
Abstract
Background:
Rickettsial diseases were reported from Kashmir, India, in the early 20th century. Since then, limited research was carried that has resulted in a significant gap in understanding these diseases. This study was conducted to find out the prevalence and diversity of rickettsial diseases in this region.
Methods:
Blood sample from 476 patients were collected. Enzyme-linked immunosorbent assay was done for the detection of IgM and IgG, and immunofluorescence assay was done for endpoint titer determination. Nested polymerase chain reaction was performed for detection of spotted fever group (gltA, sca0, sca5 genes), typhus group (17 kDa gene) scrub typhus group (47 and 56 kDa gene), followed by sequencing and phylogenetic analysis.
Results:
The seropositivity of scrub typhus, spotted fever group, typhus group was 74 (15.54%), 71 (14.91%), and 60 (12.60%), respectively. Scrub typhus was significantly associated with the urban population (odds ratio = 1.812, 95% confidence interval 1.099–3.0, p = 0.02). Bimodal seasonal variation was observed in all the three groups. In spotted fever group, out of 48 samples 81.25%, 45.83%, and 38.09% were positive for gltA, sca0, and sca5 genes, respectively, and in typhus group 20.83% were positive for 17 kDa. In the scrub typhus group, out of 62 samples, the 56 kDa gene was positive in 56.45%, while the 47 kDa gene was positive in 35.48%. Phylogenetic analysis revealed Rickettsia conorii, Rickettsia parkeri, Rickettsia typhi, and Orientia tsutsugamushi.
Conclusions:
This study confirms the presence of human rickettsial infections in Kashmir, highlighting the need for including rickettsial diseases in diagnostic algorithm for acute febrile illness.
Introduction
The prevalence of rickettsial infections displays remarkable geographical heterogeneity, influenced by a complex interplay of ecological, climatic, and sociodemographic factors (Tabor et al., 2018). Among the diverse spectrum of rickettsial infections, spotted fever, typhus fever, and scrub typhus fever stand out as complex entities, each presenting unique challenges to clinicians and epidemiologists alike.
Spotted fever is caused by various species, resulting in variations in prevalence and species diversity worldwide as different regions harbor distinct species of ticks and their associated pathogens (Ribeiro et al., 2021). The Rickettsia conorii complex consists of Mediterranean spotted fever (MSF), Israeli spotted fever, and Indian tick typhus occurring across the Mediterranean basin, Africa, the Middle East, southern Russia, Pakistan, and India. In India, Rickettsia conorii is the most common species reported (Nallan et al., 2023). However, recent studies also suggest the occurrence of other species like Rickettsia africae, Candidatus Rickettsia, Rickettsia laoensis (Babu et al., 2023), and Rickettsia felis (Khan et al., 2020).
Typhus fever, comprising both epidemic and endemic forms is caused by Rickettsia prowazekii and Rickettsia typhi, respectively (Kato et al., 2022). Globally, typhus fever was considered a neglected or underrecognized disease with limited data available. However, recently, typhus fever has re-emerged in various parts of the world, because of improved disease recognition (Aita et al., 2023).
Scrub typhus fever, caused by Orientia tsutsugamushi was initially thought to be restricted to the “tsutsugamushi triangle,” an area extending from Afghanistan to China and Korea, including the western Pacific, Indian Ocean islands, and northern Australia. However, recent literature suggests the spread of scrub typhus beyond this geographical boundary(Jiang and Richards, 2018).
In Kashmir, India, the first documented cases of epidemic typhus were reported in 1894, and murine typhus and scrub typhus were reported in 1948 (Kalra and Rao, 1949; Kalra and Rao, 1951). From then onwards not much work has been conducted thus creating a significant research gap in understanding these diseases. A recent study from this region indicates a re-emergence of these diseases among the local population, addressing a considerable research gap (Fomda et al., 2023). However, the study’s limitation lay in its sole reliance on the Weil-Felix test, known for its lower sensitivity and specificity, potentially leading to underestimation of the actual disease burden. Therefore, this study was designed to determine the burden of rickettsial diseases and the diversity of species in this temperate region of India using more sensitive and specific methods.
Material and Methods
Study design and participants
This hospital-based prospective study was carried out in the Departments of Microbiology, Medicine, and Pediatrics at a tertiary care hospital in the Kashmir division of the Union Territory (UT) of Jammu and Kashmir, India. Patients admitted or attending the hospital were included. Children under 12 months and adults over 85 years were excluded. A total of 514 patients, clinically suspected of having rickettsial disease, were investigated after obtaining written informed consent, and for minors, consent was provided by their parents. Thirty-eight were excluded due to incomplete clinical details, thus, a total of 476 participants were included in the study. To determine the sample size, the confidence interval width method was used with a prevalence rate of rickettsial disease in India is 25–30%, the calculated sample size was approximately 450 patients (Mittal et al., 2012). A total of 5 mL blood sample was collected from each patient in both a plain vial and an EDTA vial for serological and molecular testing. The convalescent samples were collected after 2–3 weeks from admitted patients and on hospital follow-up visit for discharged patients wherever possible. The samples were stored at −20°C until tested.
Detecting IgG and IgM antibodies
IgG and IgM enzyme-linked immunosorbent assay (ELISA) kits for the spotted fever and typhus groups (Fuller Labs, USA), and for scrub typhus (InBios International, Inc., USA) were used. The ELISA tests were performed following the manufacturer’s instructions. The cut-off values used were determined as per our previously published study (Fomda et al., 2022).
An immunofluorescence assay (IFA) was performed for the detection of IgG and IgM antibodies as per the manufacturer’s instructions using IFA kits (Fuller Labs, USA). For each group, positive by ELISA, IFA was used to confirm the result and identify different groups of rickettsia. Samples positive by IFA were further diluted to achieve endpoint titer. A bright apple green fluorescence of 2+ intensity was considered positive (Fig. 1).
