
Abstract
Background:
The burden of zoonotic diseases in developing countries is significantly underestimated, influenced by various factors such as misdiagnosis, underreporting, natural disasters, climate change, resource limitations, rapid unplanned urbanization, poverty, animal migration, travel, ecotourism, and the tropical environmental conditions prevalent in the region. Despite Sri Lanka's provision of a publicly funded free health care system, zoonoses still contribute significantly to the burden of communicable diseases in the country. This study serves as a timely and exhaustive systematic review of zoonoses reported over the past 22 years in Sri Lanka.
Materials and Methods:
This systematic review adhered to the guidelines provided by the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) statement. A systematic literature search was conducted between July and September 2022, utilizing the following databases and sources: Google Scholar, PubMed, Cochrane Library, Weekly Epidemiological Reports, and Rabies Statistical Bulletins published by the Ministry of Health, Sri Lanka.
Results:
From the initial database search, 1,710 articles were identified. After excluding nonzoonotic diseases, duplicated reports, inaccessible articles, and those not meeting the inclusion criteria, 570 reports were evaluated for eligibility. Of these, 91 reports were selected for data extraction, comprising 58 original research articles, 10 case reports, 16 weekly epidemiological reports, and 7 rabies statistical bulletins. Over the study period (2000–2022), 14 parasitic, 7 bacterial, and 7 viral zoonoses have been reported in Sri Lanka. Notably, leptospirosis emerged as the most reported zoonotic disease in the country.
Conclusions:
In response to these findings, we strongly recommend the implementation of a tailored, country-specific prevention and control program. To achieve this goal effectively, we emphasize the importance of adopting a country-specific “One Health” approach as a comprehensive framework for managing and controlling zoonotic diseases in Sri Lanka.
Introduction
Infectious diseases that can naturally transmit from vertebrate animals to humans are called zoonotic diseases (WHO, 2020). It has been documented that a significant portion of emerging infectious diseases, specifically 60.3%, is attributable to zoonotic pathogens, with approximately 71.8% originating in wildlife (Jones et al., 2008). These zoonotic pathogens encompass various types, including bacteria, viruses, parasites, fungi, rickettsia, chlamydia, mycoplasma, and acellular nonviral agents (Rahman et al., 2020). The routes of transmission of zoonotic diseases to humans often occur at the interface between human populations and wildlife due to livelihood activities, the need for sustenance, and cultural practices (Namusisi et al., 2021). In addition, domesticated animals can serve as conduits, bridging the gap between humans and wildlife, creating new pathways for transmission (Magouras et al., 2020).
Recent anthropogenic changes in land use, such as rapid urbanization, intensified agriculture, deforestation, and habitat fragmentation, have notably increased the transmission of zoonotic diseases (White and Razgour, 2020). Furthermore, global phenomena like climate change, animal migration, and tourism have significant impacts on the emergence and re-emergence of zoonotic diseases (Rahman et al., 2020). Factors such as limited awareness, a preference for traditional medicines, cultural practices, and community poverty contribute to the transmission of zoonoses in the Indian subcontinent (Durrance-Bagale et al., 2021). The presence of an incomplete surveillance system, failure to detect early warning signals, and inadequate communication between sectors have likely heightened South Asia’s vulnerability to zoonotic diseases (Laxminarayan et al., 2017). Consequently, zoonoses account for a substantial 26% of the infectious disease burden in low-income South Asian countries, in stark contrast to the mere 0.7% observed in high-income countries (Grace et al., 2012). Given that infectious diseases transcend human-defined geographical boundaries, close surveillance of zoonotic diseases is imperative to mitigate risks.
Sri Lanka, a developing nation in South Asia with a population of nearly 22.1 million (World Bank data, 2022), faces significant vulnerability to the emergence and transmission of zoonotic diseases for several reasons. The country boasts rich biodiversity, including diverse wildlife such as mammals, birds, reptiles, amphibians, and marine and freshwater fish species (Don Bamunusinghage et al., 2020). Tourism plays a crucial role in Sri Lanka's economy, with ecotourism, involving safaris and adventure sports, being particularly popular (Fernando et al., 2016). However, ecotourism elevates the risk of pathogen transmission from animals to humans (Chomel et al., 2007). Furthermore, in rural and estate sectors, the primary source of household income is derived from agriculture and livestock farming (Senevirathna and Dharmadasa, 2021; Prasannath, 2015). The livestock sector encompasses cattle, buffaloes, poultry, swine, goat, and sheep farming, with notable population increases in cattle and buffalo in recent years (Livestock statistical bulletin, 2020). Rural livestock keepers are at high risk of zoonotic diseases due to frequent contact with their animals, consumption of livestock products, and limited access to health care facilities (Grace et al., 2017). Moreover, Sri Lanka’s tropical environmental conditions, characterized by high humidity and heavy monsoonal rainfall, further enhance the risk of zoonotic disease transmission (Schønning et al., 2019; Allen et al., 2017). Consequently, Sri Lanka requires a coordinated surveillance and monitoring system to proactively prevent the emergence and re-emergence of zoonotic diseases.
To the best of our knowledge, an updated systematic review addressing the incidence, diagnostic approach, and burden of zoonotic diseases reported in Sri Lanka has not been published in recent years. Therefore, conducting a comprehensive study to analyze historical and current zoonotic disease trends is essential to provide the latest data, information, and knowledge necessary to prevent the emergence and re-emergence of zoonotic diseases in Sri Lanka. This study serves as a timely and exhaustive systematic review of zoonoses reported over the past 22 years in Sri Lanka.
Materials and Methods
Systematic review protocol
This systematic review adhered to the guidelines provided by the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) statement (S1 File). A systematic literature search was conducted between July and September 2022, utilizing the following databases and sources: Google Scholar (https://scholar.google.com/), PubMed (https://pubmed.ncbi.nlm.nih.gov/), and the Cochrane Library (https://www.cochranelibrary.com/). In addition, incorporated data from the weekly epidemiological reports spanning from 2007 to 2022, as issued by the Epidemiology Unit of the Ministry of Health, Sri Lanka (https://www.epid.gov.lk/web/index.php?option=com_content&view=article&id=148&Itemid=449&lang=en). Furthermore, we conducted an analysis of rabies statistical bulletins published by the Public Health Veterinary Services, Ministry of Health, Sri Lanka (http://www.rabies.gov.lk/english/reports.php), covering the period from 2009 to 2022. Only reports that met the specified inclusion criteria were included in this study.
Inclusion and exclusion criteria
In this study, we included research articles, epidemiological reports, abstracts of proceedings, and case reports related to zoonotic diseases in humans in Sri Lanka, reported between 2000 and 2022. Zoonotic diseases were defined based on their recognition by the World Health Organization (WHO) (https://www.who.int/) and the Centers for Disease Control and Prevention (CDC) (https://www.cdc.gov/), or as documented in peer-reviewed journals. We limited our review to articles written in English.
Exclusions comprised overlapping or duplicate data, zoonotic diseases reported outside Sri Lanka, studies concerning frequently occurring zoonotic diseases where sufficient data were available, reports related to awareness and knowledge about zoonotic diseases, and studies with inadequate planning and insufficient information, as well as reports concerning nonzoonotic species or species that have evolved from original zoonotic sources and currently infect only animals or humans.
Search strategy
Initially, we identified 49 diseases as potential zoonoses that could be found in Sri Lanka based on information available from WHO and CDC websites, as well as published research and review articles in peer-reviewed journals. The names of zoonotic diseases and/or their causative agents were employed as search terms in web search engines. Search queries followed this order and utilized Boolean operators: Sri Lanka AND “Zoonotic disease” OR “Zoonosis,” Sri Lanka AND “disease name” OR “causative agent.”
Selection of studies and data extraction
Titles that aligned with the inclusion criteria were selected for article assessment. Four independent reviewers analyzed the chosen publications, evaluating criteria such as ethical and scientific study design, details regarding the study population, and the disease-causing organism. Extracted data were recorded in an Excel worksheet, covering aspects such as disease name, disease category based on etiologic agent, identified causative agent, source of test samples, number of subjects, type of sample collected, reported period, diagnostic techniques used, and significant study outcomes. The tabulated data were manually analyzed, and the results were synthesized into figures (graphs and maps) and tables. The complete search strategies, along with the report selection procedure, are illustrated in Figure 1.
