
Abstract
Background:
West Nile virus (WNV) infection is a viral disease caused by arboviruses. It can cause epidemics of febrile diseases and meningoencephalitis, especially at the end of the summer season. In this study, we aimed to determine the risk factors of WNV encephalitis with a case–control study of the patients followed in our clinic.
Materials and Methods:
Among the patients who applied to our hospital with sudden onset fever, headache, myalgia, nausea, vomiting, maculopapular rash, viral meningitis, or encephalitis findings in late summer and early autumn, those diagnosed with positive WNV PCR and antibody tests were defined as WNV cases. In the same date range, patients with clinically compatible but negative serological and PCR tests for WNV in our hospital were considered as the control group.
Results:
WNV infection was diagnosed in 26 of 48 patients who were examined with a preliminary diagnosis of WNV infection, and the other 22 patients were considered as the control group. A statistically significant difference was found between the two groups in C-reactive protein, procalcitonin, 1-h erythrocyte sedimentation rate, alkaline phosphatase, platelet, and platelet distribution width (PDW). PDW >17.85% indicated WNV infection with 82% sensitivity and 91% specificity. PDW percentage >17.85 increased the risk of WNV infection by 6.1 times. The power of the study was calculated as 83%.
Conclusion:
The most common findings in WNV cases were fever and confusion. WNV infection should be considered in the differential diagnosis in patients with fever and confusion in September and October in settlements on the migration route of birds. The percentage of PDW in whole blood examination can guide the differential diagnosis of WNV cases.
Introduction
West Nile virus (WNV) Flaviviridae is an enveloped polarized single-stranded RNA virus. WNV was first detected in Uganda in 1937. Although the first epidemic in Europe was reported in France in 1962, the first in Turkey was reported in 2010. The most common primary vector of WNV is Culex-type mosquitoes. The agent's main reservoir is birds and has an enzootic transmission cycle. Horses and humans are accidental hosts and do not matter in this cycle (Gould and Solomon, 2008). Other than mosquitoes, they can be transmitted from person to person by blood and organ transplantation (Blitvich, 2008; Hayes and O'Leary, 2004).
WNV causes epidemics with late summer febrile diseases and meningoencephalitis, especially in lakes and similar rural areas where mosquitoes are shared and on the route of migratory birds. The symptoms of infected individuals can range from mild flu-like symptoms to more serious symptoms such as encephalitis (Blitvich, 2008; Gould and Solomon, 2008).
After exposure to WNV, patients may have symptoms such as fever, weakness, headache, malaise, low-back pain, loss of appetite, diarrhea, rash, and clinically severe findings with neurological involvement such as encephalitis, meningitis, and flaccid paralysis (Hayes et al., 2005; Sambri et al., 2013) (Fig. 1).
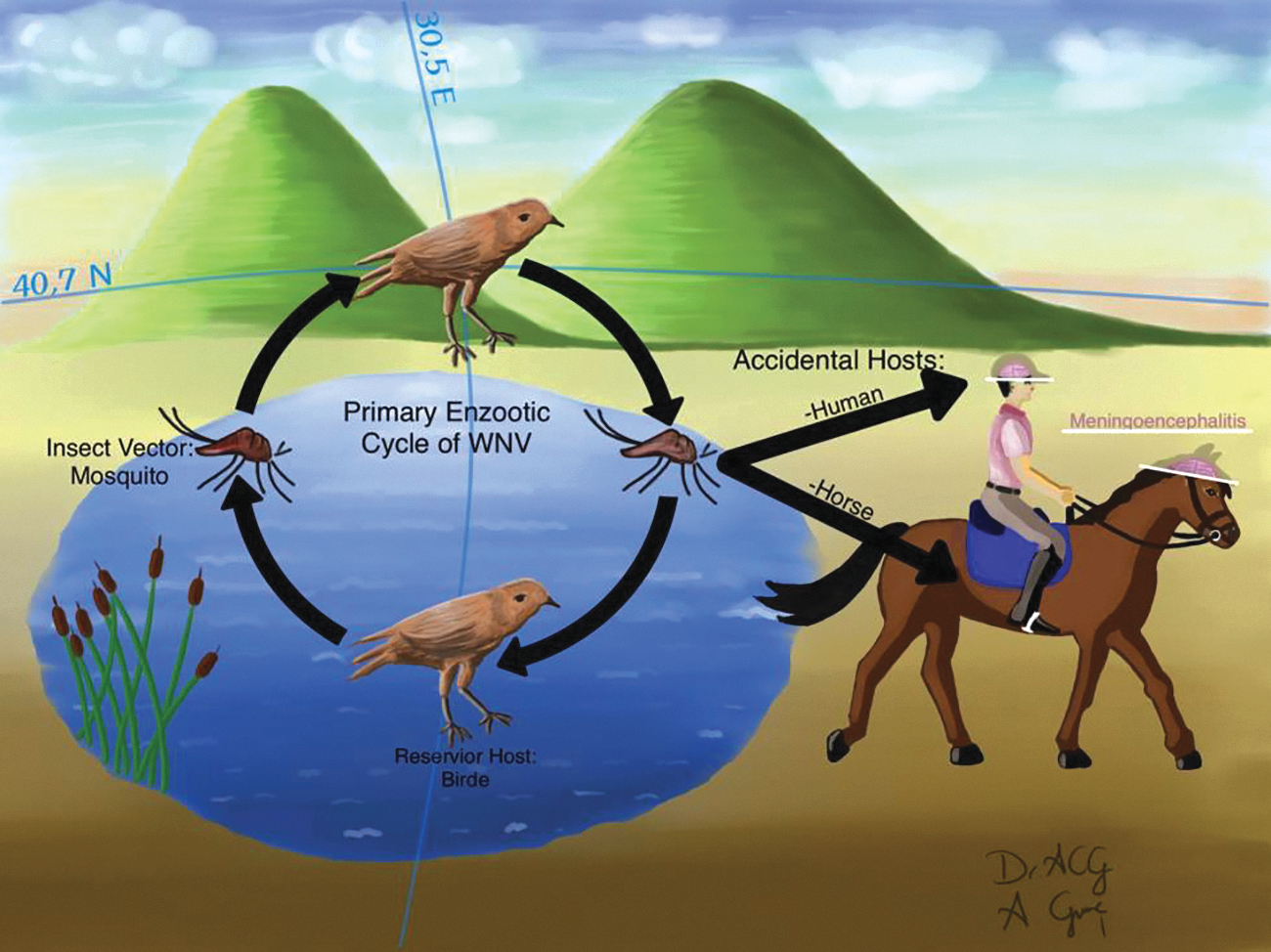
Interhost transmission routes of WNV infection. The demonstration of the transit route of migratory birds, geographical location, rural area, and lake surroundings, which are convenient features where WNV infection turns into an epidemic. WNV, West Nile virus.
