.8% neutrophils, 113 g/L hemoglobin, decreased platelet of 62 × 109/L, elevated C-reactive protein of 33.6 mg/L, erythrocyte sedimentation rate of 2.0 mm/h, 85 U/L (normal range <50 U/L) alanine aminotransferase, 154 U/L (normal range, 15–60 U/L) aspartate aminotransferase, and 2.5 mM (normal range, 1.79–6.43 mM) urea.
Laboratory Test Value of the Patient
WBC, white blood cell count; Hb, hemoglobin; PLT, platelet; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; ALT, alanine aminotransferase; AST, aspartate aminotransferase; Cr, creatinine; CSF, cerebrospinal fluid; Leu of CSF, leukocyte count of CSF; Pro of CSF, protein level of CSF; Glu of CSF, glucose level of CSF.
No evidence of abnormality was found in other laboratory examinations, including blood glucose, electrolyte, HIV, syphilis, Epstein-Barr virus, influenza virus, adenovirus, respiratory syncytial virus, and Mycoplasma pneumonia. The chest X-ray of the patient was also normal. On day 2 after admission, brain MRI scans showed an ovoid shaped abnormal signal intensity in the SCC, which was hyperintense on T2-weighted and fluid attenuated inversion recovery (FLAIR) and hypointense on T1-weighted images (Fig. 1). The cerebrospinal fluid (CSF) examination revealed results that were within normal limits.
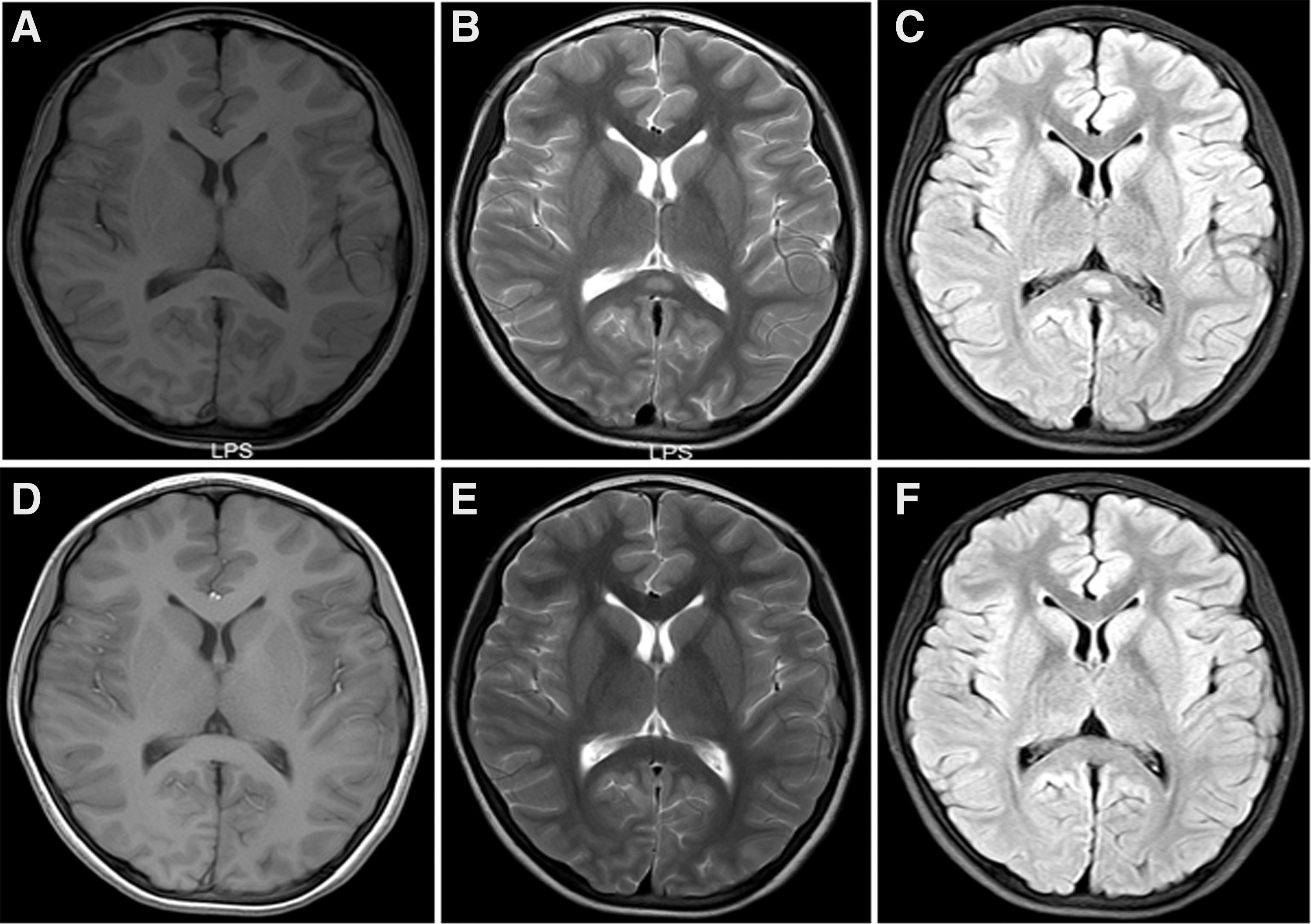
Brain MRI scans showed an ovoid shape with abnormal signal intensity in the SCC, which was hypointense on T1 weighted