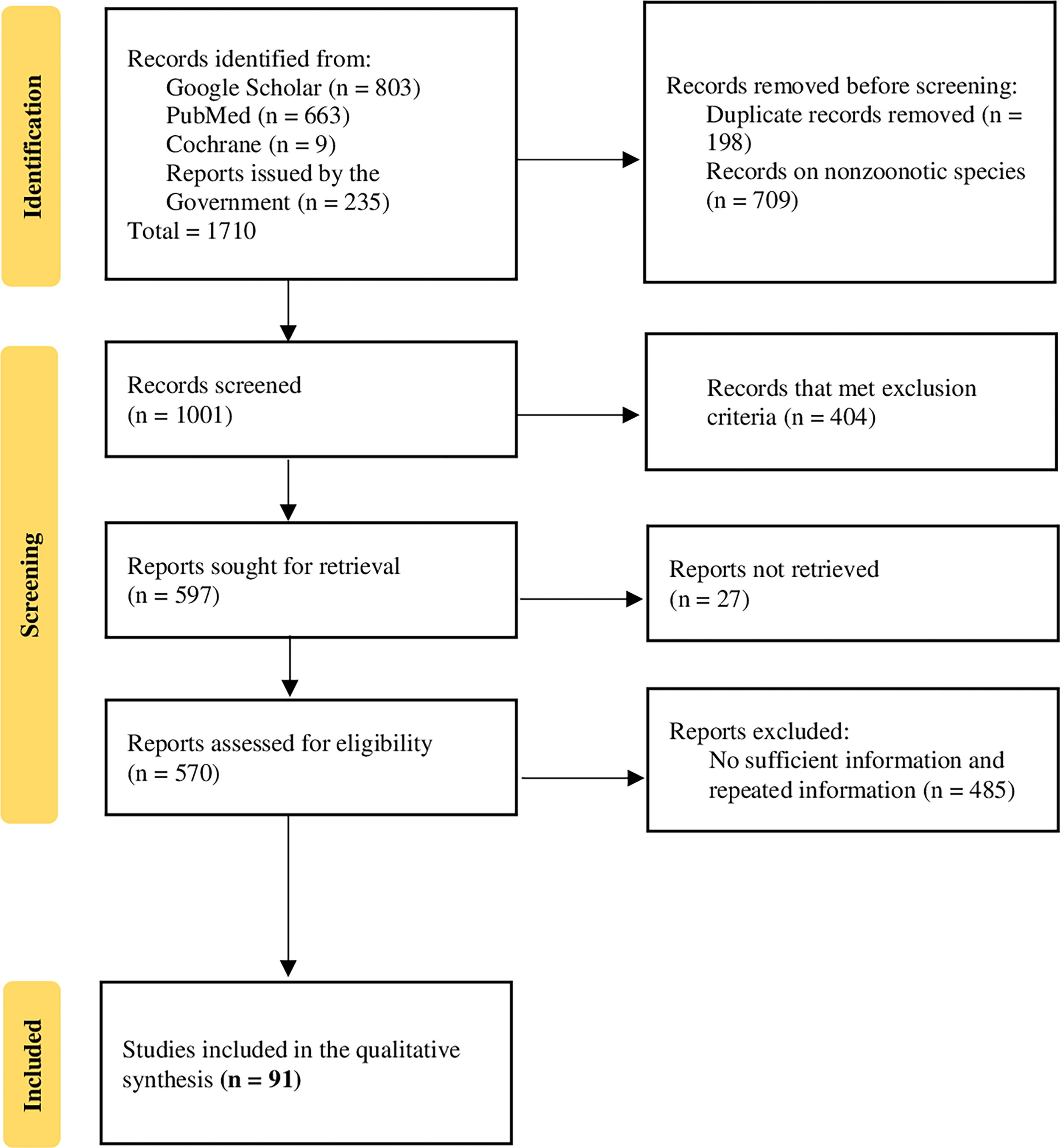
PRISMA flowchart describing the strategy followed to search and select the research articles and reviews for the results synthesis.
Results
Database search and selection process
The initial database search yielded a total of 1,710 articles. To ensure the quality and relevance of the selected articles, a rigorous manual screening process was conducted. During this manual screening, 198 duplicated records were identified and excluded. In addition, 709 reports focusing on nonzoonotic diseases were removed from consideration, along with 206 reports that did not meet the predefined inclusion criteria. Furthermore, 27 reports were deemed inaccessible and were also excluded from the study. Duplicated reports were identified based on matching criteria, including title, author(s), publication year, volume, issue number, and page number(s).
Following the manual screening process, 570 reports were assessed for eligibility. Out of these, 91 reports were selected for data extraction, as illustrated in Figure 1. The final selection encompassed a diverse range of sources, including 58 original research articles, 10 case reports, 16 weekly epidemiological reports, and 7 rabies statistical bulletins.
Distribution of selected studies
The selected studies provided comprehensive coverage of zoonotic diseases, including bacterial, viral, and parasitic zoonoses. Within this set of articles and case reports, 16 articles reported findings related to 7 bacterial zoonotic diseases, and 11 articles related to 7 viral zoonotic diseases. In addition, 28 articles examined various aspects of 14 parasitic zoonotic diseases.
The studies were further categorized based on their focus on humans or animals, resulting in 41 studies dedicated to zoonoses in humans and 14 studies centered on zoonotic diseases in animals. Table 1 provides a comprehensive overview of the included articles and case reports.
Details of Studies on Zoonotic Diseases in Sri Lanka (2000–2022)
Bacterial zoonoses
Leptospirosis
Leptospirosis stands as the most prevalent bacterial zoonotic disease reported in Sri Lanka. Between January 2007 and September 2022, a total of 78,263 leptospirosis cases were reported in the country. Notably, this disease gained significant attention following the 2008 outbreak in the Central Province of Sri Lanka, which resulted in 7,406 cases and 204 deaths, with a case-fatality rate of 1.3% in the endemic districts of Kegalle, Kandy, and Matale (Agampodi et al., 2011). In 2011, approximately 6,626 cases of leptospirosis were reported, coinciding with heavy rains and floods in the first quarter of the year (Bandara et al., 2015). Interestingly, the peak incidence occurred during the paddy harvesting season (Yathramullage and Meegaskumbura, 2016). In 2020, Sri Lanka experienced its highest number of leptospirosis cases (8,579), potentially influenced by increased farming activities or reduced attention to doxycycline prophylaxis due to the COVID-19 pandemic (Niriella et al., 2021). Studies have identified four pathogenic Leptospira species as potential causes of leptospirosis in Sri Lanka, namely, L. interrogans, L. weilii, L. borgpetersenii, and L. kirschneri (Jayasundara et al., 2021). Another study found that 34.1% of patients with undifferentiated febrile and clinically suspected leptospirosis were positive for leptospirosis (Warnasekara et al., 2022). Several risk factors for leptospirosis have been identified, including floods, heavy rainfall, exposure to rodents, and specific occupational activities such as agriculture, gem mining, construction work, and sand mining (Epidemiology Unit, 2016). In addition, cattle serve as important reservoirs for human leptospirosis (Gamage et al., 2014).
Rickettsioses
Rickettsioses stands out as the second most prevalent bacterial zoonotic disease in Sri Lanka. According to the Epidemiology Unit of the Ministry of Health in Sri Lanka, there were a total of 21,840 reported cases of typhus fever in the country from 2007 to 2022, with the highest number of cases (1,788) occurring in 2016 (Fig. 2B).
