
Abstract
Background:
Severe fever with thrombocytopenia syndrome (SFTS), an emerging viral infectious disease, is mainly transmitted by ticks in the surrounding environment. Clinical progress and risk factors for prognosis in SFTS patients were not yet fully understood. Thus, the objective of this study was to analyze clinical progression and laboratory data related to the prognosis of South Korean SFTS patients in a single institution from 2014 to 2021.
Materials and Methods:
Fifty-three confirmed SFTS patients from August 2014 to September 2021 at Gyeongsang National University Hospital (GNUH) in Jinju, South Korea were enrolled. Electronic medical records of SFTS patients' demographic features, clinical data, and laboratory data were retrospectively reviewed. Risk factors for fatality were statistically analyzed by classifying enrolled patients into fatal and non-fatal groups.
Results:
The mean age of patients in the fatal group was significantly higher than that in the non-fatal group (p = 0.036). Hemorrhagic manifestations (p = 0.001) and multiple organ dysfunction (MOD) (p < 0.001) were significantly common in the fatal group. Age, hemorrhagic manifestations, and MOD were also associated with death (p = 0.001, p = 0.008, and p = 0.041, respectively), with adjusted hazard ratios (aHRs) of 1.14, 18.25, and 2.36, respectively. Onset of illness to admission was also significantly associated with death (p = 0.005), with aHR of 0.48. Age, interval from onset of illness to admission, hemorrhagic manifestations, and MOD were found to be variables related to the fatality of SFTS patients.
Conclusion:
Laboratory test results showed a significant difference between the fatal group and the non-fatal group, but they did not have a statistically significant effect on the prognosis of SFTS patients.
Introduction
Severe fever with thrombocytopenia syndrome (SFTS) is an emerging viral infectious disease. It was first reported in China in 2011 (Yu et al, 2011). The SFTS has attracted attention as a potential pandemic disease due to its common transmission vector and escalating incidence. The severe fever with thrombocytopenia-causing phlebovirus belongs to the genus bandavirus in the family Phenuiviridae, order Bunyavirales.
The International Committee on Taxonomy of Viruses (ICTV) officially named the virus Dabie bandavirus (ICTV, 2020). In addition, this virus has the name as Severe Fever with Thrombocytopenia Syndrome Virus (SFTSV), which is derived from the symptoms, and is more widely used than the official name. It can be classified into at least six genotypes (Fu et al, 2016). As with other members of the Phenuiviridae family, transmission of SFTSV is vector-borne, primarily through tick bite. The ticks that transmit the SFTSV virus are Haemophysalis longicornis, Amblyomma testudinarium, and Ixodes nipponensis (Fu et al, 2016, Niu et al, 2013, Yoo et al, 2018) that can be found in the surrounding environment, including domestic animals (Tenquist and Charleston, 2001, Zhao et al, 2020).
Human-to-human transmissions are also possible (Gai et al, 2012a, Kim et al, 2015, Yoo et al, 2016, 2018). The SFTS cases were mainly reported in East Asia. For example, 13,824 cases in China (2010–2019) (Huang et al, 2021), 1241 cases in Korea (2015–2020) (KCDA, 2020), and 641 cases in Japan (2013–2021) (NIoI, 2020) have been reported. The SFTS-like virus infection has also been reported in the United States (Wormser et al, 2020). The average fatality rate was 5.2% in China (Huang et al, 2021), 16.8% in Korea (KCDA, 2020), and 12.5% in Japan (NIoI, 2020).
Typical clinical features of SFTS are fever, gastrointestinal (GI) symptoms, neurological symptoms, and hemorrhagic manifestations. Most patients have thrombocytopenia and leukopenia, with elevated alanine aminotransferase (ALT), aspartate aminotransferase (AST), and lactate dehydrogenase (LDH). The clinical spectrum range of SFTS varies from asymptomatic to fatal (He et al, 2020). Laboratory confirmation is essential for the diagnosis of SFTS. Up to now, reverse transcription polymerase chain reaction is a specific tool for the detection and diagnosis of viral RNA.