The Pandy test was negative with a leukocyte count of 2/mm3, a protein level of 25.4 mg/dL, and a glucose level of 3.43 mM (serum glucose level of 5.9 mM). The oligoclonal bands and IgG index were within the normal ranges. The polymerase chain reaction for herpes simplex virus and enterovirus (HEV, EV71, CA16) of CSF were all negative, and cultures for the CSF and blood were negative. Electroencephalography was normal.
The patient's fever and headache did not improve and the rashes multiplied. Therefore, we again performed a physical examination whereby an eschar was noted on the right axilla, which was highly suggestive of scrub typhus (Fig. 2). Furthermore, we made a detailed inquiry about the contact environment. The patient self-reported that she had been in contact with grassy habitats around her house. Combined with a positive Weil-Felix test (OXK titer of 1:640), the diagnosis of scrub typhus infection could be established. Subsequently, she was administered with azithromycin (10 mg/kg per day) for 5 days, which was stopped because of the evident abdominal discomfort that ensued.
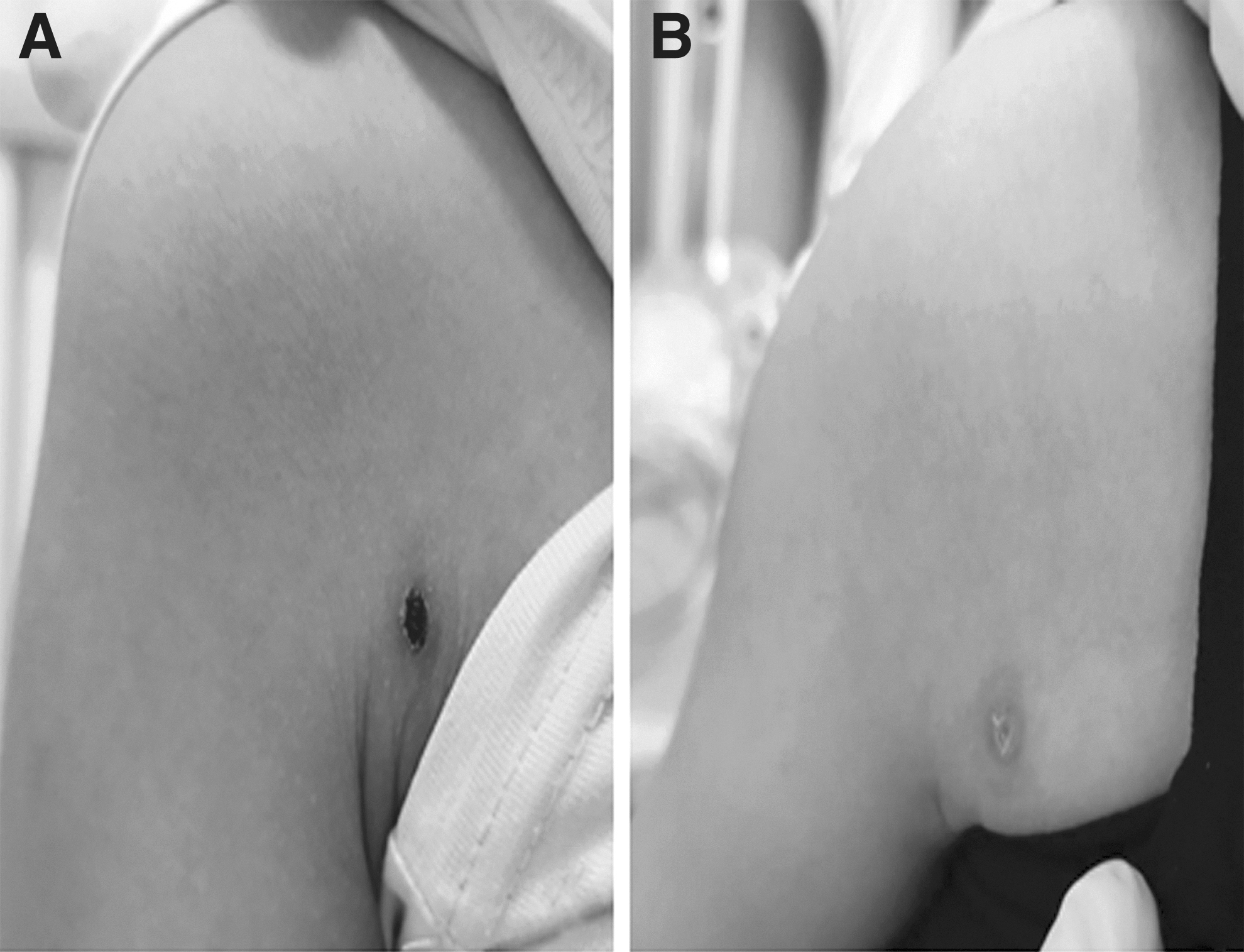
An eschar on the right side of the axilla in the patient with scrub typhus.
The patient's temperature improved and her headache was relieved, but her temperature fluctuated between 37.2°C and 38.0°C in the 3 days after withdrawal. Thereafter, doxycycline (2 mg/kg, twice a day) was added for 7 days. After 2 days, her fever and headache improved completely and she became alert. A repeat MRI scan of the brain 5 days later indicated that the lesion in the SCC had completely resolved (Fig. 1). Therefore, the final diagnosis of this patient was MERS associated with scrub typhus. She was discharged without any neurological complications.