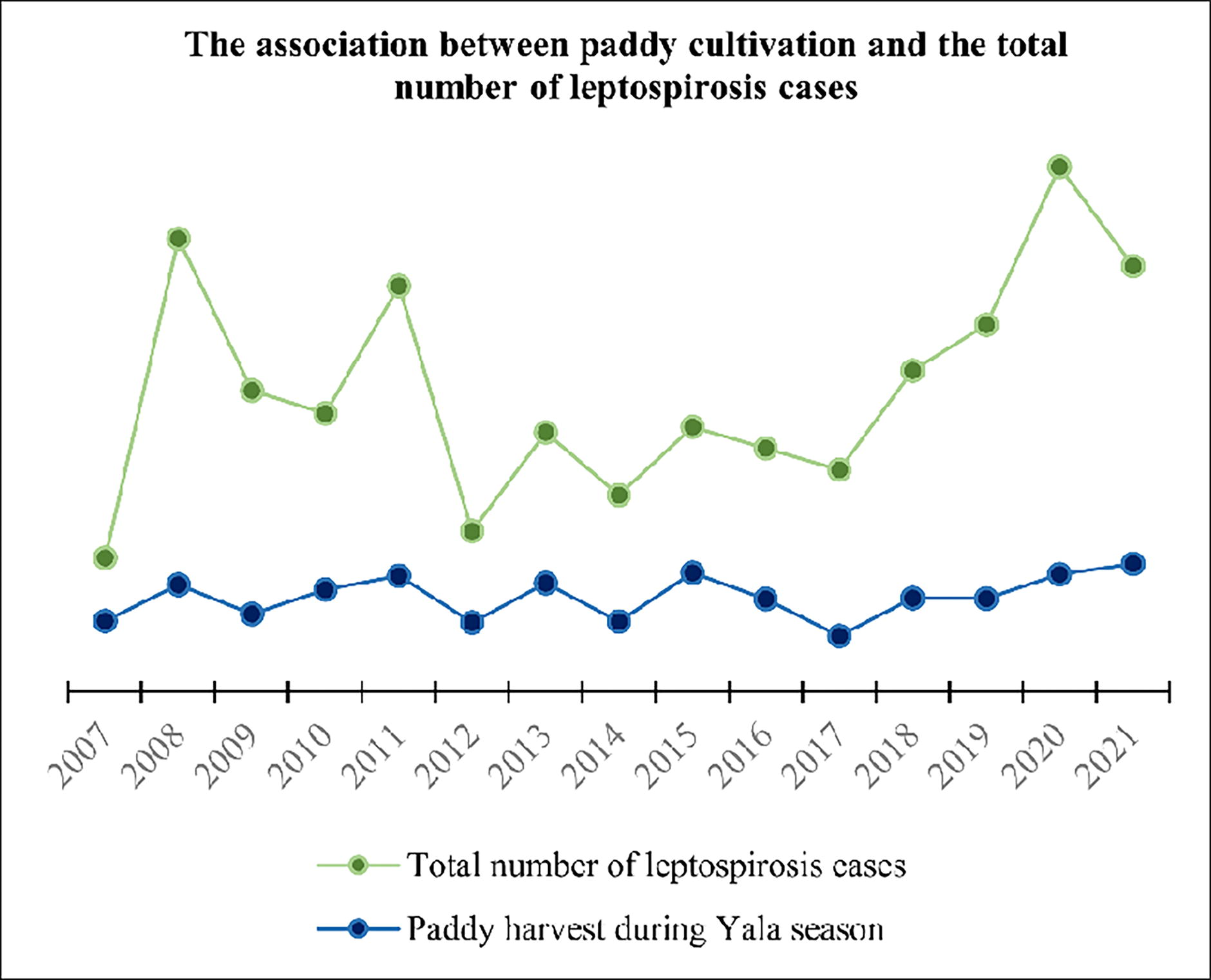
Impact of paddy cultivation on leptospirosis cases reported in Sri Lanka (2007–2021). Epidemiology Unit, Ministry of Health, Sri Lanka; Department of Census and Statistics, Sri Lanka.
To review the prevalence, risk factors, and diagnosis of spotted fever and typhus fever in Sri Lanka, we selected three hospital-based studies (Pradeepan et al., 2014; Premaratna et al., 2008; Kularatne et al., 2013). Two of these studies (Kularatne et al., 2013; Premaratna et al., 2008) assessed the prevalence of rickettsioses in the Western Province and Central Hills of Sri Lanka from 2002 to 2007. These studies revealed that out of 402 patients with suspected rickettsioses, 26 were infected with scrub typhus, and 63 were infected with spotted fever group infections. The Northern region of Sri Lanka also reported a notably high prevalence of scrub typhus, with an infection rate of 84.4% among patients older than 12 years between 2012 and 2013 (Pradeepan et al., 2014). In another study involving 178 patients from Matara, the findings indicated that 25 (14%) patients had scrub typhus, 6 (3%) had SFG rickettsioses, 3 (1.6%) had murine typhus, and 3 (1.6%) were infected by Rickettsia felis (Angelakis et al., 2012).
Brucellosis
Brucellosis is a recognized endemic zoonotic disease across the Asian continent, with notable impacts on livestock productivity and human health in the region. In a study by Karunanayake et al. (2019), the seroprevalence of human brucellosis was investigated in 1,294 healthy individuals living in the Central, North-West, North-Central, and Western Provinces of Sri Lanka between 2014 and 2015. The researchers conducted Standard Tube Agglutination Tests (SAT) using Brucella abortus and B. melitensis antigens, revealing that 8.4% of the study population tested seropositive for brucellosis. In addition, livestock farmers were identified as a high-risk group for Brucella infection (Karunanayake et al., 2019).
Bovine brucellosis has been reported in three provinces in Sri Lanka, specifically, Uva, North Central, and Sabaragamuwa. The Uva Province recorded the highest disease incidence, accounting for 72.5% of the cases.
Q fever
In 2009, Angelakis et al. (2012) conducted a retrospective investigation in Matara involving 178 patients who were suspected of having rickettsioses due to the presence of an eschar or a rash. The study revealed that 3 out of these patients (1.6%) had acute Q fever (Angelakis et al., 2012). No other publication about Q fever caused by Coxiella burnetii in Sri Lanka was identified in our search.
Shigellosis, campylobacteriosis, salmonellosis, and listeriosis
Shigella sp. is a zoonotic bacterium that can be transmitted to humans through the consumption of contaminated food or water. Two common pathogenic Shigella species are S. flexneri and S. sonnei, with S. flexneri being endemic in developing countries and frequently isolated worldwide (Epidemiology Unit, 2007). A study in Jaffna, Sri Lanka, investigated the presence of S. flexneri 11 and S. sonnei in children. It was reported that out of 346 children screened, 15 were found to be infected with Shigella sp., and it was noted that these affected individuals did not have access to clean water (Sathiadas et al., 2016).
Campylobacter sp. and Salmonella sp. are two major zoonotic bacterial pathogens responsible for food-borne illnesses and deaths worldwide. Contaminated meat, dairy products, and eggs are common sources of infection (Abebe et al., 2020). In Sri Lanka, the presence of Campylobacter jejuni was confirmed in free-roaming toque macaques (Tegner et al., 2019), while Salmonella sp. was detected in broiler chicken meat (prevalence rate of 11.6%) (Jayaweera et al, 2020). In addition, Kalupahana et al. (2018) reported the detection of Campylobacter sp. in broiler chicken and suggested that the tropical climate in Sri Lanka provides favorable conditions for Campylobacter colonization in its hosts (Kalupahana et al., 2018).
Listeriosis, a rare, but severe foodborne disease caused by the bacteria Listeria monocytogenes, can survive and multiply at low temperatures typically found in refrigerators, according to the WHO. In Sri Lanka, Listeria monocytogenes was detected in raw milk and other dairy products such as ice cream, pasteurized milk, curd, cheese, and yogurt. The distribution of raw milk contamination was significant, with the highest incidence in the Kandy and Gampaha districts of Sri Lanka (Wijendra et al., 2014). Moreover, Gunasena et al. (1995) reported the presence of Listeria monocytogenes in raw chicken and vegetables, including green leaves, cabbage, and lettuce, obtained from retail shops in Gampaha, Colombo, Kiribathgoda, and Dalugama (Gunasena et al., 1995).
Several food poisoning outbreaks in Sri Lanka have been linked to the consumption of contaminated food. For instance, in 2006, a food poisoning outbreak in Biyagama affected over 200 employees of a company, and contaminated chicken meat was identified as a possible cause. However, the specific causative pathogen was not identified.
Viral zoonoses
Hantavirus infection
Hantavirus infection is recognized as an emerging zoonotic infection in Sri Lanka (Gamage et al., 2011), with black rats and lesser bandicoot rats being identified as potential reservoir animals (Lokupathirage et al., 2019). The prevalence of hantavirus infection among people in the North-Central (Muthugala et al., 2021; Sunil-Chandra et al., 2020) and Central (Gamage et al., 2011) regions of Sri Lanka has been reported. However, it is suggested that hantavirus infection may have been underreported (Gamage et al., 2011) and misdiagnosed (Ehelepola et al., 2018) in Sri Lanka due to its close clinical resemblance and epidemiological characteristics to leptospirosis.