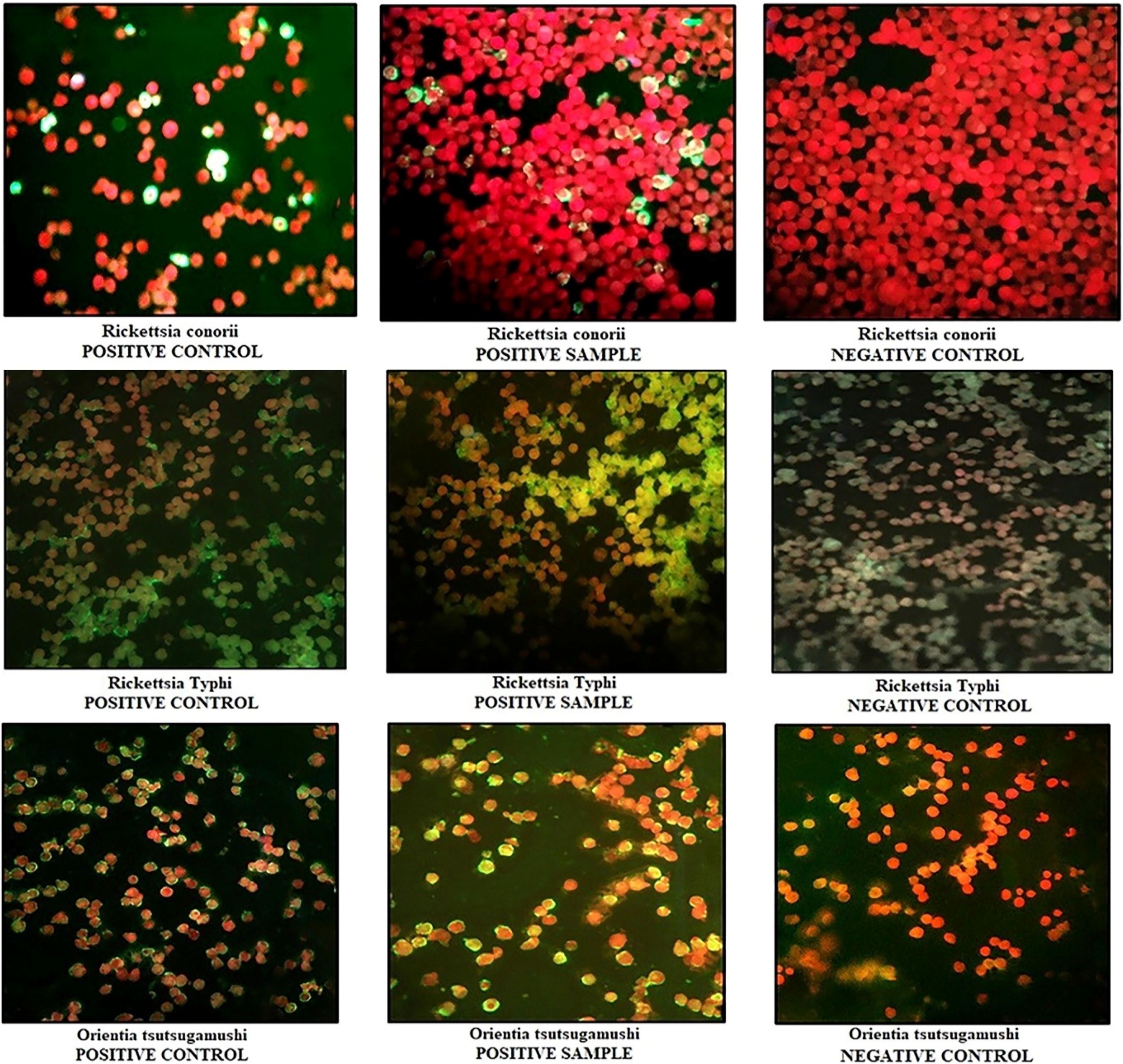
Photomicrograph showing immunofluorescence pattern of controls and samples for different rickettsial groups.
Case definition
Patients were considered positive (acute infection) who were clinically suspected of rickettsial diseases and either IgM/IgG or both (IgM and IgG) positive above the cut-off or fourfold rise in IgG titer between acute and convalescent sera by ELISA.
Nested polymerase chain reaction, DNA sequencing, and phylogenetic analysis
DNA was extracted from whole blood using a QIAmp DNA Blood mini-kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. Nested polymerase chain reaction was performed on the samples that were positive by IFA assay to confirm the species prevalent in this region. For the detection of the spotted fever group (SFG), gltA, sca0, and sca5 were used, for typhus group (TG), 17 kDa protein (htrA) was used and 47 kDa outer membrane protein and 56 kDa type-specific antigen were used for the detection of the scrub typhus group (STG). Each reaction (25 μL) was performed in an automatic thermocycler (Biometra, Analytik Jena, Germany) by adding 2.5 μL of 10× PCR buffer (NH4)2SO4, 1.5 mM of MgCl2, 0.2 mM of dNTPs mix, 1.5U of DNA polymerase (3B BlackBio Biotech, India), 0.2 μM of each primer (Supplementary Table S1 and S2) and nuclease free water. Template volume was adjusted according to the concentration of DNA. Amplified PCR products were run on the 2% agarose gel (Supplementary Fig. S1) and PCR products of the desired size were purified using FavorPrep™ GEL/PCR Purification Kit (FAVORGEN BIOTECH CORP. Taiwan). R. conorii was used as a positive control for SFG and R. typhi for TG (obtained from Naval Medical Research Center, USA) and positive control for O. tsutsugamushi was obtained from Department of Microbiology, Post Graduate Institute of Medical Education and Research, Chandigarh, India. For each run reaction mix without a DNA template was used as a negative control to validate the PCR run.
