
Abstract
Background:
The first Zika virus outbreak in U.S. Virgin Islands identified 1031 confirmed noncongenital Zika disease (n = 967) and infection (n = 64) cases during January 2016–January 2018; most cases (89%) occurred during July–December 2016.
Methods and Results:
The epidemic followed a continued point-source outbreak pattern. Evaluation of sociodemographic risk factors revealed that estates with higher unemployment, more houses connected to the public water system, and more newly built houses were significantly less likely to have Zika virus disease and infection cases. Increased temperature was associated with higher case counts, which suggests a seasonal association of this outbreak.
Conclusion:
Vector surveillance and control measures are needed to prevent future outbreaks.
Introduction
Vector-borne diseases are a growing public health problem in the United States because of increasingly frequent introduction of pathogens and vectors from endemic regions (Rosenberg et al, 2018). Zika virus (ZIKV), a mosquito-borne flavivirus, causes a range of syndromes from asymptomatic infection to fever, rash, Guillain-Barré syndrome, and congenital malformation, including microcephaly. ZIKV is primarily transmitted between people by the Aedes sp. mosquito vector, and by vertical transmission during pregnancy from mother to fetus, as well as during sex. ZIKV was detected in Brazil in May 2015 and rapidly spread throughout the Americas (Bonilla-Soto, 2018).
On January 3, 2016, the first case of Zika was reported to the U.S. Virgin Islands Department of Health (USVI DOH) by primary care providers and confirmed by the CDC Division of Vector-Borne Diseases. By July 3, 2016, ZIKV disease cases were identified on all USVI islands. Public health interventions enacted by the USVI DOH to mitigate the epidemic included educational outreach focused on the “Four Ds” of N-Diethyl-meta-toluamide (DEET) use, dress (covering exposed skin), dusk and dawn (avoiding outdoor activities when mosquitoes are most likely to bite people), and drain (removing free standing water); testing for all pregnant persons in the territory; and environmental mosquito spray treatment. Mosquito adulticiding and larviciding were conducted locally at residences of pregnant persons and public places.
USVI has three main islands: St. Thomas (population ∼52,000), St. Croix (population ∼51,000), and St. John (population ∼4000). Each island contains geographical divisions called estates (73 on St. Thomas, 211 on St. Croix, and 51 on St. John). USVI has a tropical climate with average temperatures ranging from 73°F to 89°F (23–32°C) and heaviest rainfall during May–November. Aedes aegypti, the primary ZIKV vector, is prevalent and has caused prior arbovirus epidemics, including the ∼1-year-long 2014 chikungunya virus epidemic and intermittent dengue epidemics in 2005 and 2012 (Colby et al, 2013, Feldstein et al, 2016, Mohammed et al, 2010).
We retrospectively investigated USVI's first ZIKV disease outbreak, described its epidemiology, and determined whether spatial-temporal, sociodemographic, or weather factors influenced ZIKV cases counts. Understanding factors that influenced the ZIKV outbreak can help direct interventions and mitigation strategies for future arboviral outbreaks.
Methods
Ethics and study population
This project was determined to be routine public health surveillance in response to an emerging outbreak by the Centers for Disease Control and Prevention and the USVI DOH. During January 2016–January 2018, serum samples and case reports were obtained by primary care providers, hospitals, and the USVI DOH for pregnant persons seeking prenatal care, and from people seeking health care in USVI with ≥2 of the following clinical signs: fever, rash, arthralgia, conjunctivitis, or myalgia.
Case definition
A confirmed noncongenital ZIKV disease case (clinically compatible illness, epidemiological linkage, and laboratory evidence of ZIKV infection) and confirmed noncongenital ZIKV infection case (no clinically compatible illness, but epidemiological linkage and laboratory evidence of ZIKV infection) were defined according to the Council of State and Territorial Epidemiologists case definition (Centers for Disease Control and Prevention (CDC), 2020).