A study conducted in Kandy, Sri Lanka, aimed to determine the prevalence of hantavirus infection among 105 suspected leptospirosis patients. The study revealed that 8 patients from the study group tested positive for hantavirus antibodies (Gamage et al., 2011). In another hospital-based study, the prevalence of hantavirus infection was investigated in 72 patients admitted to two hospitals in the North-Central Province of Sri Lanka, with symptoms resembling hemorrhagic fever with renal syndrome and hantavirus pulmonary syndrome. The study reported that 40.28% of the patients screened were found to be positive for hantavirus IgM (Muthugala et al., 2021). However, the infection may have been underreported and misdiagnosed due to its clinical and epidemiological similarities to leptospirosis.
Rabies
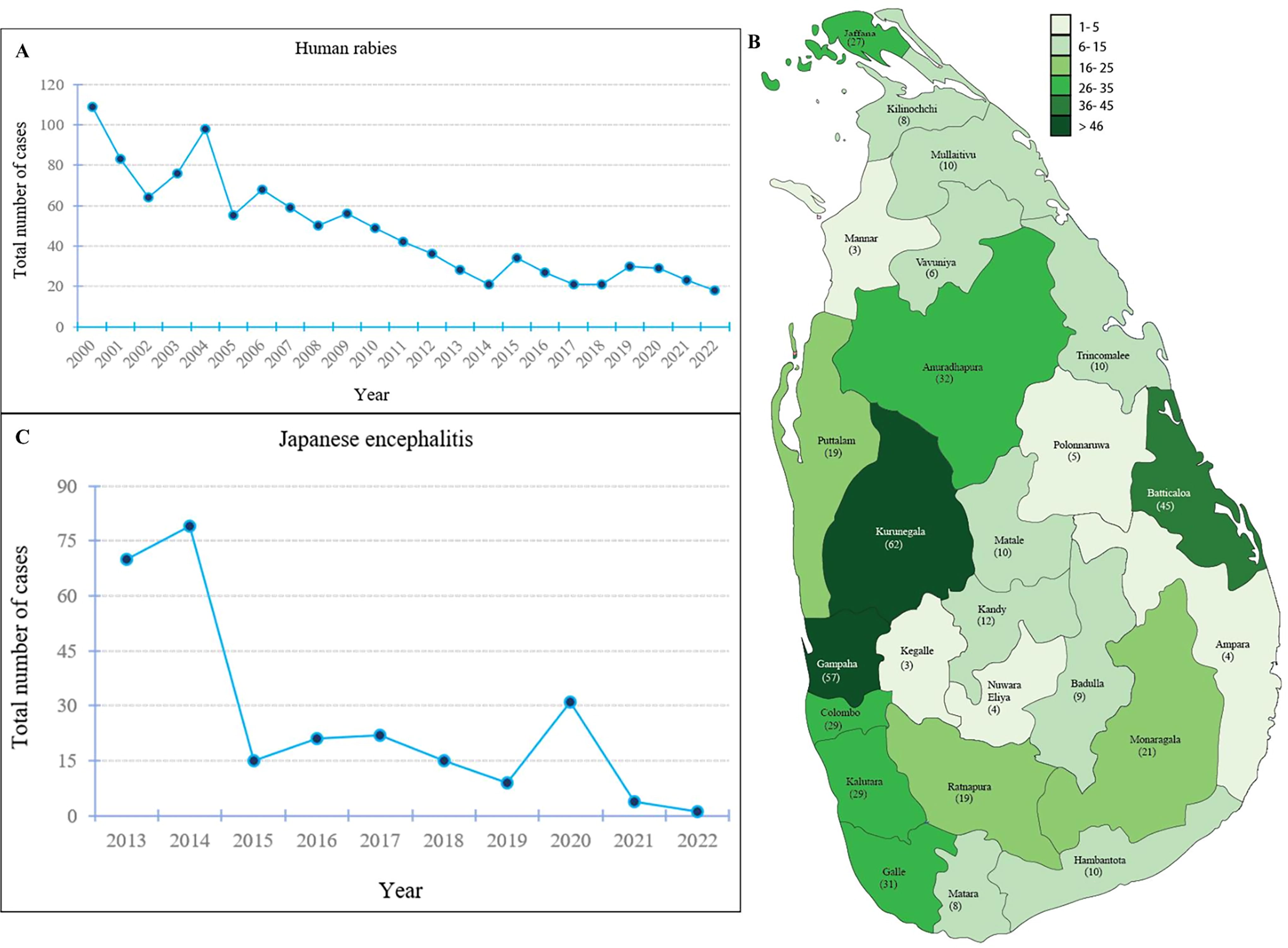
From 2000 to 2021, Sri Lanka reported a total of 1079 human rabies cases. The highest number of human rabies cases, with 109 cases, was documented in the year 2000. Nevertheless, the annual count of human rabies cases reported has consistently decreased since 2006 (Fig. 3). In 1984, Sri Lanka declared seven districts—Kurunegala, Colombo, Kalutara, Gampaha, Galle, Hambantota, and Matara—as rabies-endemic areas.
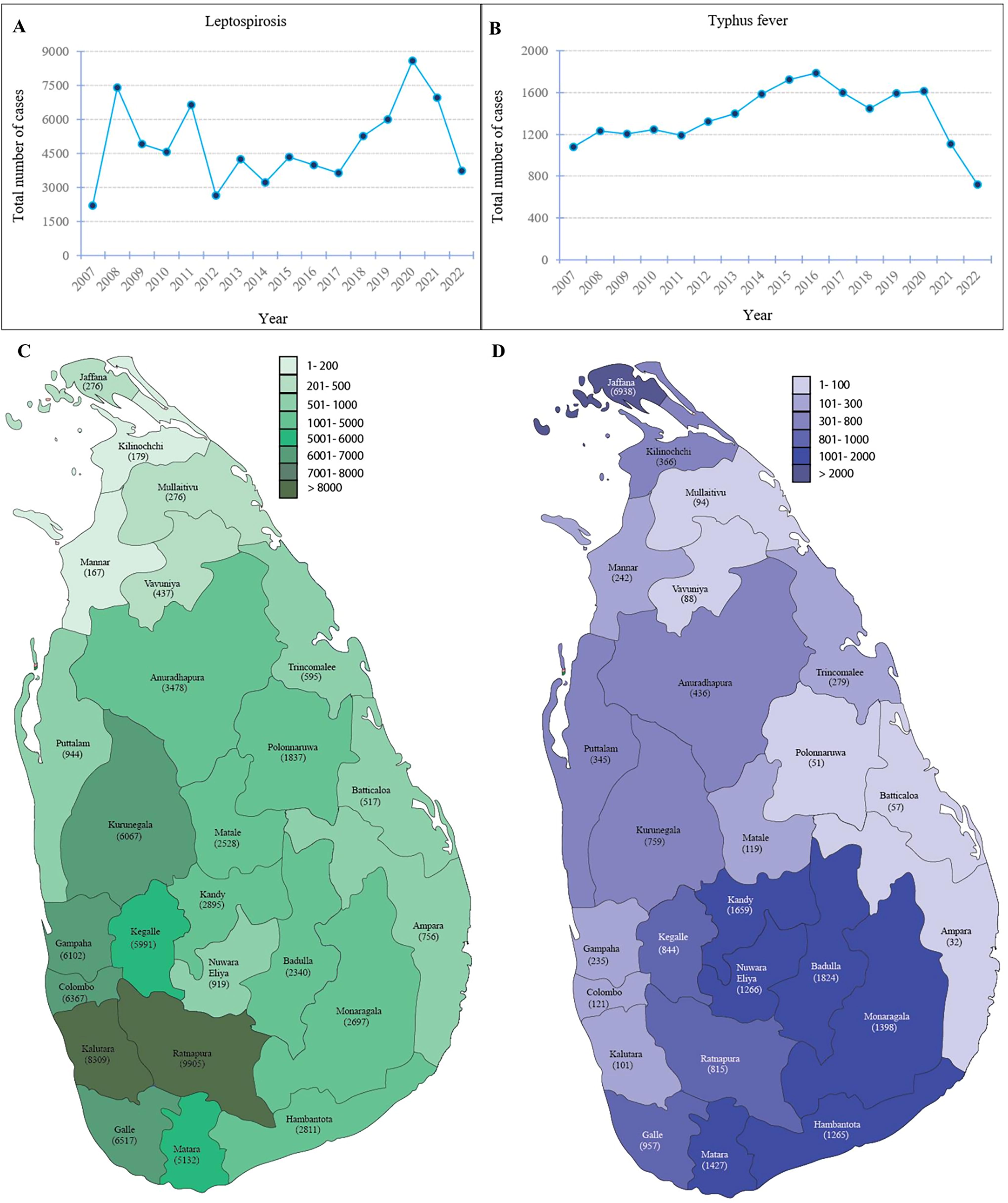
Yearly fluctuations and geographical distribution of leptospirosis and typhus cases reported in Sri Lanka.