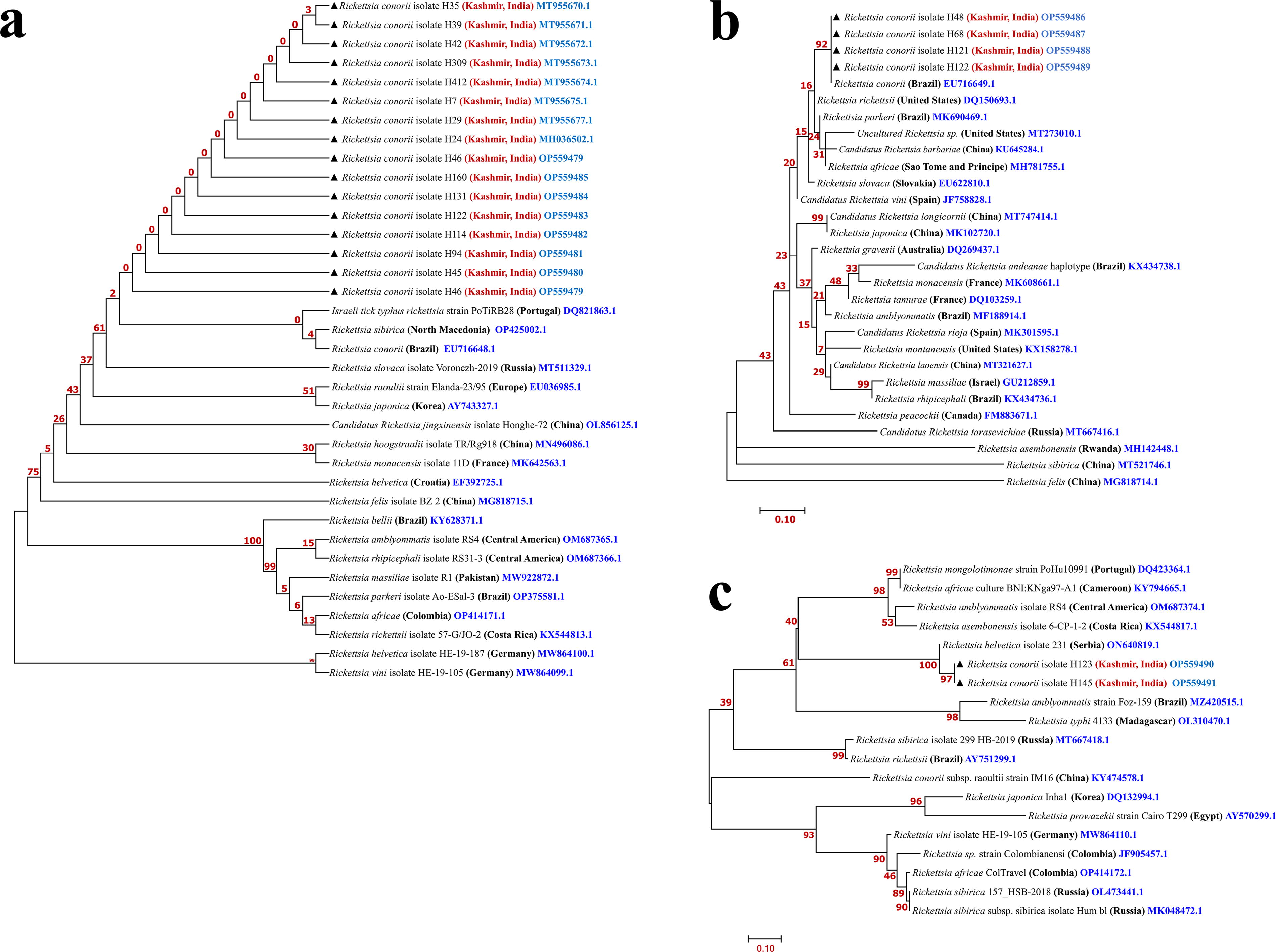
The sequencing of the samples was outsourced to BioKart India Pvt. Ltd. Bengaluru, India. The resulting nucleotide sequences were compared to those archived in GenBank using the Basic Local Alignment Sequence Tool (http://blast.ncbi.nlm.nih.gov/Blast.cgi) and analyzed based on Multiple Locus Sequence Typing criteria. Sequences were aligned using the ClustalW2 program (http://www.ebi.ac.uk/Tools/msa/clustalw2/). Upon consideration of appropriateness, the sequences were submitted to the National Center for Biotechnology Information GenBank. A phylogenetic tree was built using MEGA version 11. The evolutionary tree was constructed employing the neighbor-joining method, while the evolutionary distance matrix was computed using the Maximum Likelihood method (Figs. 2–4).
Maximum likelihood phylogenetic tree generated from
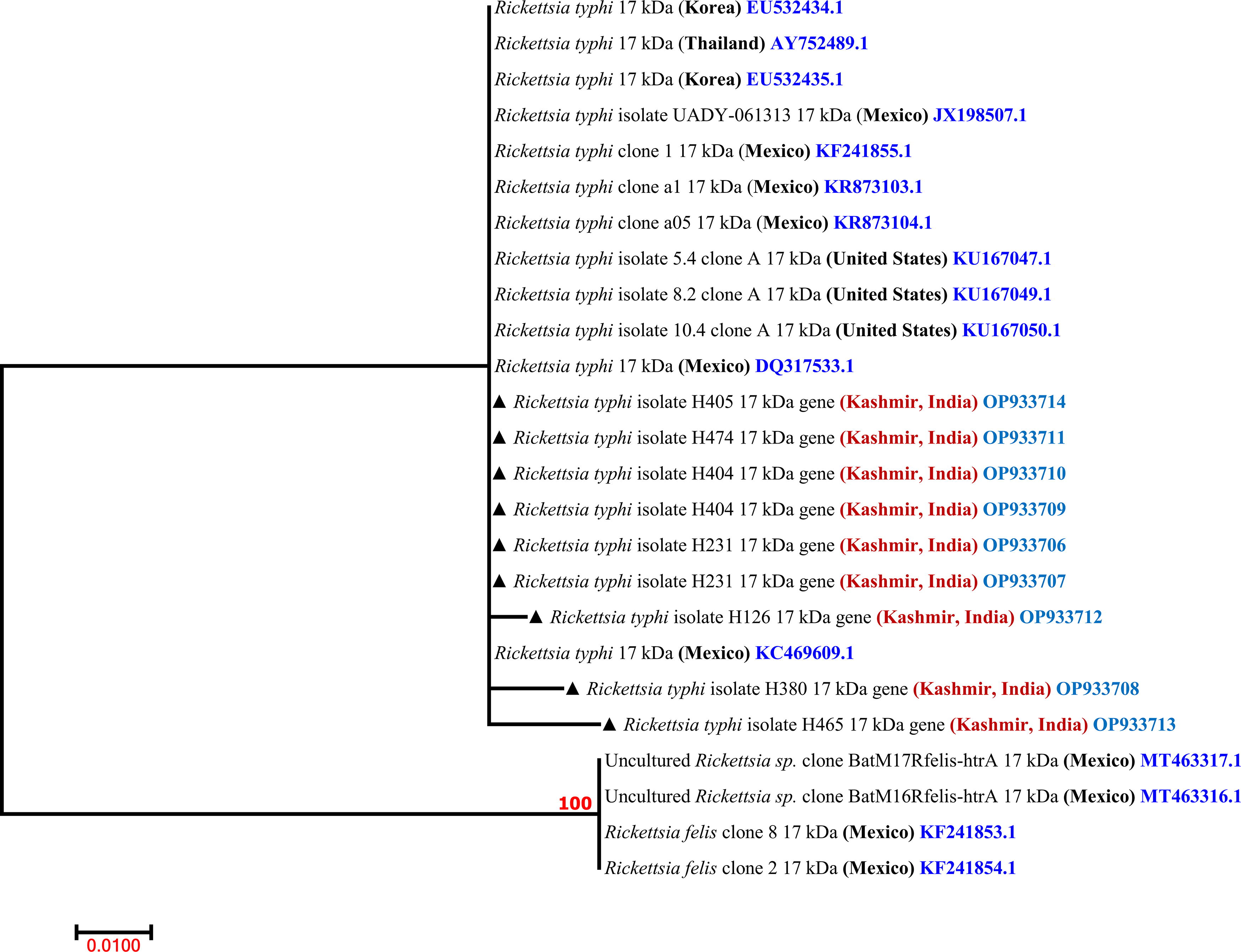
Maximum likelihood phylogenetic tree generated from 17 kDa gene sequences. Sequences marked with a black solid triangle (▲) indicate the sequences obtained in this study.