The parameters of an individual with WNV infection can vary depending on the severity of their symptoms and the progression of the infection. Cases infected with WNV are often asymptomatic. For this reason, many infections cannot be identified at all. However, many countries are endemic to WNV according to their geographical location (Kalaycioglu et al., 2012). Therefore, determining the clinical features of the cases in which we detected WNV and compiling the information we obtained from these cases is essential for detecting future WNV outbreaks.
The gold standard in the diagnosis of WNV infection is virus isolation. However, serology is used more in practice for diagnosis, since its efficiency is low in humans (Sambri et al., 2013). Serological diagnostic methods are less standard than complete blood counts and more costly. Therefore, access to serological tests is more limited than a complete blood count. Platelet distribution width (PDW) is part of the complete blood count. PDW is the variation in platelet size, and the PDW value may change in conditions such as infection and inflammation (Artunc Ulkumen et al., 2014).
WNV infection can cause a significant change in blood cells. The severity of the infection can vary depending on the degree of changes. In general, the following hematological changes can be observed in individuals with WNV infection: White blood cell count: Some individuals may experience a decrease in white blood cell count after being infected, whereas others may experience an increase. However, these changes can vary depending on the severity of the infection. Lymphocyte count: Lymphocytes (immune cells) can also be affected. Some infected individuals may experience an increase in lymphocyte count, whereas others may experience a decrease. Platelet count: Individuals with WNV infection may experience decreased platelet count. This can vary depending on the severity of the infection. Red blood cells: Some infected individuals may experience a decrease in red blood cell count. However, these changes can vary depending on the severity of the infection. Hemoglobin: Hemoglobin levels can also vary in individuals with WNV infection. Depending on the severity of the infection, hemoglobin levels may increase or decrease. These changes can vary depending on the course of the infection and the individual's immune system response.
In this study, we aimed to compile the characteristics of patients infected with WNV in the summer of 2018 using the case–control method and to show that PDW value can be a new marker in differentiating WNV infection.
Materials and Methods
Definition
Sakarya Province is in the Eastern Marmara Region of Turkey, with ∼1 million living in agriculture and industry. There are lakes such as Sapanca and Poyrazlar Lake in the province, and they are on the migration path of many migratory birds. Many WNV infections have been reported in Sakarya Province since 2010 (Kalaycioglu et al., 2012).
Facts
Antigen, antibody, and PCR tests were positive for WNV patients who applied to our hospital with sudden onset fever, weakness, headache, myalgia, nausea, vomiting, maculopapular rash, viral meningitis, or encephalitis findings in September and October 2018. Demographic characteristics of the patients were obtained from patient files and face-to-face conversations.
