
Abstract
Background:
Tularemia is one of the most prevalent zoonoses across the world. Patients in Turkiye mostly contract the oropharyngeal form, acquired through drinking, or contact with microorganism-contaminated water.
Methods:
Patients with oropharyngeal tularemia aged under 18 years and diagnosed between January 01, 2017, and December 31, 2020, were evaluated retrospectively. Tularemia was diagnosed in patients with compatible histories, symptoms, clinical presentations, and laboratory test results.
Results:
The mean age of 38 children was 12.1 ± 3.4 years, and the female/male ratio was 0.58 (14/24). The mean duration of symptoms on admission was 33.8 ± 26.2 days. All children had enlarged lymph nodes. Malaise, fever, and loss of appetite were other frequent symptoms. Patients were treated with antibiotics for a mean of 26.2 ± 18.8 days. Gentamycin was the most frequently used antibiotic (either alone or in combination) (n = 29, 76.3%). Twenty-six (68.4%) patients underwent surgical procedures in addition to antibiotherapy. Five (13.2%) required secondary total excision. Patients with higher leukocyte counts at admission received a combination of antibiotherapy plus surgery, rather than antibiotics alone. No relapses, reretreatment requirement, or mortality were observed after 12 months of follow-up.
Conclusions:
Oropharyngeal tularemia in children can require longer courses of antibiotic treatment with more than one drug and more frequent surgery than previously suggested in the literature, especially if the patients are admitted late to the hospital, symptom duration is prolonged, and appropriate treatment is initiated late. Higher leukocyte counts on admission may be prognostic for longer antibiotic treatment course and suppurative complications that require surgery. Raising awareness among patients and physicians is essential.
Introduction
Tularemia, also known as hunters’ disease, rabbit fever, deerfly fever, O’Hara’s disease, and Francis’ disease, is an ancient, ubiquitous zoonotic disease. Following a period of scarcity, re-emergence has been reported in many Middle Eastern countries, such as Turkiye and Iran. Various factors, including armed conflicts, climatic variations, and natural calamities, which generate a cycle between humans and vectors or rodents, have been implicated (Shahsavari et al., 2018).
It is endemic in the northern hemisphere countries such as the Russian Federation, Kazakhstan, Turkmenistan, Finland, and Sweden (World Health Organization, 2007). The reported prevalence in Turkiye is up to 2.88/100,000 in recent years (Turkish Ministry of Health, 2023). Numerous water-borne outbreaks and nonoutbreak oropharyngeal tularemia cases have been reported to date (Hennebique et al., 2019). Humans contract the disease through ingestion of contaminated food or water, tick/deer fly bites, skin contact with infected animals, inhaling contaminated aerosols/dust, and laboratory exposure. Drinking or contact with microorganism-contaminated water during aquatic activities such as swimming and fishing is a major mode of transmission, which causes oropharyngeal tularemia to be the most common of the six major clinical forms in Turkiye (Kwit et al., 2019).
History, symptoms, and findings suggestive of tularemia, plus unresponsiveness to classical beta-lactam antibiotics, traditionally suggest a diagnosis of oropharyngeal tularemia. A limited number of antibiotics effective against intracellular infections and with well-established efficacy, such as streptomycin, gentamicin, tetracyclines, fluoroquinolones, and chloramphenicol, are available. Unfortunately, however, there is a scarcity of controlled clinical studies evaluating the efficacy of different drug regimens or the optimal duration of tularemia treatment. Antibiotic therapy consists of one or more of these agents to inhibit the growth and/or virulence of Francisella tularensis. Although no resistance to aminoglycosides, fluoroquinolones, or tetracyclines has been reported in clinical isolates, the disease is difficult to manage, especially when diagnosis is delayed.
The objective of this study was to evaluate children with oropharyngeal tularemia in terms of their epidemiological characteristics, management details, and clinical responses, and to determine predictors for complications.
Materials and Methods
Patients with oropharyngeal tularemia aged under 18 years and diagnosed between January 01, 2017, and December 31, 2020, in Erzurum Regional Training and Research Hospital were evaluated retrospectively. The data were extracted from the patients’ files, and missing data were completed by phone calls with the families.