Maximum likelihood phylogenetic tree generated from
Statistical analysis
The data were analyzed utilizing IBM SPSS Statistics for Windows, Version 26.0, by IBM Corp. in Armonk, NY. The association between risk variables and rickettsial infection was assessed using either a chi-square test or Fisher’s exact (two-tailed) test. The magnitude of the association between risk factors and rickettsial infection was quantified using odds ratios (OR).
Results
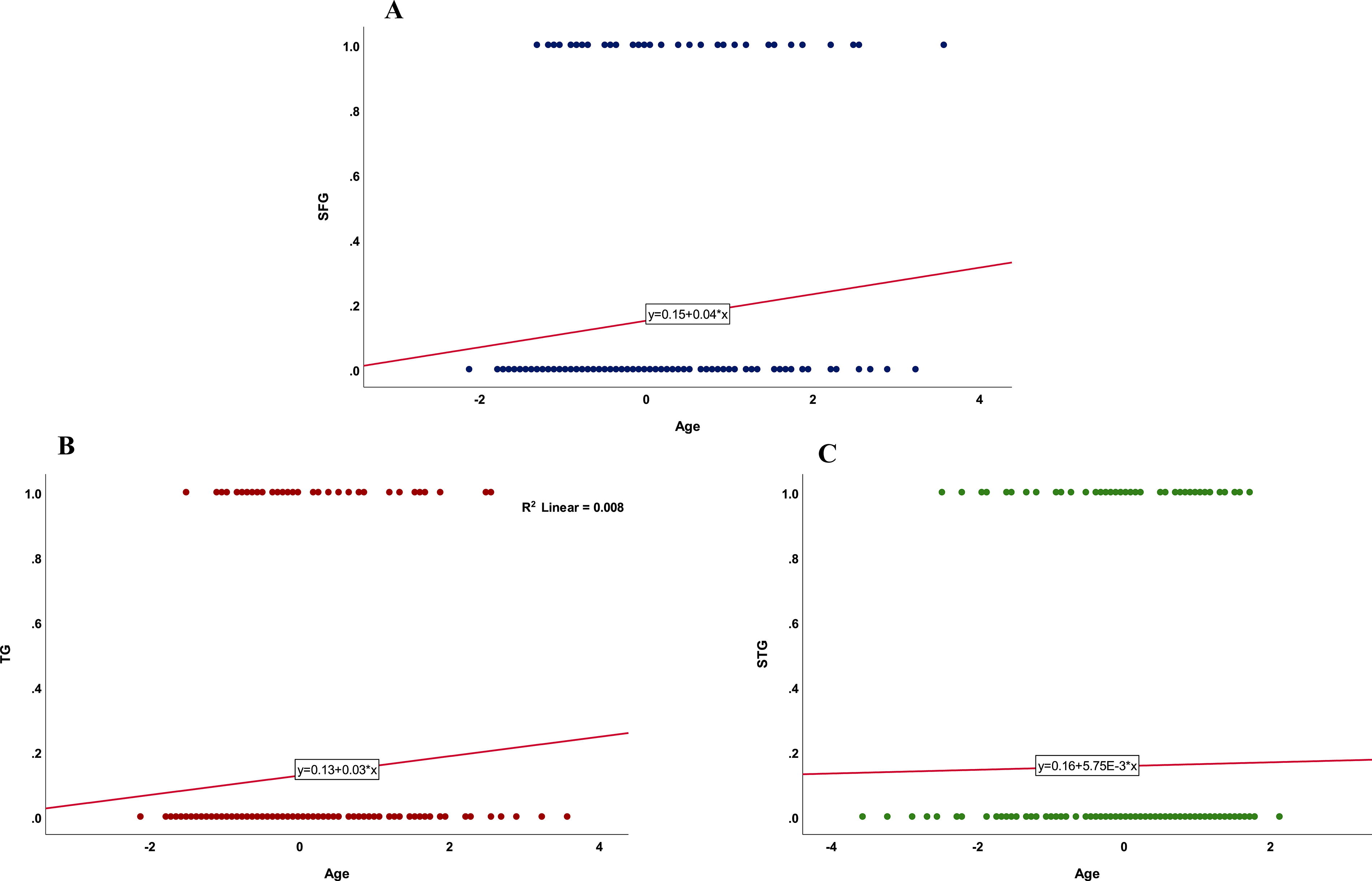
Demographic characteristics are mentioned in Table 1. The median age of patients was 30 years (interquartile range = 21–40) and ranged from 1 to 85 years. The mean age ± standard deviation was 32.33 ± 14.75. The demographic factors like age and gender did not show any significant association with the seropositivity of SFG, TG, and STG, however, an increasing trend was observed with increase in age. Further analysis using binary logistic regression model, revealed that seropositivity of SFG significantly increased with increase in patient’s age (p = 0.013) (95% confidence interval [CI] 0.0043–0.0367), but the association between the TG seropositivity and increasing age showed borderline significance (p = 0.051) (95% CI −0.0001 to 0.0346), however, there was no significant association between the increase in age and seropositivity of STG (p = 0.73) (95% CI −0.0200 to 0.0140) (Fig. 5). The residents living in the urban areas had 1.812 (p = 0.019) times higher odds for scrub infection as compared to the residents living in rural areas. Scrub typhus showed maximum seropositivity 74 (15.54%), followed by spotted fever group 71 (14.91%) and typhus group 60 (12.60%). However, there was no statistically significant difference in the prevalence of the three groups. Cross-reactions were observed among different groups. The highest cross-reaction was observed between SFG and STG (IgM) in nine samples, while the lowest was observed between SFG, TG, and STG (IgG, IgM) in one sample (Supplementary Table S3). The results of the endpoint titer for the IFA-positive samples are shown in Supplementary Table S4. Differentiation into different groups based on higher IFA titter is shown in Supplementary Table S5. Within the SFG and TG out of 48 samples tested, 39 (81.25%), 22 (45.83%), and 16 (38.09%) were positive for gltA, sca0, and sca5 genes, respectively, and 10 samples (20.83%) were positive by 17 kDa (TG). In the STG, out of 62 samples, 35 (56.45%) and 22 (35.48%) were positive for 56 kDa and 47 kDa genes, respectively. District-wise distribution of spotted fever, typhus fever, and scrub typhus fever are shown in Supplementary Figure S2. Seasonal variations of spotted fever, typhus fever, and scrub typhus fever are shown in Figure 6. All three groups showed bimodal seasonal variation with a small peak in spring followed by a large peak in summer and autumn.