Laboratory methods
Detection of ZIKV by polymerase chain reaction or ZIKV immunoglobulin M antibody with positive ZIKV neutralizing antibody titers and negative neutralizing antibody titers against dengue virus by plaque reduction neutralization testing (PRNT) was used to confirm ZIKV cases by the CDC Division of Vector-Borne Diseases Arboviral Diseases Branch laboratory in Colorado, and the Dengue Branch laboratory in Puerto Rico; the PRNT has a 90% cutoff value titer ≥10 in serum and ≥2 in cerebrospinal fluid to define positive specimens. Only confirmed noncongenital ZIKV disease and infection cases were included in this investigation, and will be described as “ZIKV cases” throughout the text for brevity.
Statistical analyses: spatial and sociodemographic
To evaluate if statistically significant spatial clustering or “hot spots” of ZIKV cases existed anywhere within USVI, we used a Global Moran's I test. Proximity was defined using a k-nearest neighbor spatial weights matrix (k = 8). Publicly available 2010 U.S. Census Bureau Data (US Census Bureau, 2010) that include sociodemographic variables (Supplementary Table S1) by estate were evaluated for association with ZIKV cases using a Poisson model and a negative binomial model; the negative binomial model was used because it was better suited to data variability. The evaluation of the year housing units built in USVI was divided into three time periods: before 1960, 1960–1989, and 1990 or newer.
Statistical analyses: weather
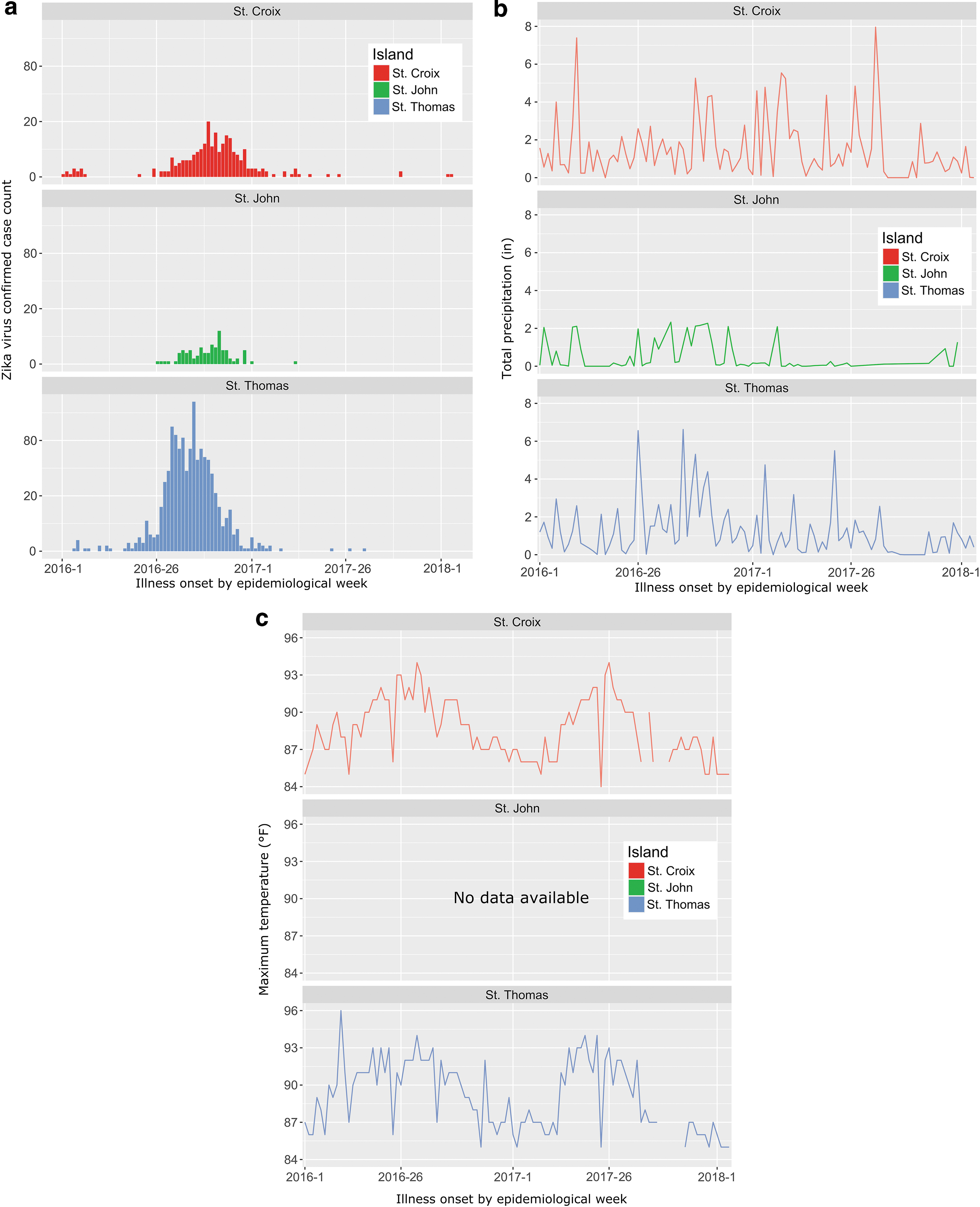
