
Abstract
In June 2021, a traveler to Ashe County, North Carolina, was bitten by an Ixodes scapularis tick. The patient experienced axillary lymphadenopathy and an erythematous rash near the bite site. We confirmed Borrelia burgdorferi sensu stricto through PCR testing and DNA sequencing in the attached tick and later from mice trapped inside the cabin where the patient stayed.
Introduction
Ixodes scapularis ticks infected with Borrelia burgdorferi have been present for decades along North Carolina's Atlantic Coast (Levine et al, 2017). However, as recently as the mid-1980s, no I. scapularis were found on deer in the Piedmont or mountains (Apperson et al, 1990). In 2014, Herrin et al documented I. scapularis in southwestern Virginia, and in 2015 Lantos et al predicted expansion of this tick species into the North Carolina mountains.
The Case Patient
Human case data for the study were obtained per University of North Florida Institutional Review Board approval #468310-9. On June 9, 2021, a 79-year-old woman visiting Ashe County, North Carolina, United States, found a partially engorged tick attached to her right wrist (Fig. 1A) a few days after she arrived. She removed and photographed the tick (Fig. 1B). The next morning, she noticed a tender lymph node in her right axilla and sought medical care from her primary care provider through her patient messaging service.
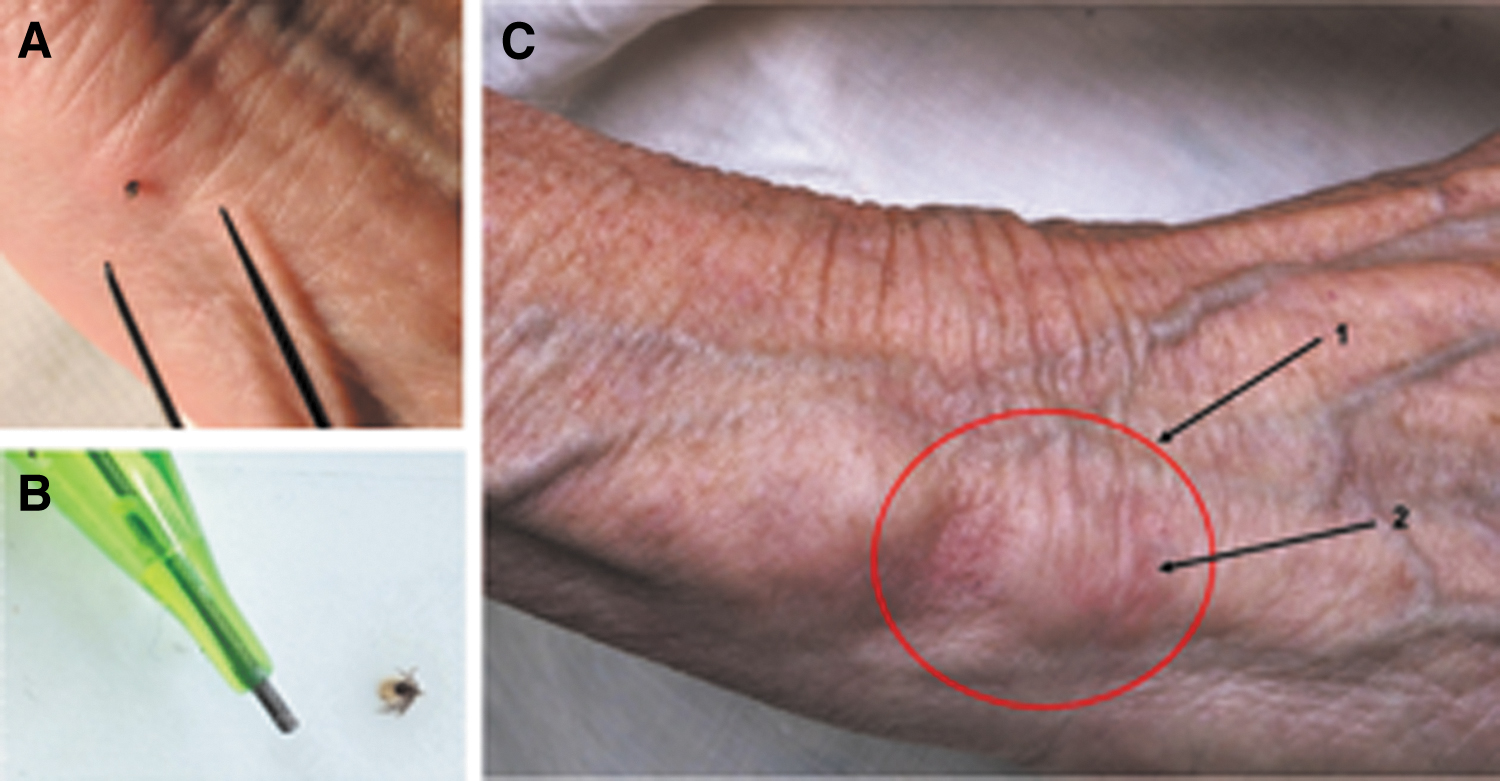
The provider offered a single-dose doxycycline prophylactic treatment, but refused additional treatment. The patient left the following day to seek further evaluation near her home 4 h away. That same morning, the patient noticed a noncontiguous area of erythema above and slightly distal to the bite site (Fig. 1C). The soonest the patient could find an urgent care center that would see her was June 12 in her Piedmont NC home county. That provider prescribed 2 weeks of 100 mg doxycycline twice a day. No blood specimens were collected for testing. The patient's rash and tender lymph node abated within a few days, and she recovered without further incident.