Effective therapies or vaccines for SFTS have not, as yet, been established (Liu et al, 2013, 2014). As of now, conservative treatments, antiviral agents, and plasma exchanges are common treatment strategies (Yoo et al, 2019). If treatments are not received at an early stage of diagnosis, the mortality rate could increase. Thus, it may be necessary to know the risk factors that can help us evaluate the prognosis and establish treatment plans at the early stage of diagnosis. However, only a limited number of studies have described the progression of the SFTS (Choi et al, 2016, Shin et al, 2015).
In addition, most studies describing the clinical progressions and risk factors for death in SFTS were conducted in China. Studies in other countries are not yet active. Since the most common SFTSV genotype by country, ranging from F, A, and D in China to B genotype in Korea and Japan (Seo et al, 2021), it might be necessary to identify characteristics of the disease in each country and respond accordingly.
Thus, clinical progression and laboratory data of South Korean SFTS patients in a single institution from 2014 to 2021 were analyzed in this study. We attempted to determine general clinical characteristics of Korean patients and identify risk factors that could differentiate fatal cases from non-fatal cases. We retrospectively analyzed clinical signs and laboratory data of 53 confirmed cases during hospitalization. In addition, we applied a time-dependent statistical analysis model and performed survival analysis to identify prognostic factors. We believe that this study could serve as a basis for regional studies of SFTS. Results of this study would be also helpful in the establishment of a therapeutic strategy for SFTS patients.
Materials and Methods
Study subjects
A total of 53 confirmed SFTS patients from August 2014 to September 2021 were enrolled. All patients visited Gyeongsang National University Hospital (GNUH) in Jinju, South Korea for suspected SFTS. They were admitted to the Department of Infectious Diseases. The SFTS confirmatory tests were performed at the Korea Disease Control and Prevention Agency (KCDC) using in-house SFTS real time-PCR diagnosis kits. This study was approved by the Institutional Review Board of GNUH (IRB no. GNUH 2021-09-017).
Data collection
Electronic medical records (EMRs) of SFTS patients' demographic features, clinical data, and laboratory data were retrospectively reviewed. Demographic features (including sex, age, illness onset, and underlying disease) and clinical data (including sign and symptoms, final outcome (death or survival), and laboratory test results) were retrieved from EMRs. Complete blood count was determined by either XN-9000 (Sysmex Corporation, Kobe, Japan) or ADVIA 2120 (Siemens Healthcare Diagnostics, Tarrytown, NY). Serum laboratory parameters were measured using COBAS 8000 (Roche Diagnostic, Basel, Switzerland).
Coagulation factors were determined using ACL TOP 750 (Werfen, Munich, Germany). Dynamic blood and serum analyses results were presented according to the number of days after patients' admission. Multiple organ dysfunction (MOD) was defined when two or more of the following conditions existed: (1) hypoxia requiring respirator-assisted ventilation for at least 3–5 days; (2) serum bilirubin ≥2–3 mg/dL or liver function tests ≥twice normal; (3) oliguria ≤479 mL/24 h or rising creatinine (≥2–3 mg/dL); (4) ileus with intolerance to enteral feeding >5 days; (5) prothrombin time (PT) (PT) and PTT (partial thromboplastin time) increase >25% or platelet counts <50–80,000; (6) confusion and mild disorientation; and (7) decreased ejection fraction or capillary leak syndrome (Bone et al, 1992).
Statistical analysis
For categorical variables, results are presented as frequencies and percentages. For continuous variables, results are presented as means and standard deviations, and interquartile range values. To compare clinical and laboratory parameters, the Chi-squared test was used for comparing qualitative data and a paired t-test was used for comparing quantitative data. In addition, the linear mixed model (LMM) was used for comparing laboratory parameters between fatal and non-fatal groups. Time-dependent Cox's proportional hazard model was used to analyze time varying lab data.
