
Abstract
Introduction:
Brucellosis remains an important public health problem in many developing countries. This study examines the serum levels of endocan, a novel immune-inflammatory marker, in this potentially difficult to diagnose disease, and their predictive diagnostic value.
Methods:
Fifty patients under follow-up with diagnoses of brucellosis between May 1, 2020, and December 1, 2020, and 50 healthy individuals constituting the control group were included in the study. Cases were classified as acute, subacute, or chronic, depending on the duration of their symptoms. Patients' plasma specimens were collected before the initiation of brucellosis treatment.
Results:
Serum endocan levels were higher among the patients with brucellosis than in the healthy control group (p < 0.001). Endocan levels also differed significantly among the patients with acute, subacute, and chronic brucellosis (p < 0.001 for all). Comparison of C-reactive protein (CRP) and the erythrocyte sedimentation rate (ESR) in the patients with acute, subacute, and chronic brucellosis revealed a significant difference only in terms of CRP levels between the acute and chronic patients (p = 0.018). No significant association was observed between serum endocan levels and growth in blood culture or serum agglutination test results in the patients with brucellosis (p > 0.05). However, a significant correlation was found between patients' CRP and ESR values and endocan levels (r = 0.572, and r = 0.415, respectively, p < 0.001). At a cutoff value of 597.35 pg/mL, serum endocan levels exhibited 90% sensitivity and 85% specificity in differentiating patients diagnosed with brucellosis from healthy individuals (area under the curve = 0.927, p < 0.001, 95% confidence interval = 0.877–0.977).
Conclusion:
Endocan may be a useful guide in differentiating patients with brucellosis from healthy individuals, and in distinguishing between acute, subacute, and chronic brucellosis. Ethics committee approval No: B.30.2.ATA.0.01.00/203.
Introduction
Brucellosis is a zoonotic disease caused by the Brucella bacteria species and transmitted through the consumption of infected animal products or contact with infected animal tissues or fluids. It represents an important public health problem in many developing countries (CDC 2017). More than 500,000 new cases are reported every year. However, due to reporting deficiencies and difficulties in diagnosis, the true prevalence is thought to be higher (Marvi et al. 2018).
Brucellosis typically manifests with nonspecific findings such as insidious-onset fever, malaise, night sweats, and arthralgia. Missed diagnoses therefore result in an increase in chronic and complicated cases (Galińska and Zagórski 2013, Ulu Kilic et al. 2013). The gold standard in the diagnosis of brucellosis is Brucella spp. growth in blood or tissue (CDC 2017). However, culture methods may result in diagnosis being delayed or unsuccessful due to late or lack of agent growth in culture. Despite being more widely used in the diagnosis of brucellosis, hematological parameters and serological tests are of limited value (Ulu Kilic et al. 2013). Rapid and simple novel markers for the early diagnosis of cases of brucellosis therefore need to be identified.
Endocan is a proteoglycan released from the surface of activated endothelial cells, particularly liver and kidney renal cells, and formerly known as “endothelial cell-specific molecule 1” (Luyt et al. 2008). Synthesis is induced by proinflammatory cytokines (Bechard et al. 2000). Studies have shown that endocan is associated with endothelial dysfunction and plays a role in inflammation in conditions such as sepsis and chronic kidney disease (Yilmaz et al. 2014, Pauly et al. 2016).
Although several studies have investigated the role of endocan, none has examined its role in brucellosis. The primary aim of the present study was to determine serum levels of endocan, a novel immune-inflammatory marker in patients diagnosed with brucellosis, and to evaluate whether it is a guiding marker in the differential diagnosis of acute, subacute, and chronic brucellosis. The second aim of the study was to compare serum endocan levels and laboratory findings in patients diagnosed with brucellosis.
Materials and Methods
Following receipt of local ethics committee approval (B.30.2.ATA.0.01.00/203), 50 patients aged 18 or older, with no additional disease, and diagnosed with brucellosis in our clinic between May 1, 2020, and December 1, 2020, were included in the study. Diagnosis of brucellosis was based on the Centers for Disease Control and Prevention Brucellosis Reference Guideline (CDC 2017). Depending on the duration of symptoms, cases were classified as acute (1–3 months), subacute (3–6 months), or chronic (>6 months).