A significant proportion of human rabies cases in Sri Lanka were attributed to bites from stray dogs and household pets. For instance, in 2016, 20 human rabies cases were reported in the country, with ten cases resulting from stray dog bites and four from household pet bites (Epidemiology Unit, 2017). Matsumoto et al, (2013) diagnosed 79 human rabies cases between 2008 and 2010, analyzing brain samples sent to the Rabies Diagnosis and Research Laboratory in Colombo, Sri Lanka. Their findings revealed that 92.2% of patients were bitten by dogs, while 7.8% were bitten by cats (Matsumoto et al., 2013).
The prevalence of the rabies virus in dogs in Sri Lanka was assessed through 57 canine brain samples submitted for screening at the University of Peradeniya from 2007 to 2011. Among these samples, 53 were found to be positive for the rabies virus (Beck et al., 2017). Moreover, free-roaming mongooses were identified as potential reservoirs for the rabies virus in Sri Lanka (Patabendige and Wimalaratne, 2003). The Veterinary Epidemiological Bulletin, issued in 2013, reported a significant number of rabies cases among cattle, buffalo, swine, and goats as well.
Figure 4A shows the total number of human rabies cases reported in each district in Sri Lanka from January 2008 to September 2022. During this period, the highest number of human rabies cases (62 cases) was recorded in the Kurunegala district, while the lowest number of cases (3 cases) was reported in Kegalle and Mannar districts.
Influenza a
Swine in Sri Lanka have been found to harbor influenza A viruses genetically similar to human influenza A (H3N2) and A (H1N1) pdm09 viruses. Furthermore, the country has witnessed two instances of A (H1N1) pdm09 virus transmission from humans to pigs (Perera et al., 2013).
A total of three studies, comprising two hospital-based investigations (Perera et al., 2010; Lamabadusuriya, 2001) and one animal-based study (Perera et al., 2013), have reported the occurrence of zoonotic influenza A virus infection in Sri Lanka (Table 1). Perera et al. (2010) conducted a study involving patients admitted to the Outpatient Department at Colombo North Teaching Hospital for the treatment of acute upper respiratory tract infections from 2003 to 2004. Their findings revealed that 8% of the patients were infected with influenza A virus. Particularly, the majority (13 out of 24) of the infected patients were younger than 15 years. In addition, it was observed that the influenza viruses detected in Sri Lanka closely resembled the viruses identified in both the Northern and Southern hemispheres (Perera et al., 2010). In another study, Lamabadusuriya (2001) investigated 30 febrile patients 6 months to 10 years of age, who were admitted to the Lady Ridgeway Hospital in Colombo. Among the screened patients, zoonotic influenza A (H3N2) was detected (Lamabadusuriya, 2001).
Japanese encephalitis
Japanese encephalitis, a vector-borne zoonotic disease, can be effectively controlled using a live attenuated vaccine (Erlanger et al., 2009). According to the Epidemiology Unit of the Ministry of Health in Sri Lanka, 266 Japanese encephalitis cases were reported from 2013 to 2021. The highest number of cases, totaling 79, was reported in 2014. However, the number of reported Japanese encephalitis cases significantly decreased to 15 in 2015 and further dropped to 4 in 2021.
In a study by Jeewandara et al. (2015), 1689 dengue patients admitted to the Family Practice Center at the University of Sri Jayewardenepura, Sri Lanka, were screened for Japanese encephalitis. The findings revealed that both children and adults admitted for dengue infection were likely to test seropositive for Japanese encephalitis virus antibodies (Jeewandara et al., 2015).
West Nile virus infection
West Nile virus infection is a mosquito-borne zoonotic disease. Although it has been reported in India (Khan et al., 2011), there was no prior report of its transmission in Sri Lanka until 2015. Lohitharajah et al. (2015) conducted an enzyme-linked immunosorbent assay and a plaque reduction neutralization test to detect West Nile virus IgM in 108 clinically diagnosed encephalitis patients admitted to the National Hospital and the Lady Ridgeway Hospital in Colombo, Sri Lanka. Their study revealed that 2.8% of the study population tested positive for West Nile virus neuroinvasive disease, and these patients were between 17 and 49 years of age (Lohitharajah et al., 2015).
According to the World Health Organization (WHO), no vaccine against the West Nile virus has been approved for use in humans at present. However, integrated and comprehensive mosquito control programs, along with studies identifying local mosquito species involved in West Nile virus transmission, play a crucial role in preventing the transmission of this infection.
Monkeypox
The first case of monkeypox was diagnosed in an individual who had recently returned from Dubai, United Arab Emirates (UAE), in November 2022. This person exhibited symptoms such as enlarged lymph nodes, exhaustion, fever, and the development of skin blisters. Shortly thereafter, a second case was reported in a man who had also returned from the same country, as indicated by the Ministry of Health in Sri Lanka. It is worth noting that locally acquired monkeypox cases have not been reported in the country to date.
Chikungunya
The chikungunya virus, a member of the alphavirus family, is primarily transmitted by mosquitoes of the Aedes genus (Hapuarachchi et al., 2010; Schuffenecker et al., 2006). In Sri Lanka, the first documented case of chikungunya virus infection dates back to 1965 (Munasinghe et al., 1966). However, the virus experienced a re-emergence in 2006, resulting in a significant outbreak. Between 2006 and 2007, approximately 40,000 individuals in Sri Lanka were affected by this infectious disease (Hapuarachchi et al., 2010). It is noteworthy that 2006 also marked the first reported instance of coinfection with chikungunya and dengue in Sri Lanka (Hapuarachchi et al., 2008). In 2008, there was a resurgence in the number of reported cases, with figures similar to those seen in 2006–2007 (Hapuarachchi et al., 2010).
A study conducted in 2007 in southern Sri Lanka provided insights into the prevalence of the chikungunya virus. The research revealed that the chikungunya virus was detected in 28 out of 797 patients who presented with febrile illness, highlighting its significant role as a cause of nonspecific acute febrile illness in the southern region of the country (Reller et al., 2013).
In 2010, Hapuarachchi et al reported the presence of a mutated strain of the chikungunya virus circulating in Asia, including Sri Lanka. This mutation was found to enhance the virus's transmissibility by Aedes albopictus mosquitoes. Given the outdoor nature of these mosquitoes and their widespread distribution globally, this infection poses a substantial global threat. Therefore, it is imperative to implement effective vector control strategies to mitigate the risk of unforeseen outbreaks.
Parasitic zoonoses
Protozoa
Toxoplasmosis
Toxoplasmosis, a parasitic zoonosis with a broad geographical distribution, is caused by the protozoan parasite Toxoplasma gondii, affecting a wide range of hosts (Khan et al., 2017). During pregnancy, Toxoplasmosis poses a risk of transplacental transmission and can lead to severe fetal anomalies (Montoya and Rosso, 2005). Several cases of toxoplasmosis have been reported among pregnant women in Sri Lanka, particularly in those attending hospitals such as Colombo North Teaching Hospital (Chandrasena et al, 2016), Teaching Hospital Peradeniya (Iddawela et al., 2017), and Colombo De Soyza Maternity Hospital (Subasinghe et al., 2011).