Other variables were analyzed by Cox's proportional hazard model. All statistical analyses were conducted using R software, version “4.1.2” (R Core Team. R Foundation for Statistical Computing, Vienna, Austria, 2021), the package survival 3.4-0 (Therneau et al, 2022). p Value <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of subjects
From August 2014 to September 2021, a total of 57 patients with SFTS confirmed by real-time PCR at GNUH were analyzed. Four patients were excluded due to missing detailed clinical and laboratory data. Thus, 53 patients were finally included in the study. The average age of the total patient group was 68.4 years, and the male to female ratio was 0.83 with 24 (45.3%) males and 29 (54.7%) females (Table 1). The occupations of the patients were diverse, with farmers showing the highest frequency (n = 18, 34%).
Demographic and Clinical Characteristics of Study Subjects
p Value relates the difference between the fatal and non-fatal groups.
CVD, cardiovascular disease; DIC, disseminated intravascular coagulation; DM, diabetes mellitus; GI, gastrointestinal; HTN, hypertension; LN, lymph node; MOD, multiorgan dysfunction; SD, standard deviation.
The SFTS virus is mainly spread through tick bites, but occupations exposed to more ticks (e.g., farmers) did not appear significantly more in the fatal group (p = 0.469). All patients had a history of field exposure to potential tick bites before admission. Types of underlying diseases associated with patients were as follows: hypertension (34%), diabetes mellitus (22.6%), cardiovascular disease (7.5%), and others (15.1%). Among a total of 53 patients, 9 patients expired during the study period, with a case-fatality rate of 17%. Study patients were divided into fatal and non-fatal groups depending on survival. All patients in the fatal group died within 7 days of admission.
The mean age of the fatal group patients was 76.3 years, and the male to female ratio was 0.5 with 3 (33.3%) males and 6 (67%) females. The mean age of the non-fatal group of patients was 66.7 years, and the male to female ratio was 0.91 with 21 (47.7%) males and 23 (52.3%) females. Although the mean age of the patients in the fatal group was significantly (p = 0.036) higher than that in the non-fatal group, there was no significant (p = 0.487) difference in the sex ratio between the two groups (Table 1).
The mean time from onset illness to admission to the hospital was 3.7 days for total patients, 2.2 days for patients in the fatal group, and 4.0 days for the non-fatal group. The mean time was statistically significantly shorter in the fatal group (p = 0.029). Main symptoms accompanying hospitalization were as follows in order of frequency from high to low: GI symptoms including lack of appetite, nausea, vomiting, and diarrhea (81%); neurologic symptoms such as lethargy, apathy, muscular tremor, and convulsions (45.3%); and hemorrhagic manifestations such as ecchymosis, hematuria, oral suction site bleeding (13.2%), fever over 39°C (11.3%), lymph node enlargement (7.5%), disseminated intravascular coagulation (DIC) (5.7%), and coma (3.8%).
Hemorrhagic manifestations were significantly more common in the fatal group (p = 0.001) than in the non-fatal group. MOD was observed only in 15.9% of patients in the non-fatal group. However, in the fatal group, all nine patients showed MOD (p < 0.001).
Dynamics of laboratory parameters
Dynamic changes of the following 13 laboratory parameters were tracked to analyze clinical features of disease progression and risk factors associated with fatal outcome: white blood cell (WBC), neutrophil, lymphocyte, platelet, PT, activated partial thromboplastin time (aPTT), albumin, AST, ALT, blood urea nitrogen (BUN), creatinine, LDH, and creatinine kinase (CK). Daily data of hematologic and biochemical parameters from admission day (day 0) to day 20 are shown in Figs. 1 and 2. During day 1–7, SFTS patients had distinct leukocytopenia and thrombocytopenia in both fatal and non-fatal groups. Platelet and neutrophil counts decreased to a minimum on day 3; lymphocytes were decreased at admission but steadily increased thereafter in both groups. They were normalized at about day 7, for the non-fatal group.