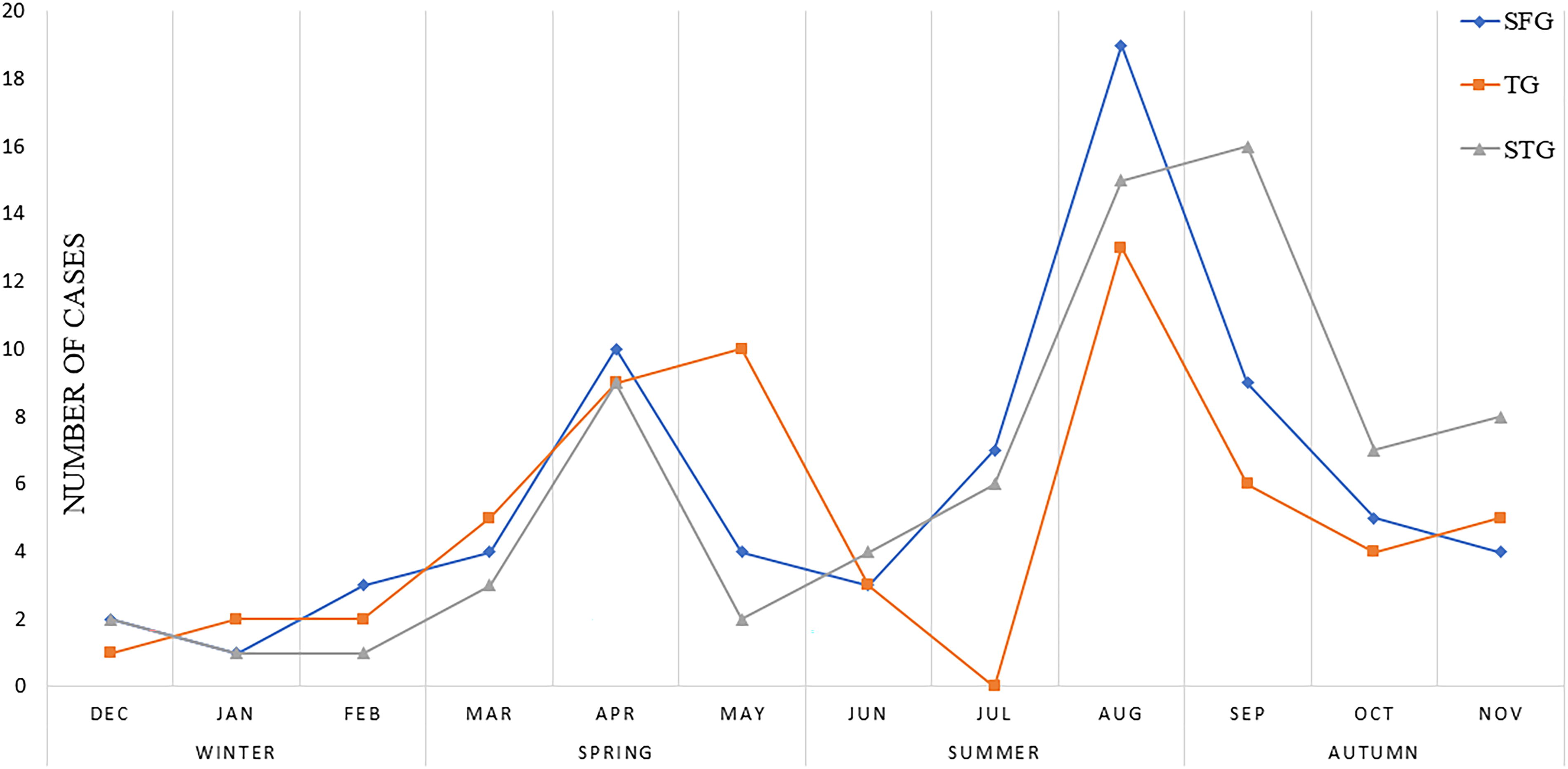
The seasonal variation of different rickettsial groups.
Demographic Characteristic of Patients Enrolled in the Study (n = 476)
Statistically significant.
CI, confidence interval; OR, odds ratio.
Clinical manifestations like a rash (Supplementary Fig. S3), headache, jaundice, myalgias, splenomegaly, conjunctival congestion, skin changes, diarrhea, cough, stroke, shock, and heart failure showed no statistically significant association, however, vomiting was significantly associated with typhus fever (OR = 2.135, p = 0.007) (Table 2). Elevated liver enzymes, ALT (>45 U/L), and ALP (>141 U/L) were most commonly observed in the TG group, LDH levels (>248U/L) were highest in the SFG group (24.32%), followed by the TG group (20%) and the STG group (18.31%). Elevated creatinine phosphokinase (CPK) (>195 U/L) was predominantly seen in the TG group (26.67%) (Table 3). Among hematological findings, low hemoglobin (<13 g/dL) was most commonly observed in the TG group (53.33%), followed by the SFG (45.07%) and STG (37.84%) groups. The prevalence of leucocytosis (>10,000/μL) thrombocytopenia and hyponatremia was also common across all three groups (Table 3).