Tularemia was diagnosed in patients with compatible histories, symptoms, clinical presentations, and laboratory test results. Patients with other forms of tularemia and individuals with clinical or laboratory evidence of any other disease capable of mimicking tularemia, such as leukemia, solid tumors, and viral infections, were excluded. Laboratory diagnosis of tularemia was based on positive Tularemia tube agglutination test results (titer ≥ 1:160). Patients with the other forms (typhoidal, ulceroglandular, glandular, oculoglandular, and pneumonic) of tularemia were not included.
Patient data involving demographic variables, including risk factors for transmission of the pathogen (contact with livestock, chlorination of water source, nature activities, etc.), symptoms (enlargement of lymph nodes, fever, malaise, etc.), physical examination findings (lymphadenopathy, fever, etc.), and laboratory results (tularemia serology, leukocyte, and hemoglobin values, etc.) were recorded. Treatment details, including the type of antibiotics and duration of treatment, and surgery type and requirements were also noted. The patients who were given antibiotics alone were compared with those who received antibiotics plus surgical treatment. Afterward, correlation analyses were performed to reveal the associations between treatment durations and other patient characteristics.
The legal guardians of all children gave informed consent for their inclusion in the study. The study was approved by the local institutional ethics committee (Erzurum BEAH 2022/18-179).
Data were analyzed on SPSS (Statistical Package for the Social Sciences) version 17.0 software. The Shapiro-Wilk test was used to investigate whether the continuous variables were normally distributed. Mean, standard deviation, median, minimum, and maximum values were used for descriptive statistical data. The significance of differences between the mean values of two groups was measured using the t-test, while the significance of differences between the median values of two groups were measured using the Mann-Whitney U test. The χ2 or Fischer’s exact tests were used to compare categorical variables. Spearman correlation analysis was applied to measure the strength of relationships between continuous variables. Statistical significance was set at 0.05.
Results
There were five patients with glandular and 38 patients with oropharyngeal tularemia during the study period. The mean age of the patients with oropharyngeal tularemia was 12.1 ± 3.4 years. The female/male ratio was 0.58 (14/24). Only five (13.1%) patients were below eight years of age. Many of the patients (n = 29, 76.3%) were living in Erzurum, and 35 (92.1%) were living in rural areas. Patients were most frequently admitted in September (n = 11, 28.9%) (Fig. 1), and the majority had histories of contact with livestock (n = 30, 78.9%) (Table 1). Generally, the children’s caregivers either denied knowing or did not know the chlorination status of their water sources (n = 29, 76.3%). None of the children had histories of tick bites or travel.
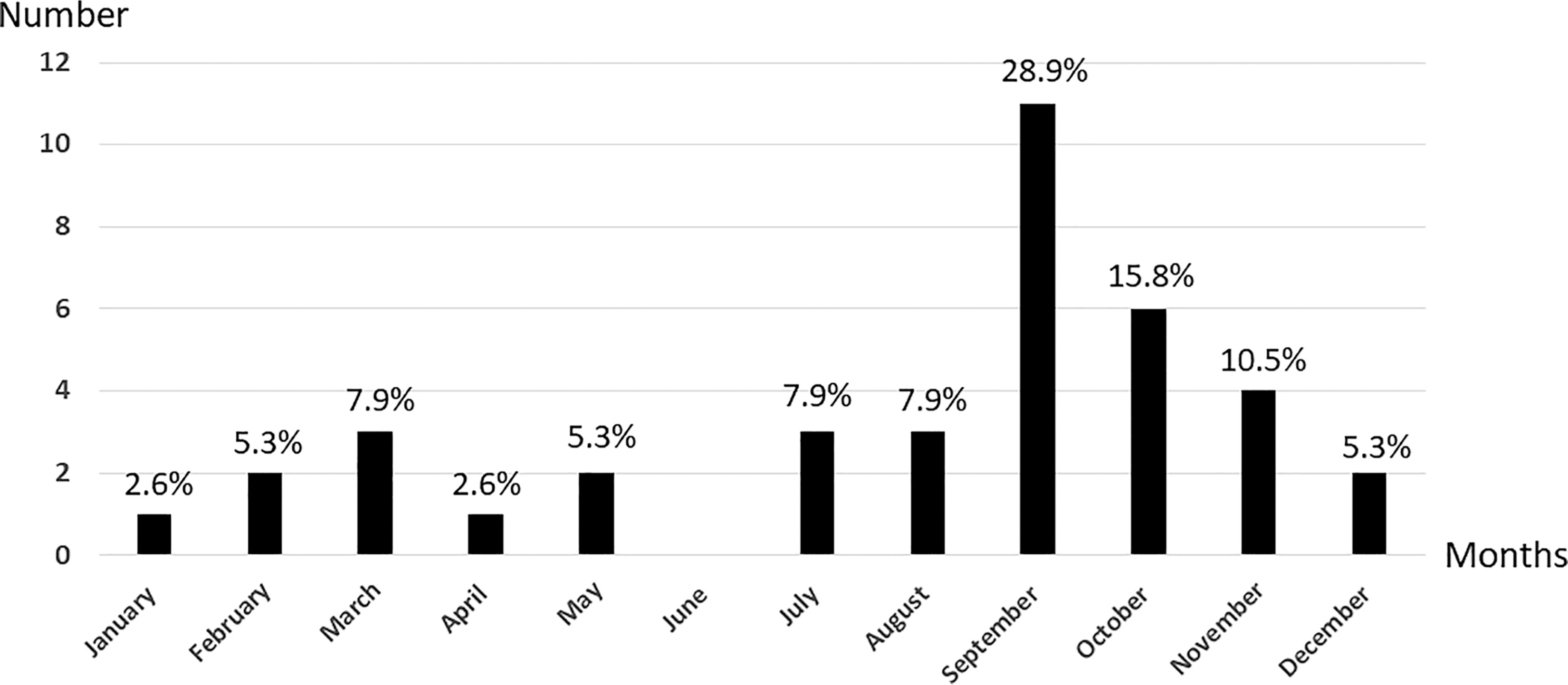
Distribution of patients’ admission times.