Discussion and conclusions
Scrub typhus is a vector-borne rickettsial zoonotic disease, caused by the pathogen O. tsutsugamushi and transmitted by the bite of larval Leptotrombidium mite or chigger. Rodents are known as the main hosts for the trombiculid vector. It is an emerging infectious disease in many parts of the world and is endemic to the Asia-Pacific region, including but not limited to the region known as the “Tsutsugamushi Triangle” (Xu et al. 2017). The main clinical manifestations of scrub typhus are high fever, rash, lymphadenopathy, and early ulcer or eschar at the site bitten by tsutsugamushi. The characteristic eschar is located in hidden and moist parts of the body, such as the armpit, groin, perineum, and anus, among others. In some cases, scrub typhus leads to multiple organ dysfunctions, including nervous system involvement and death.
Although the pathophysiology of scrub typhus is not yet fully understood, in general, it is thought to be due to focal or disseminated vasculitis. Both humoral and cellular immunity are considered to play key roles in the development of vasculitis (Rajapakse et al. 2012). It is speculated that inflammatory cytokines such as interferon gamma (IFN-γ) and tumor necrosis factor-α can synergize with damage-associated molecular pattern (DAMP) molecules to cause impairments in the bloodbrain barrier (Soong et al. 2017). The neurological manifestations of scrub typhus are not uncommon and diverse.