Clinical Manifestations of the Patients with Rickettsial Diseases (n = 476)
Statistically significant.
Laboratory Parameters Among the Three Rickettsial Groups
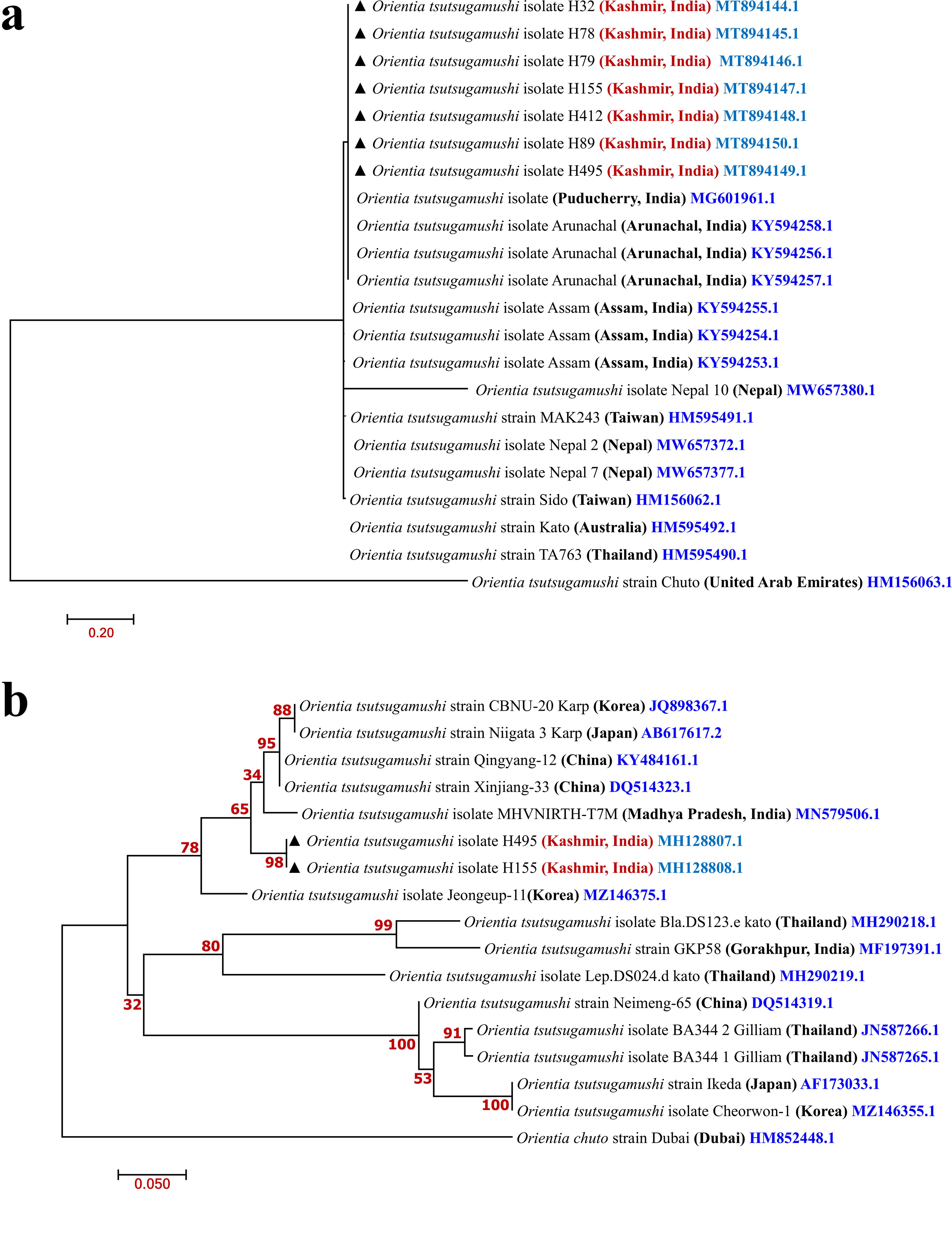
Out of 39 gltA-positive, 14 were sequenced; for sca0, 4 out of 22 were sequenced; and for sca5, only 2 out of 16 PCR-positive samples were sequenced. Phylogenetic analysis based on the sequences gltA and sca0 revealed R. conorii (accession numbers: MT955677.1, MT955676.1, MT955675.1, MT955674.1, MT955673.1, MT955672.1, MT955671.1, MT955670.1, OP559485.1, OP559484.1, OP559483.1, OP559482.1, OP559481.1, OP559480.1 and OP559486, OP559487, OP559488, OP559489), respectively, which displayed 100% similarity with each other. The sequencing of the sca5 gene in two samples revealed the presence of Rickettsia parkeri (OP559490 and OP559491). Out of 10 PCR-positive samples for the 17 kDa gene, 8 were sequenced, revealing the presence of R. typhi (accession numbers OP933714.1, OP933707.1, OP933706.1, OP933712.1, OP933710.1, OP933709.1, OP933713.1, and OP933708.1). Out of 22 PCR-positive samples for the 47 kDa gene, 7 were sequenced, and out of 35 PCR-positive samples for the 56 kDa gene, 2 were sequenced. The sequencing analysis of the 47 and 56 kDa genes confirmed the presence of O. tsutsugamushi (accession numbers: MT894144.1, MT894145.1, MT894146.1, MT894147.1, MT894148.1, MT894149.1, MT894150.1) for the 47 kDa gene and (MH128808.1, MH128807.1) for the 56 kDa gene, respectively.
Treatment outcomes of 111 IFA-positive patients were available. Out of 111 patients, 57 received rickettsial treatment (doxycycline and/or azithromycin) and 54 patients received nonrickettsial treatment. Two patients, one from the STG group and one from the TG group, died who have not received antirickettsial treatment.