The Patients’ Risk Factors, Symptoms, and Clinical Findings, n (%)
The water supply of 26 (68.4%) patients had no chlorination, while 3 (7.8%) patients did not know the water chlorination status.
The children’s symptoms persisted for a mean of 33.8 ± 26.2 days on admission. All had enlarged lymph nodes. Malaise (n = 26, 68.4%), fever (n = 23, 60.5%), and loss of appetite (n = 23, 60.5%) were other frequent accompanying symptoms. Lymphadenopathy was solitary in nearly half of the patients, and 47.3% of the participants had tonsillopharyngitis (Table 1). The oropharyngeal form of tularemia was diagnosed in all cases, and 27 (71.1%) of the patients were hospitalized. Only one (2.6%) patient had elevated transaminases, and no patient exhibited renal function abnormality. Other laboratory parameters are shown in Table 2.
Patients’ Laboratory Findings and Treatment Data
SD, standard deviation; min, minimum; max, maximum.
None of the patients had previously received an antibiotic known to be effective against F. tularensis. Gentamycin (5 mg/kg/day), streptomycin (30 mg/kg/day), doxycycline (4 mg/kg/day), or ciprofloxacin (30 mg/kg/day) were given as antibiotics. The mean total length of antibiotic therapy during the study period was 26.2 ± 18.8 days. Gentamycin was the most frequently used antibiotic (either alone or in combination) (n = 29, 76.3%). The median duration of gentamycin therapy was 14 (7–28) days, while doxycycline and ciprofloxacin had the longest duration of use (21 [7–70] and 21 [14–68] days, respectively) (Table 2). Patients unresponsive to antibiotherapy (emerging hyperemia, fluctuation, or lymph node enlargement) underwent surgical procedures performed by otorhinolaryngology surgeons. Twelve (31.6%) patients were treated only with antibiotics, while the remainder (n = 26, 68.4%) underwent surgical procedures in addition to antibiotics. Drainage of the abscess alone was performed in more than half of those cases due to the proximity of lymph nodes to the vital structures (n = 22, 57.9%). The mean time to surgery is 6.9 ± 2.9 (min-max, 2–13) days of antibiotic treatment. Among the patients who underwent lymph node drainage at first and persistent pathological lymphadenopathy at least 3–4 weeks after the postoperative changes, which include tissue edema, redness, etc. in the surgical area, five (13.2%) of them underwent secondary total excision. Histopathological examination of all the surgical specimens revealed necrotizing granulomatous lymphadenitis.
The comparison analysis between the patients who were given antibiotics alone and those who received antibiotics plus surgical treatment yielded no statistically significant results. However, it was seen that patients with higher leukocyte counts received combined antibiotherapy plus surgery rather than antibiotics alone (11,022 ± 3,354 vs. 9,223 ± 2,789). Correlation analyses revealed that durations of treatment with gentamycin and ciprofloxacin were positively correlated with total leukocyte and neutrophil counts (Table 3). In addition, the length of doxycycline therapy was positively correlated with the duration of symptoms.