Weather data from each island (National Centers for Environmental Information, 2020) were obtained from active weather stations and compared with ZIKV cases by island: Station no. VQC00671740, Christiansted Fort, St. Croix; Station no. VQW00011640, Charlotte Amalie Cyril E King Airport, St. Thomas; and Station no. VQC00671980, Cruz Bay, St. John. Temperature and precipitation data were summarized into weekly high temperature and precipitation totals and compared with weekly ZIKV case counts by island using negative binomial regression models. To account for the delay between rainfall events, subsequent increased mosquito populations, and ZIKV transmission from mosquitoes to humans, case counts were compared with precipitation totals 3 weeks prior (Krow-Lucal et al, 2017, Winokur et al, 2020). ZIKV cases from 2 to 3 weeks prior were also included as a confounding variable to control for temporal autocorrelation in the analyses.
All data cleaning, statistical analysis, and mapping were performed using R 4.0.2 (R Core Team, 2015). Statistical models were generated by stepwise backward elimination of the least significant variables, and eliminated variables were assessed for confounding (a change of >30% in the main variable coefficient); the Aikake Information Criterion was used to compare goodness of fit for models.
Results
In total, 1031 confirmed, noncongenital ZIKV disease (n = 967) and infection cases (n = 64) were detected during January 3, 2016–January 24, 2018, with 919 (89%) detected during July–December 2016 (Fig. 1); no additional case has been detected as of July 1, 2022. Median patient age was 37 years (range: 0–84 years); 680/1028 (66%) were female, including 20 pregnant persons. ZIKV rates were higher on St. John (89 cases; 2225 cases/100,000 persons) and St. Thomas (685 cases; 1317 cases/100,000 persons), compared with St. Croix (257 cases; 504 cases/100,000 persons).