Meningo-encephalitis is a classical neurological manifestation of scrub typhus, but cerebellitis, cranial nerve palsies, plexopathy, transverse myelitis, neuroleptic malignant syndrome, and Guillain-Barre syndrome have also been reported (Mahajan 2017). Nonetheless, the MRI findings of scrub typhus are rarely documented. In a sample of 37 patients with scrub typhus with neurological involvement, MRI was performed in 25 patients; among them, only 1 patient showed abnormal MRI findings of meningeal enhancement (Misra et al. 2015). In our patient, the presence of headache and drowsiness, together with lesions involving the SCC as shown by MRI, which completely resolved upon follow-up, fulfilled the diagnosis of MERS.
MERS is a rare clinicoradiological syndrome characterized by the MRI finding of a reversible lesion in the splenium of the SCC. MERS is divided into two types according to the lesion location: MERS type I, which has an isolated SCC lesion (ovoid or band shaped), and MERS type 2, which has extensive white matter and/or entire callosal lesions (Takanashi et al. 2010). In our patient, brain MRI consistently showed ovoid lesions that were centrally located in the SCC and hyperintense on T2 weighted and FLAIR and low on T1 weighted, which completely disappeared within 1 week. Therefore, our patient's condition was consistent with the diagnosis of MERS type I.
Multiple causes have been proposed for the pathogenesis of MERS, the most common cause is infection. The main pathogens of infection are viruses, including influenza virus, measles virus, human herpesvirus, rotavirus, adenovirus, Epstein-Barr virus, mumps virus, respiratory syncytial virus, and cytomegalovirus.
Other types of infectious pathogens include Streptococcus pneumoniae (Avcu et al. 2017), malaria parasites (Mawatari et al. 2018), and the new coronavirus (Hayashi et al. 2020, Bektas et al. 2021). In our patient, the characteristic eschar of the skin and the fourfold increase in the OXK titer confirmed the scrub typhus infection. There are only two adult cases of MERS associated with scrub typhus (Park et al. 2017, Shen et al. 2018) and, to the best of our knowledge, this is the first case reported fulfilling the diagnostic criteria for MERS associated with scrub typhus in a child.
The pathogenesis of MERS is still unknown. There are several hypotheses, including axonal or myelin edema, inflammatory infiltration, hyponatremia, and oxidative stress (Tada et al. 2004, Takanashi et al. 2009, Miyata et al. 2012). Patients with MERS resulting from various pathogen infections report increased serum and CSF cytokines, such as interleukin (IL)-6, IL-10, and IFN-γ. In contrast, scrub typhus infection can also release high levels of inflammatory cytokines in the target cells and damage the blood–brain barrier with DAMP (Soong et al. 2017). The coincidence of pathogenesis increases the possibility and credibility of the coexistence of scrub typhus and MERS. More studies are warranted to better understand this condition.
In summary, we describe the first pediatric case of MERS complicated with scrub typhus. The case indicated that an MERS patient with fever should be considered as possibly having a scrub typhus infection. The outcome of MERS is good, with the vast majority of patients achieving full recovery (Hoshino et al. 2012). The early recognition of MERS in patients can prevent the performance of unnecessary treatments and provide reassurance of the attainment of good outcomes.
Ethics Approval and Consent to Participate
The study was approved by the medical ethical committee of the Children's Hospital of Zhejiang University School of Medicine (Hangzhou, China). Written informed consents from the participants' legal guardian/next of kin were not required to participate in this study in accordance with the national legislation and the institutional requirements.
Consent for Publication
Both parents of the patient described have signed the consent form for publication, which is available for review by the editor of this journal.
Availability of Data and Materials
Data sharing is not applicable to this article as no data sets were generated or analyzed during this study.
Footnotes
Acknowledgments
We thank the patient's family for their participation in this study.
Authors' Contributions
X.L. analyzed the data and wrote the article. D.X., Y.Z., and B.C. collected the data and followed up the prognosis. Y.W. and Z.C. performed the study design and critical revision. All the authors contributed to article revision, read, and approved the submitted version.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.