Correlation Analyses Between Duration of Antibiotherapy and Other Study Parameters
All patients were followed up for 12 months, and none of them experienced relapses, or mortality, or required retreatment. Four (23.5%) patients experienced gastrointestinal intolerance with doxycycline, which was relieved by behavioral modifications and antacids.
Discussion
The prevalence of tularemia has exhibited a substantial rising trend in recent decades, due to heightened awareness of the disease, greater sensitivity in diagnostics, and increased bacterial colonization of ticks and rodents (Imbimbo et al., 2020). Bibliometric analysis also shows that it has attracted growing attention in recent years (Kaya and Üçer, 2022). Among the six clinical forms, the oropharyngeal form accounts for the greatest proportion of cases in Turkiye. Children diagnosed with oropharyngeal tularemia are presented in this study.
None of the patients in this study had previously received an antibiotic covering F. tularensis. In addition, the time elapsed until hospital admission was longer than that in previous studies (Schöbi et al., 2022; Sadiku et al., 2022). This can be attributed to the lower sociocultural and socioeconomic levels of our study population, which resulted in delayed access to healthcare services. Rotem et al. (2012) investigated the efficacy, bacterial load, and humoral response after delayed treatments with ciprofloxacin or doxycycline in mice with tularemia. Delayed onset of both antibiotics resulted in exacerbation of the disease symptoms, although all animals survived after prolongation of treatment. Önen et al. (2012) reported similar times for delayed hospital admission, which they concluded that it resulted in the suppuration of lymph nodes. Tezer et al. (2015) showed that a treatment delay ≥16 days was associated with therapeutic failure. Especially in endemic areas, the awareness of both patients and physicians about tularemia should be increased. To minimize exposure, prevention measures, such as avoiding contact with sick/death animals, drinking unsafe waters, eating wild animal meats, and using repellents effective against ticks, etc. should be advised. Education of patients and their parents to promote early hospital admission can also provide advantage for treatment.
Prognosis is usually poor in patients with tularemia in the event of delayed treatment or immunocompromised status (Maurin 2015). Studies have revealed that elevated leukocyte counts and an increase in inflammatory markers are frequently seen in children with tularemia (Tezer et al., 2015). Most of the patients in this study were treated with more than one antibiotic during their course of treatment, which is important to illustrate one of the difficulties encountered in the management of oropharyngeal tularemia. In the present study, patients with higher leukocyte counts received a combination of antibiotic and surgical therapies, rather than antibiotics alone. The higher the total leukocyte and neutrophil counts, the longer the duration of gentamycin and ciprofloxacin therapies. It was concluded that higher leukocyte counts on admission may be predictive of both complications and a longer duration of antibiotic therapy, and thus a poor prognosis.
Ten days, or even as little as 5–7 days, of effective antibiotic therapy are generally recommended for children with mild disease and no complications (American Academy of Pediatrics, 2021). Nevertheless, the mean antibiotic treatment in our study was 26.2 (max: 70) days, which is much longer than the recommended duration. It can be concluded that in selected cases, especially if symptom duration is long and the probability of complications is high, the antibiotic treatment period can be longer, even more than 3 weeks. In addition, there is a lack in the current literature of well-designed comparative data concerning the efficacy of different antibiotic options, combinations thereof, and optimal durations of use. Aminoglycosides seem to exhibit an adequate bactericidal effect and low relapse rates and are therefore the most frequently employed agents (Penn, 2023). Similarly, gentamycin was the most frequently administered antibiotic in our study. However, doxycycline and ciprofloxacin exhibited the longest duration of antibiotic use. In an animal study, doxycycline was shown to be effective only if initiated within a short time window (Rotem et al., 2012). Due to its bacteriostatic nature and potential for disease relapses, a minimum duration of 14–21 days is recommended (Tezer et al., 2015). In case of osteoarticular involvement, it was used for as long as 12 months (Ponderand et al., 2023). Ciprofloxacin has been shown to be effective against highly virulent strains at later stages of the disease (Rotem et al., 2012). Weber et al. (2012) proposed that oral fluoroquinolones might represent a promising option, with most patients treated with ciprofloxacin for more than 10 days recovering uneventfully, without the addition of aminoglycosides or tetracyclines. However, the patients in that study were admitted to the hospital after a median of 3 days of illness (range 0–44 days), and the median time elapsing between the onset of symptoms and administration of an effective antibiotic was only 13 days. With these results, it is not so easy to present a recommendation to choose which of these antibiotics to lower the mean length of antibiotic use and surgical intervention rate.