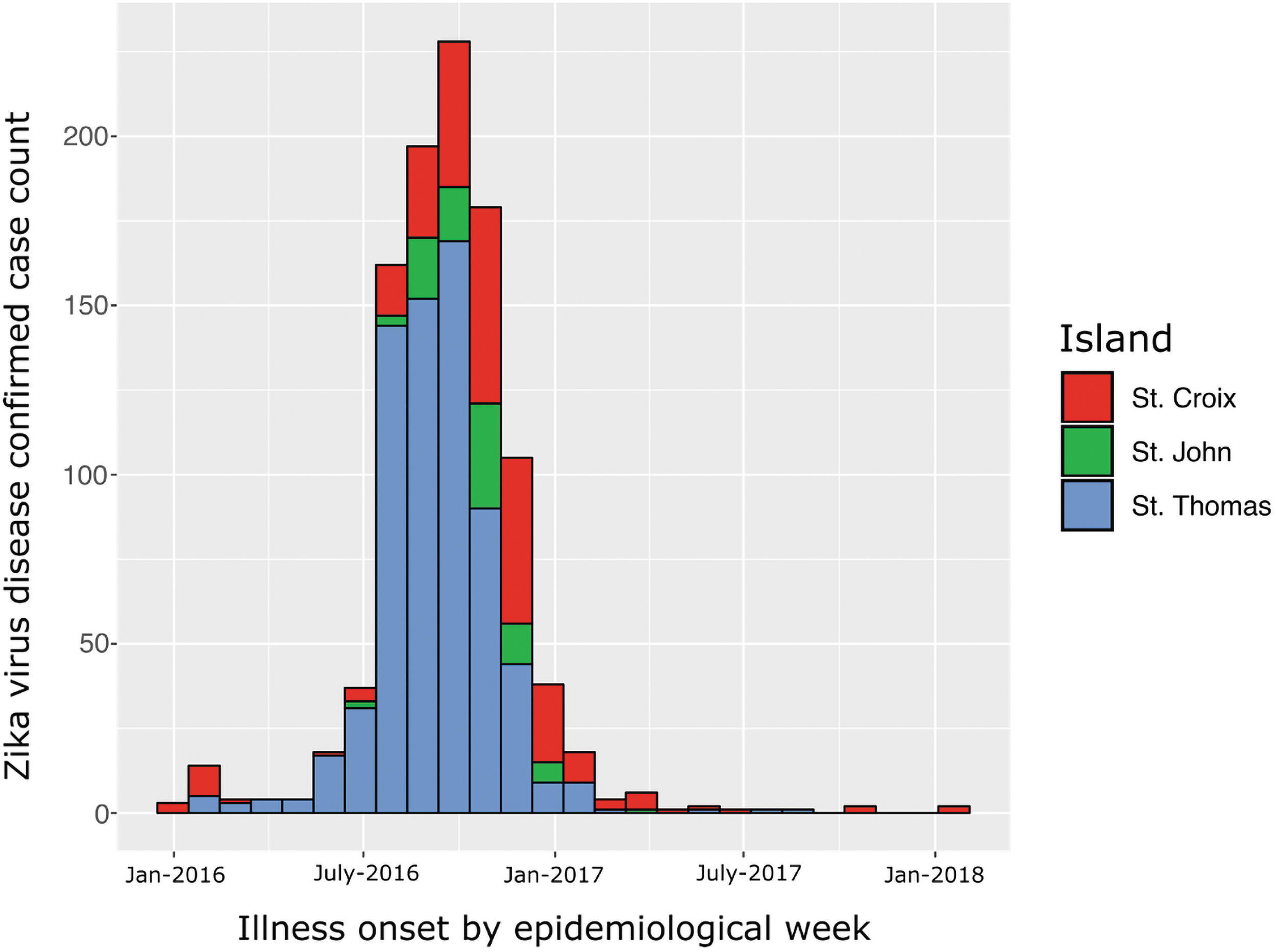
Confirmed noncongenital Zika virus disease and infection cases by month of illness onset in the U.S. Virgin Islands (St. Croix, St. John, and St. Thomas), January 2016–January 2018.
The global Moran's I statistic indicated spatial clustering of total cases (I = 0.24; p = 0.001), but not for case rate/week/estate (I = −0.02; p = 0.652). This finding suggests that the apparent clustering of case counts was associated with population distribution; mapping of cases against estate population also indicated a low and even distribution of case rate/estate throughout USVI (Supplementary Fig. S1). Only 739 (72%) cases had estate data available for sociodemographic analyses and some demographic variables were not recorded, and temperature data were not available from St. John.