Dynamics of hematologic parameters during whole admission period. Parameters of 53 patients with SFTS are illustrated with box and whisker plots based on the number of days after admission. p Values at the corner of each plot indicate statistical significance between averages of the two patient groups over 20 days. aPTT, activated partial thromboplastin time; INR, international normalized ratio; PT, prothrombin time; SFTS, severe fever with thrombocytopenia syndrome; WBC, whole blood cell.

Dynamics of clinical chemistry parameters during whole admission period. ALT, alanine aminotransferase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; CK, creatinine kinase; LDH, lactate dehydrogenase.
In the coagulation test, aPTT was prolonged at admission, whereas PT was rarely extended. Although aPTT was normalized in the non-fatal group gradually, its levels rose dramatically in the fatal group as the patient's condition deteriorated rapidly. Serum albumin level decreased whereas albumin, aspartate aminotransferase (AST), ALT, BUN, creatinine, LDH, and CK levels increased progressively during the first week in the fatal group, reaching maximum levels before the patient's death. All those parameters in the fatal group were significantly different from those in the non-fatal group (all p < 0.05).
Since all patients in the fatal group died within 7 days of admission, we tried to find a factor that could differentiate prognosis within a short period of time by analyzing laboratory parameters up to day 7. For this purpose, the time concept was introduced to see whether there were any parameters showing a significant difference between the non-fatal group and the fatal group at the time of hospitalization (day 0), at the interval from day 1 to 3, and at the interval from day 4 to 7. The analysis was conducted using an LMM (Figs. 3 and 4).

Hematologic parameters during day 0–7 after hospital admission were separately analyzed. Data were divided into three time periods (day 0, 1–3, 4–7). The difference between groups was clearly visible around day 1–3, but not on day 0.