Fifty healthy individuals aged 18 or older with the same demographic characteristics as the patients were enrolled as the control group. Exclusion criteria included the presence of any malignancy, hypertension, cardiovascular disease, diabetes mellitus, chronic kidney disease, or acute or chronic inflammatory/infectious disease. Informed consent was received from all participants.
Plasma specimens were collected from the patients in the study before commencement of brucellosis treatment. Blood specimens from the patient and control groups collected for routine biochemical tests were placed into tubes and left to stand for 10–20 min to coagulate. They were then centrifuged at +4°C for 15 min at 4000 rpm. The resulting serum samples were aliquoted and placed in a deep freeze at −80°C until being used in the analysis.
Patients' demographic data, blood leukocyte levels, neutrophil, lymphocyte, monocyte, and platelet counts, neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), lymphocyte/monocyte ratio (LMR), blood urea nitrogen, creatinine, total protein, albumin, aspartate aminotransferase (AST), alanine aminotransferase, total bilirubin, direct bilirubin, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), Brucella spp. growth in blood culture, and serum agglutination test (SAT) results were recorded.
Statistical analysis
SPSS 20.0 for Windows software (SPSS Inc.) was used for data recording and statistical analysis. Descriptive statistics were expressed as number and percentage for categorical variables and as mean ± standard deviation for numerical variables. Normality of distribution was assessed using the Kolmogorov–Smirnov test. Patient and control group laboratory results were compared using Student's t-test. One-way analysis of variance was used to compare the laboratory results of patients with acute, subacute, and chronic brucellosis, and the degree of significance between the groups was determined using the post hoc Tukey test.
Statistical analysis of the difference between the groups in terms of gender distribution was performed with the chi-squared test. Relationships between results were evaluated using Pearson analysis. The receiver operating characteristic (ROC) curve, an expression of a specific method's predictive power, was used to calculate endocan, CRP and ESR sensitivity, specificity, area under the curve (AUC), and cutoff values. A value of p < 0.05 was regarded as statistically significant.
Results
Eighteen (%36) of the patients followed up with diagnoses of brucellosis were men and 32 (%64) were women, while 23 (%46) of the control group were men and 27 (%54) were women. There was no significant gender difference between the two groups (p = 0.309). Blood leukocyte, neutrophil, and monocyte counts and NLR, LMR, AST, CRP, ESR, and endocan levels differed significantly between the patient and control groups (p < 0.05). Laboratory values in the patient and control groups are shown in Table 1. The most common symptoms of brucellosis were malaise (92%) and joint pain (74%).
Patient and Control Group Laboratory Results
Italic values: A value of p < 0.05 was regarded as statistically.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; LMR, lymphocyte to monocyte ratio; NLR, neutrophil to lymphocyte ratio; PLR, platelet to lymphocyte ratio; SD, standard deviation.
Fifteen (0.3%) brucellosis cases were acute, 15 (0.3%) were subacute, and 20 (0.4%) were chronic. Serum endocan values differed significantly between serum endocan acute and subacute cases, between the acute and chronic cases, and between the chronic and subacute cases (p < 0.001 for all). CRP values also differed significantly between the acute and chronic cases (p = 0.018) (Table 2).
Serum Endocan, C-Reactive Protein, and Erythrocyte Sedimentation Rate Levels in the Patients with Acute, Subacute, and Chronic Brucellosis
Italic values: A value of p < 0.05 was regarded as statistically.
Comparison of all groups.
Comparison of the acute and subacute patients.
Comparison of the acute and chronic patients.
Comparison of the subacute and chronic patients.
Brucella spp. growth was present in the blood cultures of 16 (32%) patients with brucellosis, but not in the other 34 (68%). SAT results were ≥1/160 in 14 (28%) of the patients with brucellosis and <1/160 in 36 (72%). No difference in blood culture was observed in terms of growth on blood culture or SAT results and serum endocan levels (Table 3).