Discussion
The present study demonstrates the existence of all three groups of rickettsial infections with scrub typhus being the commonest followed by SFG and TG in this region. This is consistent with the findings reported previously (Khan et al., 2016; Devamani et al., 2020). Most of the studies from India have been done on scrub typhus (Devasagayam et al., 2021) with limited data available on the prevalence of spotted and typhus fever (Krishnamoorthi et al., 2023). Methods for diagnosing rickettsial diseases vary, with some studies emphasizing on the detection of antibodies using different serological techniques (Damodar et al., 2023). While IFA is a gold standard serological test, its utilization is limited in resource-poor settings due to factors such as high cost, the requirement for an immunofluorescent microscope, and the need for technical expertise. ELISA was used in this study as it is a highly sensitive and specific technique and it is better suited to resource-poor settings due to its low cost, ability for batch testing, and reduced need for technical expertise (Stewart and Stewart, 2021). IFA was used to differentiate into different groups (SFG, TG, and STG), if the group demonstrated fourfold higher dilution compared with other groups, as described previously (Paris and Dumler, 2016). Cross-reactions were observed between different groups, which may occur because of the left-over antibodies from the previous exposures, however, in the present study, we have established an endemic cutoff for each group and the samples were considered positive only above that cutoff value. Thus, eliminating the possibility of cross-reaction with previously leftover antibodies.
There was no statistically significant difference in the prevalence of spotted fever and typhus groups between rural and urban areas. The spotted fever group is commonly reported in rural areas particularly peri-forested areas (Devamani et al., 2020). The expanding population in urban areas needs more land for use which is generally acquired by extending into rural areas by deforestation thus facilitating human vector interaction. Some studies suggest no significant difference between urban and rural areas probably reflects similar environmental conditions (Tshokey et al., 2017). Typhus group though predominantly occurs in urban areas, however, an association of R. typhi with rural residents and farming has been reported (Bolaños-Rivero et al., 2011).
The seropositivity of scrub typhus reported in the present study was high in urban areas as compared to rural areas and the difference was statistically significant. Most studies suggest scrub typhus to be more prevalent in rural areas than in urban areas (Devamani et al., 2020). Contrary to its predominant rural distribution some studies suggest the occurrence of scrub typhus in metropolitan areas (Vallee et al., 2010).
In the present study, no statistically significant difference was observed between seroprevalence in hilly and plain areas. A study conducted in south India has shown a higher prevalence of spotted fever in hilly villages compared to urban and rural plain areas (Devamani et al., 2020). The possible explanation for no difference in hilly and plain areas in the present study may be the low temperature in hilly areas as compared to plain areas. As the latitude decreases the incidence of rickettsial disease increases, as has been reported previously (Jeung et al., 2016).
Rickettsial diseases have historically been associated with higher rates in men and those of old age, however, some investigations have reported predominantly in female subjects (Roopa et al., 2015; Zhang et al., 2019). However, no significant difference was noted between gender for susceptibility to rickettsial infections, which is consistent with similar observations in a recent study (Abdad et al., 2018). In the present study, significant association was observed between the SFG seropositivity and increasing age of the study population, which is in line with a previous study (Thiga et al., 2015), however, no significant association was observed between TG, STG seropositivity, and increasing age, as reported previously (Abdad et al., 2018). Numerous studies indicate that children are equally susceptible to infection, yet the diagnosis is often overlooked (Marshall, 2000). In contrast, few investigators revealed that scrub typhus was predominant in old age but for murine typhus and spotted fever old age was not a risk factor (Devamani et al., 2020). The gender-wise variation depends on the involvement of a particular gender in farming activity in the majority of places it is the male gender who is involved in such activity. The probable reason for no significant difference in the present study may be that females are equally involved in farming activities, particularly in rural areas. The majority of households in Kashmir have kitchen gardens and invariably females work in these gardens. Regarding district-wise distribution, it is important to note that this hospital-based study may have overrepresented patients from certain districts due to their proximity to the hospital, rather than solely reflecting the risk of rickettsial diseases in those areas.
The seasonal distribution corresponds to the rainy season in Kashmir, which facilitates the proliferation of vectors along with ample food in the harvesting season and may be conducive for vectors, similar observations were made in another study (Kinoshita et al., 2021). Some studies have reported no clear seasonality (Nadjm et al., 2014). Understanding these seasonal patterns is vital for implementing preventive measures effectively.
The clinical manifestations reported in the present study are in concurrence with previous findings (van Eekeren et al., 2018). Some studies have noted a higher incidence of rash, while others observed a low percentage of rash in SFG and STG (Stewart et al., 2020). Whether a skin rash is present or absent does not have a significant impact on establishing the diagnosis of rickettsial disease, which has been reported previously (van Eekeren et al., 2018). The rash typically appears early in scrub typhus and usually lasts for a brief duration (Berman and Kundin, 1973). This could potentially contribute to the lower reported percentage, as patients might seek medical attention after the rash has disappeared (Gasem et al., 2009). Lymphadenopathy was observed mostly in TG compared with SFG and STG, this is contrary to the low frequency of lymphadenopathy in TG reported in another study (Fan et al., 1987). In contrast, lymphadenopathy is frequently cited as a well-known clinical sign of scrub typhus in various studies (Phongmany et al., 2006). This distinction highlights the differing clinical presentations of these rickettsial diseases, underscoring the importance of careful differential diagnosis in patients presenting with fever and lymphadenopathy.
Eschar was not a common finding in our study, as it was observed in only a single patient. The possible reason for the low presence of eschar could be the strains present in this region, the immunity in the local population, and late presentation as the eschar may be observed in the early stages of the disease and may be missed if not looked at properly. Furthermore, it is worth mentioning that STG cannot be excluded in the absence of eschar (van Eekeren et al., 2018).
Elevated ALT and CPK levels in STG and TG, respectively, in the present study are consistent with findings reported earlier (Phongmany et al., 2006). Leucocytosis, thrombocytopenia, and hyponatremia were common findings among all three groups which is consistent with previous studies (Abdad et al., 2018).
Although the treatment of rickettsial disease is the same throughout the three groups, species differentiation by molecular methods is important as the risk of exposure, vectors, and prevention aspects are different and need consideration. Phylogenetic analysis of gltA and sca0 genes identified R. conorii as the predominant species. The pairwise nucleotide sequence identity and the phylogenetic tree constructed based on the gltA sequences indicated a 100% similarity to several strains of Rickettsia conorii, including M102, M198, M167, and M158 from Chandigarh, India, Crimea-2016–1, subsp. conorii isolate Crimea-2019H from Crimea, PoAnR3dt, and Malish 7 (accession numbers: MN497613.1, MN497615.1, MN497611.1, MN497614.1, KY640399.1, OQ184719.1, EF177486.1, AE006914.1, respectively). Additionally, a 99.69% identification was observed with strains, Xinjiang-PS from China (accession number: MF002509.1).