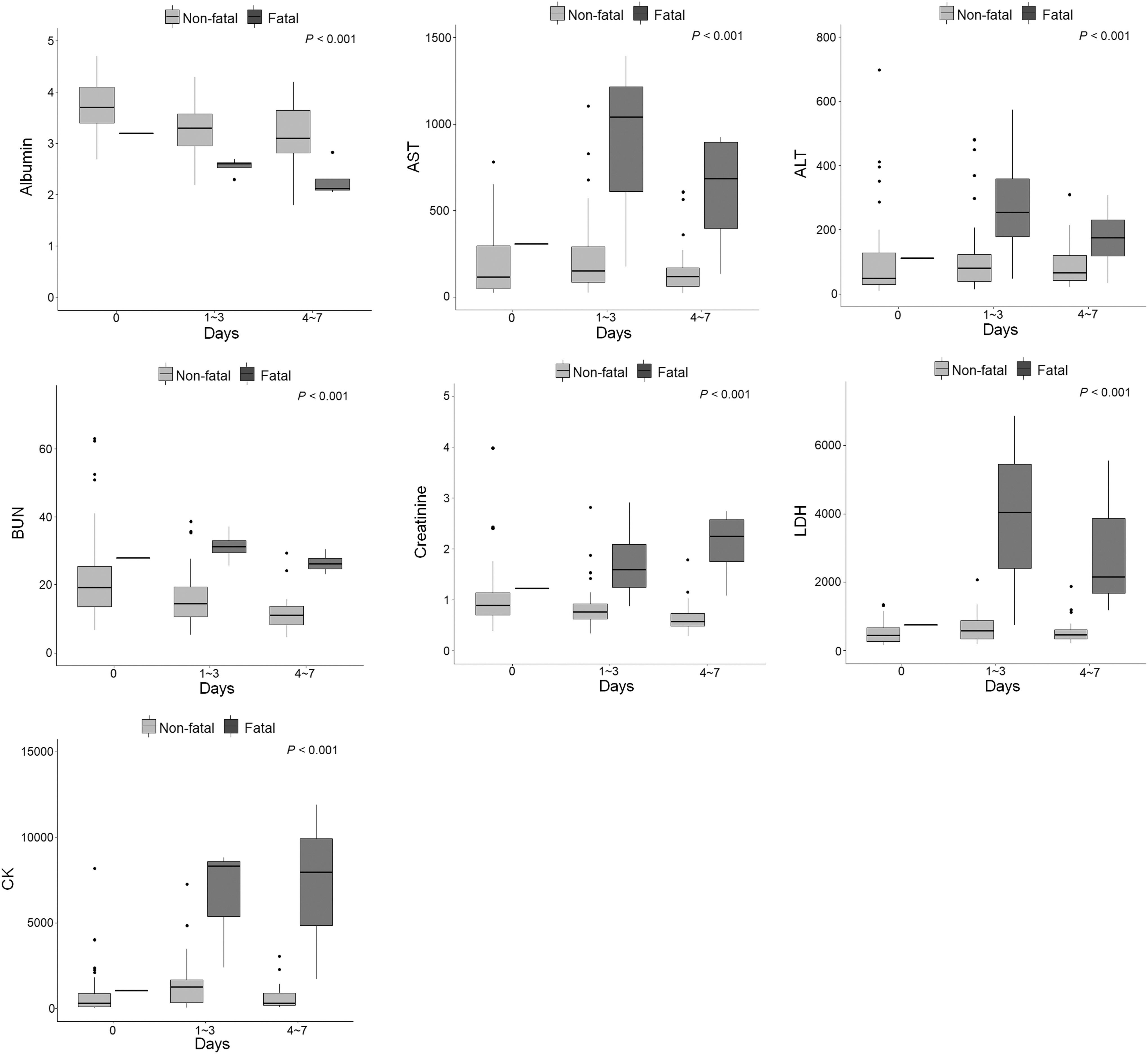
Clinical chemistry parameters during day 0–7 after hospital admission.
The analysis results showed no differences from analysis results of the total hospitalization period of day 20. PT, aPTT, ALT, AST, albumin, BUN, creatinine, LDH, and CK levels were significantly different between the two groups (all p < 0.001). However, there was no significant difference in WBC (p = 0.442), neutrophil (p = 0.706), lymphocyte (p = 0.136), or platelet (p = 0.271) between the two groups.
Risk factors for fatality
As a result of a univariate survival analysis conducted to find variables influencing patient's mortality (Table 2), it was found that a patient's age had a significant (p = 0.04) effect on the mortality rate among demographical characteristics. For every 1-year increase in patient age, the mortality rate was increased by a factor of 1.07 (HR = 1.07). The gender of the patient had no significant effect on mortality. Among clinical characteristics, the presence of hemorrhagic manifestations (HR = 14.17), DIC (HR = 6.69), and MOD (HR = 1.89) significantly increased the mortality rate of patients (p < 0.001, p = 0.018, and p = 0.001, respectively). A shorter interval from the onset of illness to admission was associated with a significantly higher mortality rate (HR = 0.612, p = 0.04).
Risk Factors for Fatality
ALT, serum alanine aminotransferase; aPTT, activated partial thromboplastin time; AST, serum aspartate aminotransferase; BUN, blood urea nitrogen; CI, confidence interval; CK, creatinine kinase; HR, hazard ratio; INR, international normalized ratio; LDH, lactate dehydrogenase; PT, prothrombin time; WBC, whole blood cell.
Among laboratory parameters, PT (INR ≥1.2), aPTT (≥100 s), albumin (<3.5 g/dL), AST (>400 U/L), ALT (>200 U/L), BUN (>20 mg/dL), creatinine (>1.2 mg/dL), LDH (>800 U/L), and CK (>10,000 U/L) were significantly associated with mortality. However, WBC (<2000/μL), neutrophil (<1500/μL), lymphocyte (< 500/μL), and platelet (<50 k/μg) had no significant effect on the mortality.