Studies in Sri Lanka have shown that out of 393 pregnant women who visited two hospitals in Colombo between 2009 and 2014, 64 tested seropositive for anti-T. gondii IgG antibodies. However, none of the participants was positive for anti-T. gondii IgM antibodies (Chandrasena et al., 2016; Subasinghe et al., 2011). In another study involving pregnant women at the Teaching Hospital Peradeniya between 2010 and 2013, 60 were found to be positive for T. gondii IgG antibodies, with only 2 testing positive for T. gondii IgM antibodies (Iddawela et al., 2017).
An association was reported between Toxoplasma seroprevalence among pregnant women and the consumption of commercially prepared meals in Sri Lanka (Chandrasena et al., 2016). In addition, a study revealed significant associations between T. gondii infection and activities such as home gardening (p = 0.01) and the preparation and sale of meat (p = 0.05) (Iddawela et al., 2017). However, no significant association was found between T. gondii seropositivity and other risk factors, including contact with cats, blood transfusion, organ transplantation, or consumption of undercooked meat (Subasinghe et al., 2011).
According to the CDC, domestic cats and other felids are the only known definitive hosts for T. gondii. In Sri Lanka, an infection rate of 30.2% was reported for toxoplasmosis in cats in Colombo, in 2008 (Kulasena et al., 2011). Furthermore, in 2006, a study testing 86 stray dogs in Sri Lanka revealed a seroprevalence of 67.4% for T. gondii using MAT (Dubey et al, 2007).
Giardiasis
Giardiasis, a water-borne disease commonly found in impoverished rural communities, is often associated with poor hygiene practices and limited health education. A survey involving 489 children (1–12 years of age) in a tea plantation community in Sri Lanka's Kandy district reported an infection rate of 0.2% for Giardia intestinalis (Galgamuwa et al., 2016). In addition, G. intestinalis assemblages A and E were identified in fecal samples from cattle in Sri Lanka (Abeywardena et al., 2014).
Plasmodium knowlesi
Plasmodium knowlesi is a zoonotic protozoan parasite causing malaria in humans and is widely distributed in Southeast Asia. Its natural hosts are pig-tailed and long-tailed macaques (Singh and Daneshvar, 2013). Sri Lanka reported only one imported case of P. knowlesi infection (Dharmawardena et al., 2017).
Cryptosporidiosis
Cryptosporidium, a cause of childhood watery diarrhea in Sri Lanka, is commonly caused by Cryptosporidium parvum and can be zoonotically transmitted (Zahedi et al., 2016). Cryptosporidium sp. was identified among children younger than three years with watery diarrhea, admitted to four hospitals in the Central Province of Sri Lanka from 2011 to 2013. Positive cases had a history of animal contact, although the species was not identified (Sirisena et al, 2014). In addition, a case of C. parvum infection was reported in a child who underwent kidney transplantation (Weerasooriya et al., 2020). Cryptosporidium was also detected in toque macaques, gray langurs, and purple-faced langurs, marking the first report of Cryptosporidium infection in wild primates inhabiting natural forests in Sri Lanka (Ekanayake et al., 2006). Furthermore, C. bovis, C. ryanae, and six new genotypes were detected in cattle using PCR-based mutation scanning-targeted sequencing of the small subunit of nuclear ribosomal RNA, although C. parvum was not identified in preweaned calves (Abeywardena et al., 2014).
Nematodes
Brugian filariasis
Lymphatic filariasis, caused by Wuchereria bancrofti, and Brugia malayi, was previously endemic in several Sri Lankan districts, but the country has successfully controlled it through mass drug administrations. However, the emerging of brugian filariasis has been reported among children 7 to 12 years of age in the Colombo and Gampaha districts of Sri Lanka. In addition, nine individuals from the Gampaha district tested positive for anti-Brugia antibodies, suggesting subperiodic transmission of Brugia spp. (Chandrasena et al., 2016). Dogs and cats were found to be potential reservoirs for human brugian filariasis, with Brugia malayi infection reported in 36 (14.4%) dogs and 18 (13.4%) cats out of 250 dogs and 134 cats screened in the Gampaha district, Sri Lanka (Mallawarachchi et al., 2018b).
Dirofilariasis
Dirofilariasis is caused by parasitic nematodes of the genus Dirofilaria, with Dirofilaria repens, D. immitis, and D. tenuis being the most commonly detected species in humans. Sri Lanka has reported over 173 cases of human dirofilariasis, primarily caused by D. repens, in various districts since 1962. Clinical presentations often include ocular, oral, and cutaneous dirofilariasis (Iddawela et al., 2015; Jayasinghe et al., 2015). Ocular dirofilariasis is particularly prevalent in the Central Province of Sri Lanka, with a significant proportion of cases (70%) occurring in females 40 to 49 years of age (Iddawela et al., 2015). Canine dirofilariasis due to D. repens is a well-established parasitic disease in dogs and cats in Sri Lanka, with high prevalence (∼60%) reported in districts such as Gampaha, Puttalam, and Colombo (Dasanayake et al., 2022; Mallawarachchi et al., 2018a).
Toxocariasis
Toxocariasis is caused by the accidental ingestion of embryonated eggs of ascarid nematodes, Toxocara canis, and Toxocara cati, with dogs and cats as the main definitive hosts. In Sri Lanka, communities with limited access to public health and veterinary services are highly susceptible to the infection. For example, Hindagala in the Central Province of Sri Lanka reported a 43% seroprevalence for toxocariasis in children (Iddawela et al., 2003). In addition, T. canis was found in dogs, and its eggs were detected in the soil of a low-income tea estate community in the Central Province (Bandaranayaka et al., 2019). A 2017 seroprevalence study found that 62% of participants were seropositive for toxocariasis, with the highest seropositivity occurring in the 10- to 14-year-age group. Clinical presentations in seropositive cases often included unilateral reduced vision and red eye (Iddawela et al., 2017).
Angiostrongyliasis
Angiostrongyliasis is caused by Angiostrongylus cantonensis and is transmitted to humans through the ingestion of raw or undercooked slugs or snails. Although the consumption of slugs or snails is rare in Sri Lanka, a case report described a 25-year-old female in the Colombo district with Angiostrongylus infection in the vitreous eye (Ihalamulla et al., 2007). The mode of infection in Sri Lanka is likely through the consumption of fresh salads or vegetables contaminated with infected snails or slugs (Wang et al., 2008; Ihalamulla et al., 2007).
Hookworms
Zoonotic hookworm infections in humans are mainly caused by parasitic nematodes Ancylostoma ceylanicum, Ancylostoma braziliense, and Ancylostoma caninum from dogs and cats (Mallawarachchi and Samarasinghe, 2020; Bowman et al., 2010). A recent report described a 70-year-old female patient infected with A. ceylanicum in Sri Lanka (Mallawarachchi and Samarasinghe, 2020).
Cestodes
Bertielliasis
Bertielliasis, caused by Bertiella studeri, has been reported in various regions across South East Asia, South Asia, the Middle East, and Sub-Saharan Africa. This parasitic cestode primarily infects Old World monkeys. In Sri Lanka, human infections with B. studeri have been reported from the Southern Province (Karunaweera et al., 2001), the Sabaragamuwa Province (Morawakkorala et al., 2006), and the Central Province (Amarasinghe et al., 2020). Most reported patients in Sri Lanka were children younger than 11 years, and transmission typically occurs through accidental ingestion of the cysticercoid stage in infected intermediate host mites (Amarasinghe et al., 2020). Settlements bordering jungles in Sri Lanka are at a higher risk of infection due to frequent visits by Ceylon torque monkeys and gray langurs. Habitat loss due to deforestation and urbanization has led to increased monkey–human interactions, as the monkeys scavenge for food (Morawakkorala et al., 2006).
Sparganosis
Sparganosis is caused by the cestode Spirometra, which resides in snakes and frogs. Humans become infected through the consumption of raw or undercooked meat from frogs and snakes, drinking contaminated water, or applying poultices. Although Sri Lankans do not typically consume frog or snake meat, one case report described two patients from the Kurunegala and Kalutara districts infected with Spirometra sp. in the anterior abdominal wall (Dissanaike et al., 2001). In addition, the first case of cerebral sparganosis in Sri Lanka was reported in a 13-year-old boy in 2007 (Alibhoy et al., 2009). The most likely mode of infection in Sri Lanka is accidental ingestion of contaminated water containing Spirometra larvae, as poultices made from infected hosts are not commonly used (Alibhoy et al., 2009).