In our study, Partial sca5 Sanger gene sequencing revealed two cases of R. parkeri, which showed similarities with R. parkeri (KY124259.1) from the United States; and Rickettsia slovaca (OR148325.1) from Russia. Similarity was also found with unclassified Rickettsia spp. (OM908388.1 and PP373674.1) from Uttar Pradesh and Bhubaneswar, Odisha, India, respectively (Behera et al., 2023).
Emerging data suggest that R. parkeri infections may extend beyond the traditional range of Amblyomma maculatum, with cases being described in southern Arizona (Herrick et al., 2016). Although documented infections are uncommon, misdiagnosis is possible due to the limited use of advanced identification techniques. Our study is the first from India to report the strain phylogenetically related to R. parkeri, however, undifferentiated rickettsial species have been reported from India, which showed similarity to its sequences (Behera et al., 2023). Further studies are required to confirm this finding and the distribution of its vector in this region.
Sequencing of the 17 kDa gene revealed the presence of R. typhi in all samples, which exhibited 100% identity with R. typhi (KC469609.1), R. typhi strain Wilmington (AE017197.1), DQ317533.1, and AY867871.1. A study from Mexico identified R. typhi through 17 kDa-based gene sequencing (JX198507), which also showed 100% identity with the R. typhi strain Wilmington (Zavala-Castro et al., 2014). Globally, typhus fever was considered a neglected or underrecognized disease with limited data available. However, recently, typhus fever has re-emerged in various parts of the world, because of improved disease recognition (Aita et al., 2023). From the Indian perspective, only seroprevalence-based studies are available (Mane et al., 2019; Vanramliana et al., 2023). Our study is the first discerption of typhus group from India using reliable diagnostic methods.
The sequencing of the 56 kDa gene revealed O. tsutsugamushi, showing an identity of 100% with OT/AIIMS/3379/2020 (accession number: ON087061.1) from Delhi, India. Kumar et al. documented that the majority of strains were Karp-like, followed by Gilliam-like strains, with a smaller proportion resembling Hualien1 or S072 in their study (Kumar et al., 2019). Moreover, O. tsutsugamushi was the sole species identified through 47 kDa gene sequencing. These sequences exhibited close identity of 96.08% with strains such as Karp (LS398548.1), Kato (LS398550.1), Gilliam (LS398551.1), RLD14433/16 (KY594257.1), RAN14813/16 (KY594256.1) from Arunachal Pradesh, India, RTN14435/16 (KY594255.1), and RNL14563/16 (KY594254.1) from Assam, India. The majority of the strains identified in our study showed similarities with Karp and Kato types. Kato-like strains were the most common, particularly prevalent in the South and Northeast of India, followed by Karp-like strains (Varghese et al., 2015). Kawasaki-type strains have been documented in the southern regions of the country, as reported by Usha et al. They also identified cases of dual infection involving both Karp and Kawasaki types in a subset of patients (Usha et al., 2016). Less frequently occurring variants, like Ikeda-like strains, have also been documented in India (Varghese et al., 2015) The diversity of O. tsutsugamushi strains across a vast geographical distribution of North India has significant implications for both diagnostic assay development and vaccine production for scrub typhus.
Early symptoms of rickettsial diseases resemble other febrile illnesses, leading to serious outcomes due to delayed diagnosis and treatment. Nonetheless, they remain susceptible to doxycycline which is the recommended treatment irrespective of age, but if a patient with rickettsial infection doesn’t respond within 48 h of starting proper antirickettsial therapy, a different diagnosis should be considered (Biggs et al., 2016). Only half of the diagnosed patients were given the right treatment and half of those prescribed antibiotics got a medication with no antirickettsial activity. The mortality rate in this study was low, which is in line with the findings of previous studies (Binder and Armstrong, 2021). There aren’t any other treatments as effective as doxycycline for preventing severe outcomes and death however, a recent study shows that combination therapy with intravenous doxycycline and azithromycin proved to be more effective in treating severe scrub typhus compared to monotherapy with either drug alone (Varghese et al., 2023), and using antibiotics other than the recommended treatment indicates lack of knowledge about the rickettsial diseases in this region.
Conclusion
Rickettsial diseases, including spotted fever group, typhus group, and scrub typhus group, are prevalent in this subtropical region, with higher incidence rates observed during spring, summer, and early autumn, underline the public health significance of these diseases in the studied regions. Moreover, phylogenetic analysis revealed the presence of species like Rickettsia conorii, Rickettsia parkeri, Rickettsia typhi, and O. tsutsugamushi (Karp and Kato-like). This study highlights the need for enhanced surveillance, and awareness of clinicians to include rickettsial diseases in diagnostic algorithms for acute febrile illness, thus increasing the likelihood of early identification and timely treatment of affected patients, ultimately leading to better clinical outcomes.
Footnotes
Acknowledgments
The authors acknowledge the Department of Health Research (DHR) Govt. of India, for funding this project. The author also thanks all the patients for their cooperation during sample collection and for giving detailed informed consent. Authors also extend their gratitude to Dr. Chao Chien-Chung, Naval Medical Research Center (NMRC), Silver Spring, MD, USA, for providing PCR-positive controls.
Authors’ Contributions
B.A.F.: Conceptualization, writing, original draft, review and editing, project administration, supervision, validation, and funding acquisition. N.A.: Investigation. Y.B.M.: Formal analysis and investigation. S.M.Q.: Resources. M.N.: Writing—original draft and software. M.A.B.: Resources. S.S.: Resources.
Ethical Statement
The authors affirm that all procedures involved in this study adhere to the ethical standards outlined by the Indian Council of Medical Research guidelines on human experimentation, as per the Helsinki Declaration of 1975, revised in 2013, and approval was obtained from the ethical clearance committee of the Sher-i-Kashmir Institute of Medical Sciences (SKIMS131/IEC-SKIMS/2013–6639).
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This work was supported by the Department of Health Research (DHR) Govt. of India (Grant No. GIA/33/2014-DHR), sanctioned to Dr. Bashir Ahmad Fomda.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.