The levels outside the reference value for albumin (<3.5 g/dL) and BUN (>20 mg/dL) were observed only in some of the non-fatal group patients. However, all the patients in the fatal group had an albumin and BUN level that greatly deviated from reference values. For this reason, HR for albumin and BUN were exceptionally high (HR = 4.53 × 108 for albumin and HR = 4.99 × 109 for BUN).
In multivariate analysis, results were corrected by considering the increase or decrease of other variables. Age, hemorrhagic manifestations, and MOD were associated with death (p = 0.001, p = 0.008, and p = 0.041, respectively), with adjusted HRs of 1.14, 18.25, and 2.36, respectively. The onset of illness to admission was also significantly associated with death (p = 0.005), with an adjusted HR of 0.48. Laboratory parameters were not significant in multivariate analysis.
Discussion
In this study, data from 53 SFTS patients at a tertiary hospital in Korea from year 2014 to 2021 were analyzed. We tried to investigate clinical characteristics and identify factors related to the prognosis of Korean SFTS patients. For Korean SFTS patients, all fatal patients expired within 7 days, showing very rapid and adverse progression without following the three distinct stages of fever, MOD, and convalescence stage over 3 weeks described in a previous study (Gai et al, 2012b). Among demographic characteristics, age showed a significant difference between fatal and non-fatal groups.
Among clinical characteristics, hemorrhagic manifestations, neurologic symptoms, DIC, and MOD showed significant differences between the two groups. Through multivariate survival analysis, it was confirmed that older age, the presence of hemorrhagic manifestation and MOD, and shorter interval from onset illness to admission were significant risk factors for mortality. In laboratory data, all biochemical parameters showed statistically significant differences between fatal and non-fatal groups. However, biochemical parameters were not significantly associated with prognosis in a multivariate survival analysis.
Patients in this study had an older mean age than those of previous studies in China (Gai et al, 2012b, Li et al, 2018, Yun et al, 2020). However, the mean age of patients in the present study was similar to those of previous studies in Korea (Choi et al, 2016, Shin et al, 2015). The difference in the demographic structure of the two countries seems to be reflected in study results between the two countries. The mean age of patients in the fatal group was about 10 years older than those of the non-fatal group (p = 0.036) in the present study.
In multivariate survival analysis, age was analyzed as a risk factor that could increase the mortality rate by 1.138 times for every 1 year increase in age, similar to a previous study showing that age was an important risk factor for a patient's death (He et al, 2020). Among clinical characteristics, the presence of hemorrhagic manifestations, neurologic symptoms, DIC, and MOD were significantly different between fatal and non-fatal groups in our study.
When multivariate survival analysis was performed, only hemorrhagic manifestation and MOD were associated with a patient's death. Considering that the course of patients in the fatal group usually goes through MOD and falls into MOF, hemorrhagic manifestations could be a specific risk factor in SFTS. Previous Korean studies have focused on neurologic symptoms, not hemorrhagic manifestations, as risk factors (Choi et al, 2016, Shin et al, 2015), whereas Chinese studies have considered both hemorrhagic manifestations and neurologic symptoms as risk factors (Gai et al, 2012b, Li et al, 2018).
Therefore, the results of our study confirmed that hemorrhagic manifestation is a risk factor associated with fatality in Korean SFTS patients as in Chinese patients.
We analyzed the clinical course of SFTS using laboratory parameters dynamics of our patients. Our fatal group patients' clinical course did not match with the three clinical stages of fever, MOD, and convalescence, reported in a previous study (Gai et al, 2012b). They showed rapid changes in biomarkers around day 3 of hospitalization. All terminal patients expired within the first week, the fever stage, before reaching the MOD stage at the second week.
Even considering the delay from the onset of illness to admission, disease progression was faster and more adverse than those previously reported in Korea and China. It is speculated that the rapid clinical progression of the fatal group in this study might be characteristic of the patient group in Korea or our region. This might be due to the fact that patients in our study were older than those in the previous study on Chinese subjects. It might also be a clinical feature of Korean SFTS patients. Therefore, additional research is needed to elucidate this.