Obtaining demographic data
All data were obtained from the hospitalization file after the seropositivity of the patients was confirmed. Missing data that could not be obtained from the patient files were completed when the patients came for control.
Control group
For the control group, age- and gender-matched patients with similar symptoms but with negative WNV IgM (Enzyme-Linked ImmunoSorbent Assay [ELISA]) and PCR tests were selected.
Tests
ELISA method was used at Ankara Public Health Institution to detect the presence of WNV PCR, WNV IgG and IgM antibodies. Cases with positive WNV PCR and WNV IgM were defined as WNV cases.
Case definition
Patients presenting with symptoms of meningitis, encephalitis, and meningoencephalitis of unknown origin, as well as those exhibiting at least one clinical sign of meningitis (such as abrupt mood changes, acute central and peripheral neurological dysfunction, nuchal rigidity, acute muscle weakness, or neuropathies like cranial and peripheral neuritis), were classified as ‘suspected cases’. To confirm the presence of WNV, a specific IgM and IgG antibody search was conducted using either the ELISA or the Immunofluorescence Assay (IFA) method. Patients in whom both ELISA and IFA methods revealed the presence of WNV-specific antibody responses in their serum samples were categorized as ‘probable cases’.
Statistical analysis
Descriptive analyses were made for the information related to the general characteristics of the population constituting our study. The data are visualized. Data visualization techniques, histogram plots, Shapiro–Wilk, and Kolmogorov–Smirnov were used to examine the distribution characteristics of the data. Mann–Whitney U test was used to compare nonparametric numerical data. Nonparametric data are given as median values (25–75% percentiles). Chi-squared tests were used to compare categorical data. Categorical data are given as numbers (% percent).
To evaluate the performance of the PDW value, the area under the curve (AUC) was calculated with receiver operating characteristic (ROC) curve analysis. The value with the highest sensitivity and specificity was accepted as the cutoff value. Odds ratio risk analysis was performed with the data below and above the cutoff value. p-Values <0.05 were considered statistically significant. IBM SPSS package program was used in the analysis of the data.
The Sakarya University Faculty of Medicine Ethics Committee applied for this study. It was approved with decision number 71522473/050.01.04/23 and accepted to comply with the ethical rules.
Results
A total 26 patients who applied to our hospital in September and October 2018 and were examined with the preliminary diagnosis of WNV infection and found positive for WNV PCR and IgM (ELISA) were considered to be infected with WNV, whereas 22 negative patients were accepted as the control group. The median age of the group with WNV infection was 58 (39–73) years, and the control group was 52 years (40–63), and there was no statistically significant difference between the two groups (p = 0.487).
The results obtained from the patients and the control group are presented in Tables 1 and 2. The most common findings in WNV cases were fever and confusion. Although 7 out of 26 patients were followed up, 19 were hospitalized. Six of the 19 hospitalized patients required hospitalization in the intensive care unit. Four out of six patients treated in the intensive care unit resulted in mortality. Sixteen patients were followed up with the clinic for WNV encephalitis. Nine of 19 hospitalized patients had a history of hypertension.
General Demographic Characteristics of West Nile Virus -Positive Cases
WNV, West Nile virus.
Comparison of Blood Tests of Groups with Positive and Negative West Nile Virus Infection (Control Group)
Variables are expressed as median values (25–75 percentiles).
Statistically significant (p < 0.05).
Four patients did not have a history of hypertension while hospitalized, whose systolic blood pressure exceeded 150 mm/Hg and diastolic blood pressure was above 90 mm/Hg. In one of them, due to resistant hypertension, glyceryl trinitrate infusion was administered intravenously. Whereas maculopapular rash was seen in six patients, pneumonia in two patients, facial paralysis in one patient, Guillain–Barré syndrome in one patient, and one patient was 38 weeks pregnant. C-reactive protein (CRP), erythrocyte sedimentation rate, and platelet values were significantly lower in WNV-infected patients compared with the control group.
The median PDW value was 18% (17.8–18.8) in the group with WNV infection and 17.10% (16.7–18.4) in the control group (p = 0.001, Fig. 2). The cutoff value of PDW in determining WNV infection was 17.85% (AUC: 0.901 [95% confidence interval 0.781–1], sensitivity: 82%, specificity: 91%, p < 0.001, Fig. 3). Odds ratio was 6.107 (95% confidence interval 1.8–20.3) when the PDW value was 17.85% and above. When the cutoff value of PDW was accepted as 17.85%, post hoc analysis was performed to determine its power in detecting WNV infection. The power of this study was found to be 83%.

Boxplot of PDW value in two groups with negative and positive WNV infection. PDW, platelet distribution width.