A Comparison of Blood Culture and Wright Tube Agglutination Test Results and Serum Endocan Levels
SAT, serum agglutination test.
Brucellosis patients' CRP and ESR values were significantly correlated with endocan levels (r = 0.572 and 0.415, respectively, p < 0.001). Correlation results for laboratory parameters and serum endocan levels are shown in Table 4.
Correlation Between Brucellosis Patients' Laboratory Findings and Serum Endocan Levels
ROC curve analysis was applied to determine the diagnostic sensitivity and specificity of serum endocan, CRP, and ESR values in patients diagnosed with brucellosis. At a cutoff value of 597.35 pg/mL, serum endocan levels were 90% sensitive and 85% specific in differentiating patients with brucellosis from healthy individuals (AUC = 0.927, p < 0.001, 95% confidence interval [CI] = 0.877–0.977) (Fig. 1). ESR at a cutoff value of 9.5 mm/h was 68% sensitive and 79% specific in differentiating patients with brucellosis from healthy individuals (AUC = 0.778, p < 0.001, 95% CI = 0.682–0.874). CRP levels at a cutoff value of 3.7 mg/dL exhibited 72% sensitivity and 81% specificity in differentiating patients from healthy individuals (AUC = 0.914, p < 0.001, 95% CI = 0.860–0.968).
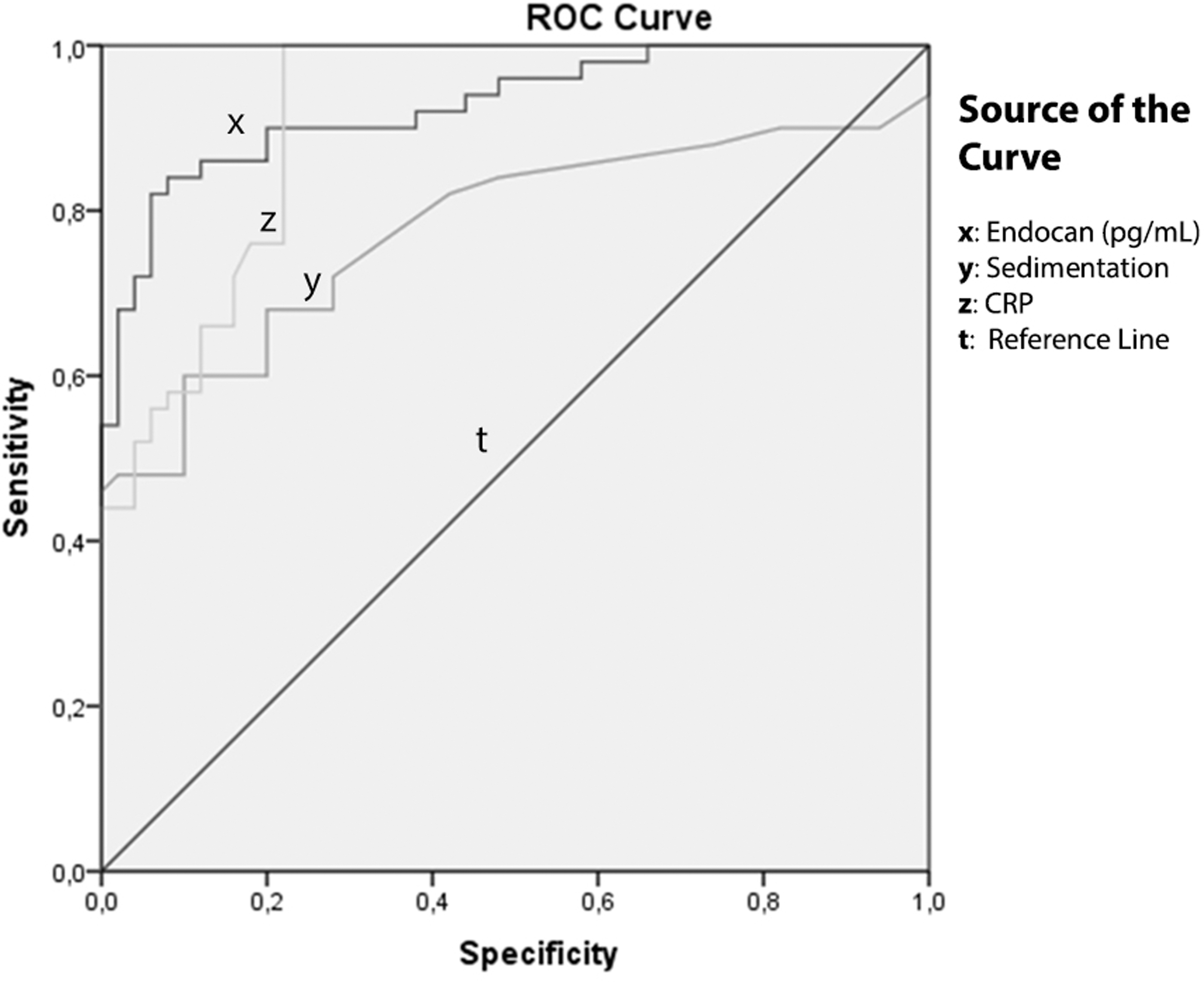
ROC curve analysis showing the diagnostic sensitivity and specificity of serum endocan, CRP, and sedimentation levels in patients with brucellosis. CRP, C-reactive protein; ROC, receiver operating characteristic.
Discussion
Serum endocan levels in this study were significantly higher in patients with brucellosis than in the control group. A significant powerful correlation was observed between endocan levels and both CRP and ESR. Serum endocan exhibited high sensitivity and specificity (90% and 85%, respectively) in differentiating patients diagnosed with brucellosis from healthy individuals. No significant difference in serum endocan levels was observed between patients with and without Brucella spp. in blood culture (p > 0.05). However, serum endocan levels differed significantly in patients with acute, subacute, and chronic brucellosis (p < 0.001 for all).