Non-fatal group patients showed abnormalities in all blood cell count parameters, including AST, ALT, and aPTT, at the first week of admission, which corresponded to the fever stage. However, they gradually recovered to normal values around day 7. Most of them were normalized in the convalescent stage, the third week. Dynamic changes of laboratory parameters showed significant differences in PT, aPTT, albumin, AST, ALT, BUN, creatinine, LDH, and CK between fatal and non-fatal groups.
However, WBC, neutrophil, lymphocyte, and platelet levels showed no significant difference between the two groups. Both PT and aPTT were significantly increased in the fatal group, corresponding to frequent hemorrhagic manifestations of the fatal group.
A previous study in China that analyzed clinical manifestation and laboratory findings of SFTS patients reported that there are three stages in the clinical progression of SFTS: fever stage, MOD stage, and convalescent stage (Gai et al, 2012b). In our study, patients in the fatal group did not undergo these three distinct stages over three weeks. All patients died within the first week of admission. Thus, we divided the first week into three periods (day 0, 1–3, and 4–7) and analyzed the dynamics of laboratory parameters (Figs. 3 and 4). Although there was no difference in parameters between fatal and non-fatal groups on day 0, the differences between the two groups were relatively clear in day 1–3.
As with results showing significant differences in important biomarkers between fatal and non-fatal groups, all biomarkers were associated with patient's death in univariate analysis. However, in multivariate analysis, no parameter examined had a significant relationship with fatality. Unlike our study, multivariate analysis in a previous study in Korea has shown that CRP and aPTT are associated with patient fatality (Choi et al, 2016).
The difference in these prognostic factors could be explained by the fact that the disease progression of patients in our study progressed very rapidly and worsened compared with that in the previous study. In other words, because every fatal group patient in our study worsened rapidly and all expired in 7 days, their laboratory parameters showed rapid fluctuations within the study period, which might be the reason for the difference between the present study and the previous study.
Our study results are the most recent study analyzing the clinical and laboratory outcomes of patients among SFTS studies conducted in Korea. The last SFTS study to identify risk factors associated with death in Korea was conducted in 2016 (Choi et al, 2016). Our study was meaningful because the latest data up to 2021 were utilized. In addition, our study included relatively sufficient data with more than 50 patients from a single institution. Also, as a single center study, our study had an advantage because we were able to analyze consistent test results by minimizing the difference in laboratory test results due to differences in different test platforms that might occur in a multicenter study (Greg Miller et al, 2011, Miller et al, 2014, Tate and Myers, 2016).
Limitations of this study are as follows. First, as this study was conducted through retrospective data collection, all patients were not tested in the same format. For this reason, some missing data and clinical variables were not checked in the same way every time. Second, according to the policy of the Korea Centers for Disease Control and Prevention, the patient's SFTSV infection was diagnosed only through an outsourced test at regional KCDC.
Since the diagnostic test was performed qualitatively, viral load could not be measured at the time of diagnosis. Third, most patients were transferred from a local medical center to our hospital, a university hospital. We depended on the patient's memory and medical records.
Conclusions
The results of this study demonstrated that Korean SFTS fatal group patients were older with a short interval from onset to admission than those in the non-fatal group. Hemorrhagic manifestations, neurologic symptoms, DIC, and MOD were observed more frequently in the fatal group than in the non-fatal group. Although it was not statistically clear that laboratory data were associated with patient's prognosis, we could observe clear differences in the data between the two groups during day 1–3 period after hospital admission.
Age, interval from onset of illness, hemorrhagic manifestations, and MOD were associated with death in patients with SFTS. Since our study is the most recent study analyzing a relatively large number of SFTS subjects, data in the present study could be used as basic data for Korean SFTS research and for developing effective diagnosis and therapy.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.