Zoonoses caused by other cestodes
Hydatidosis, a zoonotic disease caused by Echinococcus granulosus, is rare in native Sri Lankans, with most reported cases occurring in foreigners or individuals who have traveled to Central Asian countries (Matossian et al., 1997). Hymenolepis diminuta and Taenia taeniaeformis have been reported in human patients by clinicians and parasitologists in Sri Lanka, with case reports of hymenolepiasis caused by H. diminuta in a five-year-old boy (Sinhabahu et al., 2014) and T. taeniaeformis infection in a 7-year-old girl from a densely populated slum area in Colombo (Ekanayake et al., 1999). In addition, two case reports have described pet-associated Dipylidium caninum infections in children in Sri Lanka (Wijesundera and Ranaweera, 1989).
Discussion
Sri Lanka has a free health care system dedicated to maintaining continuous and quality health care services, ensuring clinical effectiveness and patient safety. The country's central health budget allocations have seen a consistent increase from 2015 to 2021. In 2021, LKR 212.3 billion was allocated for the health sector, with LKR 1.5 billion earmarked for the control of communicable and noncommunicable diseases (UNICEF, 2021). The Epidemiological Unit, established with assistance from the WHO, plays a pivotal role in bolstering surveillance, prevention, and control of communicable diseases, while ensuring the efficient dissemination of epidemiological information across the nation.
Despite these efforts, communicable diseases remain a significant health challenge in Sri Lanka. A substantial portion of the communicable disease burden is attributed to zoonoses. This study was undertaken to identify zoonotic diseases reported in Sri Lanka from 2000 to 2022.
Our findings, in conjunction with data from the Epidemiological Unit, Ministry of Health, Sri Lanka, revealed that leptospirosis is the most prevalent zoonotic disease, responsible for the highest number of reported cases in the country during the period from 2007 to 2022. Despite vigilant surveillance and systematic outpatient and inpatient management, over 150 leptospirosis cases were reported in each district of Sri Lanka during the study period. Notably, we observed an association between leptospirosis incidence and paddy cultivation during the “Yala” and “Maha” seasons, (May to August) (Fig. 3), where case numbers surged significantly, despite numerous control measures and guidance provided to paddy farmers (Yathramullage and Meegaskumbura, 2016).
The Ratnapura district, renowned for its gem mining industry, documented the highest number of leptospirosis cases, totaling 9,905 between 2007 and 2022. The Kalutara district ranked second in the number of reported cases, potentially linked to the increased occurrence of storms and floods in the region (Grama Niladhari Divisions Statistics-Kalutara District, 2020). The proliferation of rodents in urban areas due to rapid urbanization further compounds this issue (Agampodi et al., 2011). In Sri Lanka, small mammals such as Rattus, Bandicota indica, B. bengalensis, Mus musculus, Mus cervicolor, and Suncus murinus (Yathramullage and Meegaskumbura, 2016) are recognized as significant reservoirs for human leptospirosis. The elevated incidence of leptospirosis cases in Colombo, Galle, and Gampaha districts may be attributed to higher rodent populations in urban settings (Fig. 2C). In addition, cattle serve as important reservoirs for human leptospirosis (Gamage et al., 2014).
For early leptospirosis diagnosis, various methods, including indirect hemagglutination assays, ELISA, hemolytic tests, immobilized antigen dipsticks, and lateral flow assays, are employed. However, the microscopic agglutination test (MAT) is considered the gold standard serological test for diagnosing leptospirosis (WHO, 2009). In Sri Lanka, PCR is the most widely used diagnostic method for human leptospirosis. Furthermore, it has been determined that IgM ELISA is more sensitive than MAT for early and acute phase diagnosis, while immunochromatography tests can be utilized for rapid diagnosis (Niloofa et al., 2015).
The major risk factors for rickettsioses in Sri Lanka include high exposure to scrub jungles (Kularatne et al., 2013; De Silva et al., 2012) and contact with domesticated animals (Liyanaarachchi et al., 2015; Nanayakkara et al., 2013). In the Central Hills of Sri Lanka, ticks on dogs and wild boars were identified as possible vectors of spotted fever group infections (Kularatne et al., 2013). The geographical distribution of typhus fever showed an association with risk factors. Figure 2D illustrates the geographical distribution of typhus fever, with the Jaffna district reporting the highest number of cases. In Jaffna, most children infected with scrub typhus had been exposed to household pets (mainly dogs), slept on the floor, or lived in proximity to jungles (Sathiadas et al., 2013). Apart from the Northern region, a relatively high number of typhus cases were reported in districts like Kandy, Nuwara Eliya, Monaragala, Hambantota, Badulla, and Matara, while the Ampara district reported the lowest number of typhus fever cases during the study period (Fig. 2D).
Torgerson et al. (2015) estimated the worldwide burden of leptospirosis to be 2.90 million Disability-Adjusted Life Years (DALYs) annually, with Sri Lanka experiencing a burden exceeding 500 DALYs per 100,000 individuals per year. However, it is worth noting that our study did not involve the calculation of DALYs. Instead, our systematic review focused solely on the prevalence of leptospirosis in Sri Lanka. Similarly, Costa et al. (2015) reported a prevalence of over 100 cases of leptospirosis per 100,000 population in Sri Lanka. Although we did not calculate the DALYs, our results indicate that the annual prevalence of leptospirosis was significantly higher during our study period. Moreover, Torgerson et al. (2015) reported that morbidity rates were notably elevated in studies conducted among rural populations and tropical areas when compared to urban settings within the region.
For diagnosing typhus and spotted fever group rickettsioses, the “gold standard” technique is the immunofluorescence assay (IFA). However, other serological tests such as ELISA and Weil-Felix are also widely used for diagnostic purposes. In addition, molecular methods such as PCRs and DNA sequencing enable the rapid identification of rickettsiae at the species level (Stewart and Stewart, 2021). In Sri Lanka, the diagnosis of rickettsioses employs immunofluorescence antibody tests (Kularatne et al., 2013; Nanayakkara et al., 2013), IgG and IgM ELISA (Pradeepan et al., 2014), PCR (Liyanaarachchi et al., 2015), and basic biochemical tests (Premaratna et al., 2008).
Factors hindering the control of certain bacterial zoonoses in the country include poverty and lack of awareness among high-risk groups. Infections such as rickettsioses (Sathiadas et al., 2013) and brucellosis (Karunanayake et al., 2019; Kothalawala et al., 2018) were primarily reported among low-income and/or rural communities with limited access to infrastructure and health education. We also noted that the true burden of some bacterial zoonoses may not have been accurately assessed due to symptomatic diagnosis. Patients with fever, for example, are frequently reported in the country, and etiologies are not always confirmed. We observed that Q fever was reported as the etiological factor among patients with an unknown origin of fever (Angelakis et al., 2012). Furthermore, foodborne bacterial zoonotic diseases may have been underreported in the country due to treatment procedures that rely solely on symptoms. Although we found one study reporting zoonotic Shigella sp. in children in Jaffna (Sathiadas et al., 2016), we found no scientific report on campylobacteriosis or salmonellosis, despite these pathogens being identified as the main causes of food poisoning worldwide by the WHO. However, the detection of foodborne bacterial pathogens in wild animals, such as toque macaques (Tegner et al., 2019), and in food (Jayaweera et al., 2020; Wijendra et al., 2014; Gunasena et al., 1995) suggests the potential for future outbreaks in the country. Therefore, we recommend revising and implementing national standards to enhance the quality of food consumed by the population and conducting systematic investigations into food poisoning complaints to minimize or prevent unforeseen threats from bacterial foodborne infections.
In the early 2000s, the Sri Lankan government allocated nearly $3.0 million per year for rabies and Japanese encephalitis immunization programs (Nanayakkara et al., 2003; Attanyake and Stevenson, 2001). As a result, Sri Lanka witnessed a notable decline in the incidence of Japanese encephalitis (Epidemiology unit MoH, Sri Lanka, 2012) and rabies over the last decade (Silva, 2016).