The tick from the patient was sent to the research laboratory of one of the authors (K.L.C.) and confirmed through standard key (Durden and Keirans, 1996) as a nymph I. scapularis. DNA was extracted from the specimen using a standard kit (EZNA Tissue Kit; Omega Biotek, Norcross, GA, USA), and tested through PCR for Borrelia species 16S-23S intergenic spacer (IGS) (Bunikis et al, 2004), Borrelia species flaB gene (Barbour et al, 1996), and B. burgdorferi ospC (Qui et al, 2002). In addition, the tick was tested for Anaplasma phagocytophilum msp2, Bartonella species 16S-23S IGS, Babesia species 18S ribosomal rRNA gene, and Rickettsia species 23S-5S ribosomal rRNA IGS, using published protocols (Casati et al, 2016; Diniz et al, 2007; Kakumanu et al, 2016; Massung and Slater, 2003).
The attached tick was positive only for Borrelia species DNA, and the common Rickettsia endosymbiont of I. scapularis (R. buchneri sequence not submitted to Genbank). The 923 nucleotide (nt) Borrelia 16S-23S IGS sequence (GenBank acc. no. OK441075) was most similar (98.9%) to several B. burgdorferi strains recovered from I. pacificus nymphs in California (e.g., GenBank acc. no. JQ308249). The 618-nt Borrelia flaB sequence (GenBank acc. no. OK513240) was 99.7% similar (2-nt mismatches) to B. burgdorferi strain N40 (GenBank acc. no. CP002228) and 99.5% similar (3-nt mismatches) to strain B31 (GenBank acc. no. CP019767).
In addition, the 530-nt B. burgdorferi sensu lato ospC sequence derived from the tick (GenBank acc. no. OK513241) was 99.1% similar (5-nt mismatches) to strain B31 (GenBank acc. no. U01894), confirming the presence of a B. burgdorferi sensu stricto strain similar to human pathogenic strains commonly found in the northeastern United States.
We made a follow-up visit in August 2022 to the location that the patient visited in 2021. We collected three host-seeking I. scapularis nymphs and 184 larvae on a cloth drag in ∼1.5 h. Because evidence of rodents was present inside the cabin where the patient had previously stayed, the cabin owner had snap traps set, and trapped four Peromyscus leucopus mice, which were provided to the authors for study. Ear tissues, along with 1 additional I. scapularis nymph and 57 larvae, were collected from the mice. DNA extracted from the ear tissues and questing nymph ticks was tested by PCR for the aforementioned pathogen groups, but using only the flaB gene PCR for Borrelia spp.