Endocan is a novel immune-inflammatory marker synthesized from endothelial cells (Balta et al. 2015). It is found at low levels in the blood of healthy individuals. The upregulation of endocan under the effect of proinflammatory cytokines has led to suspicion that it may be involved in the regulation of inflammatory reaction (De Freitas Caires et al. 2018). Several publications have shown a relationship between endothelial dysfunction and inflammatory diseases (Balta et al. 2015, Celik et al. 2015, Icli et al. 2016). Increasing plasma endocan levels during the follow-up of septic patients have been described as a potential predictor of acute respiratory distress syndrome development and to be closely associated with it (Ioakeimidou et al. 2017, De Freitas Caires et al. 2018).
A correlation between serum endocan and inflammatory parameters has been reported in the cardiovascular patient group with inflammation and in patients with psoriasis (Balta et al. 2013, Yilmaz et al. 2014). A significant association has also been shown between serum endocan levels and mortality and intensive care requirements in patients with COVID-19 (Medetalibeyoglu et al. 2021).
Tissue damage and infectious diseases are classic triggers of inflammation, one such disease being brucellosis. Various physiological and pathological processes can trigger inflammation, and the response to all these stimuli is similar (Pober and Sessa 2007). Changes occur in serum endocan levels in several inflammatory conditions, and several studies have reported a relationship between endocan and cytokines involved in inflammation (Lee et al. 2019, Faruk Ozdemir et al. 2020). However, no studies have evaluated serum endocan levels in patients with brucellosis. Serum endocan levels in the present study were significantly higher in the patients diagnosed with brucellosis compared with the control group. Significant differences were also observed in serum endocan levels among patients with acute, subacute, and chronic brucellosis.
Changes may occur in the distribution of blood leukocyte cells and platelet levels in association with systemic inflammation (Medzhitov et al. 2008). LMR, NLR, and PLR are affected as a result of systemic inflammation and are reported to be potentially useful in various diseases (Aydin et al. 2016, Sen et al. 2016, Peng et al. 2017). Due to the close relationship between infection and inflammation, these parameters cannot, unfortunately, be used in the definite diagnosis of brucellosis. Studies comparing patients with brucellosis and healthy individuals have shown variations in these values (Aktar et al. 2016, Aydin et al. 2016, Bozdemir et al. 2017).