Examination of demographic and socioeconomic variables using a negative binomial model with population as an offset revealed living in estates with higher unemployment (OR = 0.87, p = <0.00001), more houses connected to the public water system (OR = 0.98, p = <0.00001), and more newly built houses (OR = 0.99, p = 0.005) were protective against ZIKV infection and disease (Table 1). Weekly ZIKV cases were associated with increased temperature (St. Croix, St. Thomas), where each degree of high temperature increase (°F) would lead to 1.14–1.15 increase in risk; the maximum temperatures ranged from 74°F to 96°F. ZIKV cases detected 2 weeks prior were significantly associated with new ZIKV cases on all three islands (Table 2 and Fig. 2).
Sociodemographic Factors Significantly Associated with Number of Noncongenital Confirmed Disease and Infection Cases (n = 739) During the Zika Outbreak in the U.S. Virgin Islands, January 2016–January 2018, Using Generalized Linear Negative Binomial Models
Multivariable regression analyses of all sociodemographic variables (Supplementary Table S1) were performed, and nonsignificant variables were removed from the final model in a stepwise backward elimination, while controlling for confounding and assessing goodness of fit.
Assessment of Influence of Maximum Temperature (Range 74–96°F) and Total Precipitation (Range 0–7.96 Inches) Compared to Number of Noncongenital Confirmed Disease and Infection Cases (n = 1031) During the Zika Outbreak in the U.S. Virgin Islands, January 2016–January 2018, Using Generalized Linear Negative Binomial Models
Compared with case counts 3 weeks later.
Significant variable (p < 0.05).
Temperature data not available.
Discussion
ZIKV was rapidly transmitted throughout the USVI population in a continued point source outbreak. Our analyses found newer housing and public water supply systems, as well as higher unemployment rates, were protective against ZIKV disease (Table 1), while increased temperature on St. Croix and St. Thomas was associated with increased ZIKV cases (Table 2). Increased ZIKV cases were significantly associated to case counts on each island 2 weeks prior (Table 2); this finding was expected, but included in the weather model as a control factor, and further reinforces our epidemiological finding of a continued point source outbreak.
USVI residents in estates with greater proportions of new housing (i.e., built after 1990) and public water infrastructure had lower ZIKV case counts (Table 1). In Singapore, urban hydrology was a significant risk factor for dengue infection, particularly when increased drainage networks were noted in low-rise versus high-rise buildings (Seidahmed et al, 2018). Physical housing conditions have been identified as a risk factor for dengue infections (Mulligan et al, 2015). Lack of access to municipal water structure was also a risk factor for ZIKV infection in Rio de Janeiro, Brazil (Fuller et al, 2017).
Rainwater storage was found to be significantly associated with ZIKV microcephaly in Brazil, and the use of rainwater cisterns in USVI might offer more breeding habitats for Aedes mosquitoes (Campos et al, 2018). Regarding housing infrastructure, a USVI community assessment performed in June 2017 during the Zika outbreak found that 64.3% of houses had undamaged window screens, 39.9% had undamaged door screens, and 41.0% had air conditioning (Seger et al, 2019). Mitigation efforts to decrease local mosquito breeding habitats through enhancement of water and housing infrastructure in USVI might help decrease the impact of future arboviral disease epidemics.
Residents of estates with higher unemployment rates had fewer ZIKV cases (OR = 0.87). While unemployment could be related to socioeconomic status, poverty level of the adult population was not found to be significantly related to ZIKV cases. A systematic review of Aedes and arboviral diseases revealed approximately half of the 182 studies evaluated showed no significant relationship between socioeconomic status and disease (Whiteman et al, 2020).
Increased temperature was significantly associated with ZIKV cases (Table 2). The association of climate with arbovirus outbreaks has been previously reported, and advanced modeling efforts are used to help predict future arboviral epidemics, such as the AeDES project (Muñoz et al, 2020). A global analysis of islands identified minimum monthly temperatures of greater than 14.9°C (59°F) were associated with dengue virus transmission, where larger populations and increased precipitation were associated with increased dengue outbreak frequency (Feldstein et al, 2015). Analyses of dengue virus outbreaks over 8 years in Mexico showed similar temporality, and climate modeling in Barbados on dengue revealed increased minimum temperature to be associated with higher risks of an outbreak (Bisanzio et al, 2018, Lowe et al, 2018).