More than two-thirds of the patients in this study required surgical intervention in addition to antibiotic therapy. Combining surgical drainage with antibiotic therapy is known to increase the success of treatment in patients with oropharyngeal tularemia (Gozel et al., 2014). However, our surgery requirement rate was higher than those reported by the other pediatric tularemia studies (Tezer et al., 2015; Schöbi et al., 2022; Sadiku et al., 2022; Oz et al., 2014). In addition, 13.2% of our study population required secondary surgical intervention since total excision could not be performed initially because of the proximity of the lymph nodes to the vital structures. Tezer et al. (2015) reported similar rates for secondary surgical procedure requirements, irrespective of the type of antibiotic therapy. This may be attributable to delayed admission and a lack of compatible antibiotic therapy before admission. In addition, the rate of reoperation indicates the importance of selecting of most appropriate form of surgery. It may be speculated that primary total excision can lower reoperation and complication rates and reduce the length of antibiotic therapy.
Most of the children in this study were aged over eight, and their mean age was 12.1 ± 3.4 years, higher than in previous pediatric studies (Tezer et al., 2015; Schöbi et al., 2022; Sadiku et al., 2022; Oz et al., 2014). Children particularly contract the disease while engaging in outdoor activities. Most of our patients were living in rural areas and had a history of contact with livestock. The city where this study was performed has a cold climate with an average annual temperature of approximately 5°C, which probably protected younger children against contact with farm animals, rodents, or rodent excreta, or drinking natural spring water. Oropharyngeal tularemia is the most common form in Turkiye and exhibits a seasonal pattern. The disease is especially prevalent during the cold and rainy seasons, as shown in this and previous similar studies (Tezer et al., 2015; Kaya et al., 2012).
Fever was one of the most frequent symptoms in our patients, similarly to the previously cited oropharyngeal tularemia study performed in our city (Özden et al., 2018). Malaise and loss of appetite are frequently reported in children diagnosed with tularemia, also in agreement with the present study (Schöbi et al., 2022; Sadiku et al., 2022; Kaya et al., 2012). Tularemia is thought to be underdiagnosed. However, the disease should be considered in endemic regions when children develop constitutional symptoms, lymphadenopathy, or any combination of other signs and symptoms corresponding to the different forms of tularemia.
Various limitations should be considered when interpreting the results of this study. The research was retrospective in nature and involved a small population, meaning that the durations and individual success rates of the different antibiotic therapies cannot be compared. In addition, the causative agent was unable to be grown in cultures, and neither antibiogram nor subtype analysis were therefore possible. Nevertheless, the literature concerning pediatric oropharyngeal tularemia contains few prognostic clues. This study is important because it shows that cases with oropharyngeal tularemia can require longer courses of antibiotic treatment with more than one drug and more frequent surgery than previously suggested in the literature. Additionally, higher leukocyte counts on admission can predict suppurative complications and longer durations of antibiotic therapy.
In conclusion, constitutional symptoms and prolonged lymphadenopathy unresponsive to standard antibiotics should raise suspicion of oropharyngeal tularemia, especially in endemic regions. Oropharyngeal tularemia in children can require longer courses of antibiotic treatment with more than one drug and more frequent surgery than previously suggested in the literature, especially if the patients are admitted late to the hospital, symptom duration is prolonged, and appropriate treatment is initiated late. Higher leukocyte counts on admission may be prognostic for a longer antibiotic treatment course and suppurative complications requiring surgery. Raising awareness among patients and physicians is essential to take preventive measures, promote early admission when symptoms develop, the use of effective antibiotics, and appropriate surgical intervention, if necessary, particularly in endemic areas where knowledge about tularemia can be limited.
Footnotes
Authors’ Contributions
S.S.K.: Conceptualization, data duration, design of methodology, formal analysis, visualization, writing—original draft, and writing—reviewing and editing. M.P.: Conceptualization, writing—original draft, and writing—reviewing and editing. E.H.E.: Data curation, writing—original draft, and writing—reviewing and editing. A.S.D.: Conceptualization, data curation, design of methodology, formal analysis, visualization, writing—original draft, and writing—reviewing and editing.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
There is no funding to declare.