ROC curve evaluating the performance of PDW in detecting WNV infection. ROC, receiver operating characteristic.
Discussion
According to the results we obtained in this study, a parameter that could distinguish between the clinical and laboratory characteristics of the cases in the study control groups, indicating WNV infection, was obtained. WNV infection can be easily overlooked if there is a need for epidemiological information. Especially October is the month when WNV peaks the most. Therefore, if there is unexplained weakness, fever, encephalitis clinic, or thrombocytopenia in October, WNV should be considered, and tests should be performed.
Of the patients with positive WNV in this study, 19 (73%) were hospitalized, and 6 were followed up in the intensive care unit. This situation suggested that the disease progressed with severe clinical findings. Similar findings are also seen in the data of the 2010 epidemic in our country. All the cases included in that study had to be hospitalized (Kalaycioglu et al., 2012).
Four (15%) of 26 cases with positive WNV in our study resulted in mortality. In the study that compiled the WNV cases in our country in 2010, 10 (21%) of 47 cases died. The age of the patients who died was 25–86 years, and the mean age was 76 years. Four fatal cases lived in rural areas, and six had comorbid diseases such as diabetes mellitus, hypertension, chronic obstructive pulmonary disease, and psychiatric diseases (Kalaycioglu et al., 2012).
Greece experienced a significant outbreak of WNV infection in 2010 and 2017. Between July and September 2017, 45 confirmed or probable cases of WNV infection were identified in this outbreak. Advanced age, hypertension, and diabetes mellitus were identified as risk factors in this epidemic. The majority of patients with neuroinvasive involvement were older than 70 years of age (Mavrouli et al., 2019). In our study, the patient with unilateral facial paralysis was 69 years old and is compatible with the literature.
Median platelet count in patients in the WNV-positive group, 200 (167–226) U/F, was higher in the control group (p = 0.025). In addition to their role in coagulation, platelets are now considered the primary inflammatory cells with essential roles in the innate and adaptive arms of the immune system. Low platelet counts seen in patients with sepsis are defined as a marker for poor prognosis. Viral infections often coincide with platelet activation. Inflammatory responses of the host result in the secretion of platelet-activating mediators and the emergence of a prooxidative and anticoagulant environment that promotes platelet activation.
More importantly, viruses directly interact with platelets and megakaryocytes and disrupt the functions of platelets. In addition, platelets can be activated by viral antigen–antibody complexes, and in response to some viruses, B lymphocytes also produce antiplatelet antibodies, targeting them. All these processes that contribute to platelet activation result in increased platelet consumption and removal of platelets. It, therefore, leads to thrombocytopenia, which is often observed during viral infection (Assinger, 2014). In this study, the significant decrease in platelet count compared with the control group suggested that it was related to the immune response to viral infections.
In a study of COVID-19 patients, the average PDW percentage of those with severe disease was 16.47, whereas the average of those with mild disease was 17.11 (Ravindra et al., 2022). In a study conducted on patients with Crimean–Congo bleeding with fever, the PDW value was 17.6% ± 0.8 in the group with hemorrhage and 17% ± 0.7 in the group without hemorrhage. In ROC analysis, AUC was 0.67, sensitivity 68%, and specificity 65%. In the regression analysis, each unit increase in PDW increased the probability of bleeding 3.5 times.
PDW value successfully determined the severity of the disease in Crimean–Congo hemorrhagic fever (Yilmaz et al., 2016). In our study, the cutoff value of PDW in determining WNV infection was 17.85%, AUC 0.901, sensitivity 82%, and specificity 91%. A PDW value >17.85 increased the probability of diagnosing WNV infection 6.1 times in patients with similar clinical presentations.
According to our literature review, the predictive analyses of PDW value for WNV infection have yet to be studied, and, therefore, our study is the first in the literature.
Limitations of the research
The study's limitations are that it is retrospective, a rare disease, diagnostic tests are not easily performed in every center, and the number of cases could be higher.
Conclusion
As a result, CRP value, erythrocyte sedimentation rate, and platelet count were significantly lower in WNV cases than in the control group, whereas PDW was higher. The most common findings in WNV cases were fever and confusion. Countries with migratory birds' routes have suitable geographical conditions for WNV. WNV infection should be considered in the differential diagnosis, especially in cases with fever and confusion in September and October. PDW may be helpful in the differential diagnosis of WNV.
Footnotes
Acknowledgments
We thank the Sakarya Training and Research Hospital and the Infection Control Committee for their support in this research.
Ethical Approval
An ethics committee approval from Sakarya University Medical Faculty was provided for this study (Data: 16.09.2019, Protocol No: E-71522473/050.01.04/23).
Informed Consent
No written informed consent was necessary for this type of study.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.