Due to the limited change of temperatures in a tropical climate, observation of increased temperatures and ZIKV cases counts in USVI may be related to the seasonality of arbovirus outbreaks in the Caribbean region, rather than the specific risk of ZIKV infection due to temperature increases in a small time period (e.g., days). The chikungunya virus outbreak in USVI peaked between July and December 2014 in a single year, similar to ZIKV (Feldstein et al, 2016). A review of the effects of climate on mosquito-borne diseases concluded that human activities and their impact on local ecology are much more significant, and predicting prevalence using climate-based models might be inappropriate (Reiter, 2001).
Flooding events due to Hurricanes Maria and Irma (both made landfall on USVI in September 2017) did not increase ZIKV disease cases in USVI (Fig. 1). In neighboring Puerto Rico, increased mosquito populations were observed 5 weeks after Hurricanes Maria and Irma, but there was no increased detection of dengue, chikungunya, or ZIKV in mosquitoes (Barrera et al, 2019). Other hurricane- or flood-related disasters have not been shown to increase transmission of arboviruses to humans or domestic animals in the United States, with the exception of the Red River flood of 1975 (Nasci and Moore, 1998).
A modeling study of ZIKV in Colombia revealed movement of infected people on a local scale was a driver of spread of disease (Rees et al, 2018). Examination of the epidemiological curve (Fig. 1), as well as increased ZIKV on each island following increases in cases 2 weeks prior (Table 2) further reinforce our conclusion that ZIKV followed a continued point source outbreak pattern. Whole genome sequencing analysis of 11 ZIKV specimens from USVI clustered with ZIKV from the United States as well as Puerto Rico, indicating rapid local spread after two key introductions (Black et al, 2017). Although a random serosurvey of ZIKV exposure was not performed in USVI, we suspect transmission rates eventually decreased as the susceptible naive population decreased on each island.
A potential limitation to this study is that ZIKV cases were identified by testing a subset of the population (i.e., pregnant persons and residents who sought health care). Confirmed ZIKV disease and infection cases represent only a proportion of all ZIKV infections in USVI, since some people might have been asymptomatic or not sought health care and testing if they had mild symptoms. Meta-analysis indicated 61.8% (95% CI: 33.0%–87.1%) of ZIKV infections are asymptomatic (Haby et al, 2018). Estate data were limited (72% of cases were identified to estate), which might have influenced estate-level analyses for spatial clustering and demographic and sociodemographic variables. However, the Moran statistic showed no significant difference between states when controlled by population, indicating our dataset had a wide distribution of cases represented. We also did not investigate nonlinear effects in our weather model (e.g., extreme rainfall events).
In conclusion, our findings show that ZIKV spread rapidly through USVI's island communities. The ZIKV epidemic followed a similar seasonal variation as previous epidemics in USVI (e.g., dengue, chikungunya). Recovery efforts following Hurricanes Maria and Irma will modernize housing and water infrastructure, which could lead to decreased risk of future arboviral outbreaks. In response to this outbreak, the USVI DOH established a biosafety level-3 laboratory on St. Croix during 2019 to increase surveillance capacity; local sample processing can provide rapid arbovirus detection. The USVI DOH also initiated an active mosquito surveillance program to monitor mosquito populations and test for arboviral diseases, using up to 500 fixed position mosquito traps with biweekly surveillance. Public health outreach included visiting residences to advise on mosquito prevention behaviors. Increasing mosquito bite prevention behaviors, reducing mosquito habitats, and modernizing housing infrastructure could help decrease the risk of future arboviral epidemics to USVI residents.
Footnotes
Acknowledgments
We thank the CDC Dengue and Arboviral Diseases Branches of the Division of Vector-Borne Diseases for laboratory testing, Kristine Bisgard and Fatima Coronado for article review and editing, and Brian Lewis for statistical consultation.
Authors' Contributions
All persons who meet ICJME authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.