The three questing ticks were all positive for R. buchneri (sequence data not submitted to GenBank), negative for Borrelia and Bartonella, and one was positive for Babesia odocoilei (GenBank acc. no. OP684130). All mice were negative for Bartonella and Babesia species. Three of the four mice were positive for B. burgdorferi flaB gene DNA (GenBank acc. nos. OP689712–OP689714). One mouse-derived B. burgdorferi flaB sequence differed from the patient's tick-derived sequence by 1 nt, one differed by 2 nt, and one by 3 nt. In addition, one mouse tested positive for a spotted fever group Rickettsia species (GenBank acc. no. OP689711) of unknown pathogenicity.
Discussion
I. scapularis and B. burgdorferi have long been present in North Carolina's Atlantic coastal region (Levine et al, 2017), but were uncommon in the more central and western regions of the state (Apperson et al, 1990). More recent studies documented expansion of I. scapularis southwesterly along the Appalachian Mountain range (Herrin et al, 2014; Lantos et al, 2015). Hickling et al (2018) showed that I. scapularis were either established or present in several counties in eastern Tennessee along the northwest border of North Carolina.
A serological survey of B. burgdorferi antibodies in dogs suggested a lack of transmission to dogs in North Carolina before 2005 (Duncan et al, 2004). A later survey of veterinarians (Pultorak and Breitschwerdt, 2014) revealed antibody reactivity in dogs across the state, with reported reactivity statistically greater in the northern half of the state. A recent investigation of several cases of Lyme disease in Buncombe County, NC, identified four human cases associated with an outdoor camp (Barbarin et al, 2020).
The rate of B. burgdorferi infection in host-seeking nymph I. scapularis at that site was 17%, higher than that documented from questing ticks at most sites studied along the Outer Banks, for comparison (Levine et al, 2017). Together, these findings suggest that I. scapularis and B. burgdorferi have moved southward into North Carolina, and this southward expansion may not be restricted to the Appalachian corridor.
In the present case, the patient's clinical and epidemiological evidence suggest possible Lyme disease infection. Although the rash at the tick bite site did not appear as an obvious erythema migrans (EM), it is well documented that EM rashes can be highly variable and do not always occur in patients with documented Lyme disease (Rebman et al, 2021). The unequivocal molecular evidence of B. burgdorferi in the attached tick demonstrates that this patient was exposed to B. burgdorferi.
The additional evidence of several hundred ticks recovered at the site where the patient encountered the infected tick, and B. burgdorferi infection in three of four mice trapped inside the cabin where the patient stayed, strongly suggest that I. scapularis and B. burgdorferi are established at that site in Ashe County. This case did not meet the criteria of a confirmed case of Lyme disease by the North Carolina surveillance case definition (
The mountain region of western North Carolina is a popular destination for travelers. In 2019, 26% of North Carolina visitors traveled to that region of the state, totaling ∼12.7 million person-trips or ∼10.4 million overnight person-trips. Travel to the North Carolina mountains was greatest during the spring and summer (2019 North Carolina Regional Visitor Profile:
Conclusion
This report confirms B. burgdorferi sensu stricto in an I. scapularis acquired by a patient with Lyme disease-like signs and symptoms in Ashe County, North Carolina, and presents the first known DNA sequence evidence of B. burgdorferi in ticks and small mammals in Ashe County. Data obtained from the follow-up investigation 1 year later suggest that I. scapularis is established, and B. burgdorferi is endemic in natural hosts, at the site.
It is likely that risk for Lyme disease is increasing and still underrecognized in this area of North Carolina, and perhaps the entire northern portion of the state. Residents and travelers need to be aware of the risk for Lyme disease in North Carolina and take appropriate tick bite prevention measures. Furthermore, health care providers in North Carolina need to be educated on accurate diagnosis and appropriate treatment of Lyme disease.
Footnotes
Authors' Contributions
K.L.C. and M.H.-G. collected and identified ticks, drafted and edited the article, and created the figure/images. K.L.C. conducted PCR testing and DNA sequence analysis. All authors have seen, approved, and accept full responsibility for the content, and have full access to the data and analyses, as well as drafting and editing the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by donations from the Florida Lyme Disease Association and other private donors to K. Clark's UNF Foundation Research Account.