In the present study, blood leukocyte levels and neutrophil counts were lower in the patients with brucellosis than in the healthy controls, while monocyte counts were higher. NLR and LMR also differed significantly between the patient and control groups. A significant negative correlation was determined between serum endocan levels in patients with brucellosis and neutrophil counts and NLR.
Serum or plasma acute-phase proteins increase or decrease in case of infection, tissue damage, and immunological and inflammatory conditions. These proteins are synthesized from the liver under the effect of cytokines and indicate the presence of nonspecific inflammation (Baumann and Gauildie 1994). Increases in serum levels in acute events generally parallel the severity and diffusion of inflammation, while synthesis may be suppressed in chronic inflammation (Ishak and Hassan 1989). CRP and ESR values were significantly higher in the patients with brucellosis than in the healthy controls in the present study, and a significant correlation was observed between serum endocan levels and CRP and ESR values.
Significant differences were found in serum endocan levels between patients with acute, subacute, and chronic brucellosis. The significant variation in serum endocan levels in the patient groups was not observed in CRP or ESR. A significant difference in CRP levels was only observed between the acute and chronic brucellosis subgroups. Acute-phase reactants close to normal limits may not be diagnostically useful to the clinician in subacute and chronic brucellosis with nonspecific clinical symptoms and findings. The fact that serodiagnostic tests are confusing and that culture tests do not always give positive results makes the diagnosis of brucellosis in this patient group difficult.
The findings of the present study suggest that endocan may be a valuable biochemical marker capable of use both in the diagnosis of brucellosis and also in differentiating acute, subacute, and chronic cases. In addition, serum endocan levels have greater sensitivity and specificity in differentiating patients with brucellosis from healthy individuals than CRP and ESR. This means that serum endocan levels are more useful than other acute-phase reactants in cases in which diagnostic difficulty is experienced.
Since brucellosis can affect any organ and all body systems, the findings produced by the infection are not pathognomonic. The entity can therefore be easily confused with other medical conditions and diseases (Franco et al. 2007). Diagnosis of this infection may even be missed in regions where the disease is endemic. One study reported that 52 (59.1%) patients with proven disease had previously been examined by a physician but had been incorrectly diagnosed (Yilmaz et al. 2016). Overdiagnosis of brucellosis can also lead to unnecessary long-term drug use, undesirable drug side effects, and other diseases being overlooked. Accurate diagnosis of brucellosis and appropriate patient management are therefore highly important. Growth of Brucella spp. in blood cultures confirms the presence of Brucella at low or threshold antibody titers when serological tests are negative (Shemesh and Yagupsky 2011).
However, the fact that culture techniques are laborious and costly, require extra laboratory space, and are time-consuming can result in delays in diagnosis. No statistically significant difference in serum endocan levels was observed in the present study between patients with Brucella spp. growth in blood culture and those with no growth (p = 0.459). Endocan can therefore be used as an auxiliary test in the diagnosis of brucellosis in case of absence of agent growth or when culture techniques are unavailable.
Conclusion
In conclusion, serum endocan levels are higher in patients with brucellosis compared with healthy individuals. They are also highly sensitive and specific in differentiating patients with brucellosis from healthy individuals. Endocan is also a useful marker in the differential diagnosis of acute, subacute, and chronic brucellosis. The use of endocan will prevent diagnosis being missed in regions where brucellosis is endemic and also help prevent disease-related morbidity by assisting with diagnosis in the early period alongside other laboratory parameters.
Footnotes
Authors' Contributions
H.A.: Concept, design, supervision, resources, materials, data collection and/or processing, literature search, and writing the article. E.L.: Concept, design, supervision, analysis and/or interpretation, literature search, and writing the article.
Ethics Approval
Approval for this prospective cohort study was granted by the Atatürk University Medical Faculty Ethics Committee (B.30.2.ATA.0.01.00/203).
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this study.