In 1988, the Epidemiology Unit of the Ministry of Health initiated an immunization program against Japanese encephalitis, targeting children one to ten years of age. Interestingly, in the postvaccination era, Japanese encephalitis cases were predominantly reported in individuals older than 30 years, who had not been immunized against the disease (Epidemiology Unit, MoH, 2012). The Department of Animal Production and Health in Sri Lanka previously conducted a program to immunize pigs, which serve as important amplifying hosts for Japanese encephalitis (McLean and Graham, 2022). However, the Epidemiology Unit of the Ministry of Health in Sri Lanka suggested that this program could be discontinued due to its ineffectiveness (Epidemiology Unit, MoH, 2012). Nevertheless, Peiris et al. (1992) reported that the reduction in vector infection with the Japanese encephalitis virus was roughly proportional to the extent of the pig vaccination program (Peiris et al., 1992).
The reduction in the number of human rabies cases in Sri Lanka since 2006 can be attributed to antirabies vaccination programs for dogs and community awareness initiatives conducted by government agencies (Silva, 2016). For instance, according to Public Health Veterinary Services, Sri Lanka administered 1.5 million and 1.3 million antirabies vaccines in the years 2014 and 2017, underscoring the importance of these vaccination programs in the country's efforts to eliminate rabies. However, there is a need to investigate the presence of rabies virus in animals other than canines, such as cattle, buffalo, swine, goats, and wildlife, to identify potential reservoirs of rabies in the country. Although the incidence of Japanese encephalitis is decreasing in the known hot spots of the country, it appears to be spreading to new areas that previously had a low level of transmission (Epidemiology unit MoH, Sri Lanka, 2012). Therefore, we emphasize the importance of surveillance programs following mass immunizations to assess the success of immunization programs.
Nonhuman primates, along with other vertebrates, are believed to serve as amplification hosts for chikungunya virus. In Zimbabwe, African green monkeys and chacma baboons (Papio ursinus) have been identified as significant hosts (McIntosh et al., 1964). In addition, the chikungunya virus has been isolated from African green monkeys, Patas monkeys (Erythrocebus patas), and Guinea baboons (Papio papio) in Senegal (Diallo et al., 1999). Seropositivity to the virus has also been observed in chimpanzees in the Congo (Osterrieth et al., 1920). However, conclusive evidence of enzootic circulation of the chikungunya virus in Sri Lanka is lacking. Therefore, comprehensive studies are warranted to investigate the potential enzootic transmission of the chikungunya virus in Sri Lanka.
Enzootic transmission of the West Nile virus primarily involves mosquitoes, migratory birds, horses, and crocodiles (Habarugira et al., 2020). However, to date, no study has been conducted on the enzootic transmission of the West Nile virus in Sri Lanka. Therefore, we emphasize the importance of investigating the epidemiology and animal reservoirs of the West Nile virus in Sri Lanka.
The global incidence and burden of congenital toxoplasmosis (190,100 annual cases, with a 95% CI of 179,300–206,300) were estimated by region. This equates to an incidence rate of approximately 1.5 cases of CT per 1000 live births. However, it is notable that the South Asia region, including Sri Lanka, was excluded or not considered in this study. The areas included in the analysis were AFR (African Region), AMR (Region of the Americas), CI (credible interval), DALYs (Disability-Adjusted Life Years), EMR (Eastern Mediterranean Region), EUR (European Region), SEAR (South-East Asia Region), and WPR (Western Pacific Region) (Torgerson and Pierpaolo., 2013). However, in our analysis, we presented the reported prevalence of toxoplasmosis in Sri Lanka without calculating the DALYs. Although studies in Sri Lanka have been limited to specific areas, comprehensive island-wide surveys of congenital toxoplasmosis have not been conducted to determine its true prevalence and incidence rates. Thus, these findings highlight the importance of conducting seroprevalence studies and understanding and addressing the risk factors associated with toxoplasmosis transmission, especially among pregnant women, to mitigate the potential adverse effects on fetal health.
Parasitic zoonoses accounted for a smaller number of cases compared to bacterial and viral zoonoses. However, we identified 14 parasitic zoonoses that infected people in Sri Lanka. Toxoplasmosis was reported among pregnant women in Sri Lanka (Iddawela et al., 2017; Chandrasena et al., 2016; Subasinghe et al., 2011), but its pooled prevalence in Sri Lanka was lower compared to some other South Asian and Southeast Asian countries such as India, Bangladesh, Nepal, and Myanmar (Rostami et al., 2020). In addition, parasitic zoonoses like giardiasis (Galgamuwa et al., 2016), cryptosporidiosis (Sirisena et al., 2014), toxocariasis (Iddawela et al., 2003), and bertielliasis (Amarasinghe et al., 2020; Morawakkorala et al., 2006; Karunaweera et al., 2001) were predominantly reported among children, likely due to poor hygiene practices and/or accidental ingestion of contaminated food or soil. Sri Lanka has successfully controlled lymphatic filariasis caused by Wuchereria bancrofti, a WHO-declared neglected tropical disease, through mass drug administrations and stringent control measures (Epidemiology Unit, 2022). However, the emergence of subperiodic brugian filariasis in humans poses a new threat to the lymphatic filariasis control program. Dogs and cats are the main suspected reservoir animals for subperiodic brugian filariasis in Sri Lanka, necessitating further studies in collaboration with local, regional, and national levels.
During the study period, no report of fungal zoonoses among people in Sri Lanka was found. Furthermore, notifiable diseases of animal origin such as tuberculosis, babesiosis, Middle East respiratory syndrome, plague, Ebola, and the Nipah virus were not reported in Sri Lanka. However, zoonotic tuberculosis, the Nipah virus, and babesiosis have been reported in neighboring India, although outbreaks of Ebola and the Middle East respiratory syndrome were not reported (Chattu et al., 2018; Bapat et al., 2017).
Our analysis indicated that Colombo, the main commercial hub of Sri Lanka, reported the highest number of zoonoses compared to other parts of the country. Plausible factors contributing to this include poor hygiene practices, lack of individual water connections, inadequate wastewater disposal in slum settlements, the presence of stray dogs and cats, and an uncontrolled rodent population in the Colombo district (Madubhashini and Dayawansa, 2017). In addition, many studies in our review included patient populations from the Colombo district, leading to more reports on zoonoses in Colombo compared to other districts in Sri Lanka.
Practical strategies for detecting and responding to anticipated or unexpected zoonotic threats are necessary. The “One Health” approach offers a framework to address complex health threats, integrating human, animal, and environmental health. Sri Lanka has successfully used the “One Health” approach to reduce the burden of leptospirosis and rabies (Acharya et al., 2021; Epidemiology Unit, 2014). However, cost-effectiveness, surveillance strategies, laboratory facilities, and workforce requirements may pose challenges when implementing the One Health concept (Dahal et al., 2017). A more practical and generalized five-step One Health framework has been introduced for zoonotic disease control at the local or international level, encompassing engagement, assessment, planning, implementation, and monitoring and evaluation (Ghai et al., 2022). Sri Lanka, as a developing country, has effectively combated various neglected tropical diseases such as rabies, Japanese encephalitis, lymphatic filariasis, and malaria. Nevertheless, Sri Lanka requires a customized, country-specific “One Health” approach considering the factors vector surveillance, risk analysis, and efficient surveillance system to capture zoonotic diseases in domestic and wild animals, collaboration among human, animal, and environmental health sectors, strengthening laboratory capacities, awareness campaigns, and legal framework for rapid outbreak response and containment to effectively control and eliminate zoonoses in Sri Lanka.
Conclusions
Based on the systematic review, Sri Lanka can be categorized as a country with a moderate risk of zoonotic disease transmission. Over the study period (2000–2022), 14 parasitic, 7 bacterial, and 7 viral zoonoses have been reported in Sri Lanka. Leptospirosis emerged as the most reported zoonotic disease in the country. Notably, some zoonoses such as babesiosis, Middle East respiratory syndrome, plague, Ebola, Nipah virus, and Zika virus were not reported in Sri Lanka during this period.
Challenges such as tropical climate-induced flooding, occupational exposure, animal reservoirs/carriers, wildlife interactions, poverty, misdiagnosis, lack of awareness, and information gaps contribute to the burden of zoonoses in Sri Lanka. A customized and country-specific approach is needed to mitigate this burden, focusing on surveillance, early detection, and appropriate control measures. The “One Health” approach, which balances the health of humans, animals, and the environment, is recommended as a framework to address emerging and re-emerging zoonotic diseases in Sri Lanka.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This work was not supported by a grant.