
Abstract
Background:
In the study, we aimed to determine the prevalence rate of hyponatremia in patients with Crimean-Congo hemorrhagic fever (CCHF) and to investigate the relationship between hyponatremia and disease severity.
Materials and Methods:
Patients over 18 years of age who received a definitive diagnosis of CCHF between April 2018 and October 2023 were included in the study. The patients’ sodium levels, symptoms, and findings at the time of admission to the hospital were recorded. In addition, the severity score index was calculated according to the laboratory values and findings at the time of admission.
Results:
The total number of patients included in the study was 219. Hyponatremia was detected at admission in 99 (45.2%) patients. The median serum sodium value in patients with hyponatremia was 133 (127–135) mEq/L. Spearman correlation analysis revealed a statistically significant inverse correlation between serum sodium level and severity score index (r = −0.522, p < 0.001).
Conclusions:
Mild hyponatremia was detected in almost half of the patients with CCHF, and this parameter may be useful in determining disease severity on admission.
Introduction
Crimean-Congo hemorrhagic fever (CCHF) disease is a vector-borne zoonotic disease. It was isolated for the first time in the world in Congo in 1956. The first case in Turkey was seen in the Kelkit Valley in 2002. To date, cases have been reported from more than 30 countries. Mortality rates vary by country and region, but the average is approximately 10% (Nasirian, 2020).
Hyponatremia is the most common electrolyte disorder seen in various diseases. Hyponatremia, in which inflammation plays an important role, can be seen in many infectious and noninfectious diseases (Królicka et al., 2020; Swart et al., 2011). Pneumonia, encephalitis, meningitis, and tuberculosis are classical examples of infectious diseases in which hyponatremia can occur (Królicka et al., 2020). In addition, hyponatremia has been defined as severe acute respiratory distress syndrome due to coronavirus disease 2019 (COVID-19) (Ayus et al., 2021; Habas et al., 2022). Hyponatremia has also been reported in Ebola and dengue fever, which are other viral hemorrhagic fevers (Lumpaopong et al., 2010; van Griensven et al., 2016). Nonosmotic vasopressin (antidiuretic hormone) secretion due to the release of the inflammatory cytokine interleukin-6 (IL-6) causes hyponatremia (Swart et al., 2011). In addition, Dixon et al. found a linear correlation between IL-6 level and hyponatremia (Dixon et al., 2020). In CCHF, IL-6 levels were found to be higher in fatal patients than in nonfatal patients (Ergonul et al., 2006; Ergönül et al., 2017). There is also a study showing that IL-6 level correlates with disease severity (Onuk et al., 2023). However, to our knowledge, there are no studies in the literature that have examined the relationship between hyponatremia and CCHF severity. It is very important to predict mortality and disease severity in CCHF at the time of admission. Our study aimed to determine the prevalence of hyponatremia in patients with CCHF and to investigate the relationship between hyponatremia and disease severity.
Materials and Methods
Study design, settings, and participants
Patients who received a definitive diagnosis of CCHF in the Department of Infectious Diseases and Clinical Microbiology of Tokat State Hospital between April 2018 and October 2023 were included in the study. Patients younger than 18 years of age, patients who did not have a serum sodium result at the time of admission, and patients using antihypertensive, antidepressant, or antiepileptic thiazide drugs were excluded from the study (Fig. 1). The study was approved by the ethics committee of Tokat Gaziosmanpasa University (24-MOBAEK-065). The patients’ sodium levels, symptoms, and findings at the time of admission to the hospital were recorded. The severity score index (SSI) of the patients at the time of admission to the hospital was calculated. The relationship between serum sodium values and SSI at the time of admission was investigated. Patient data were collected retrospectively from the hospital electronic record system.
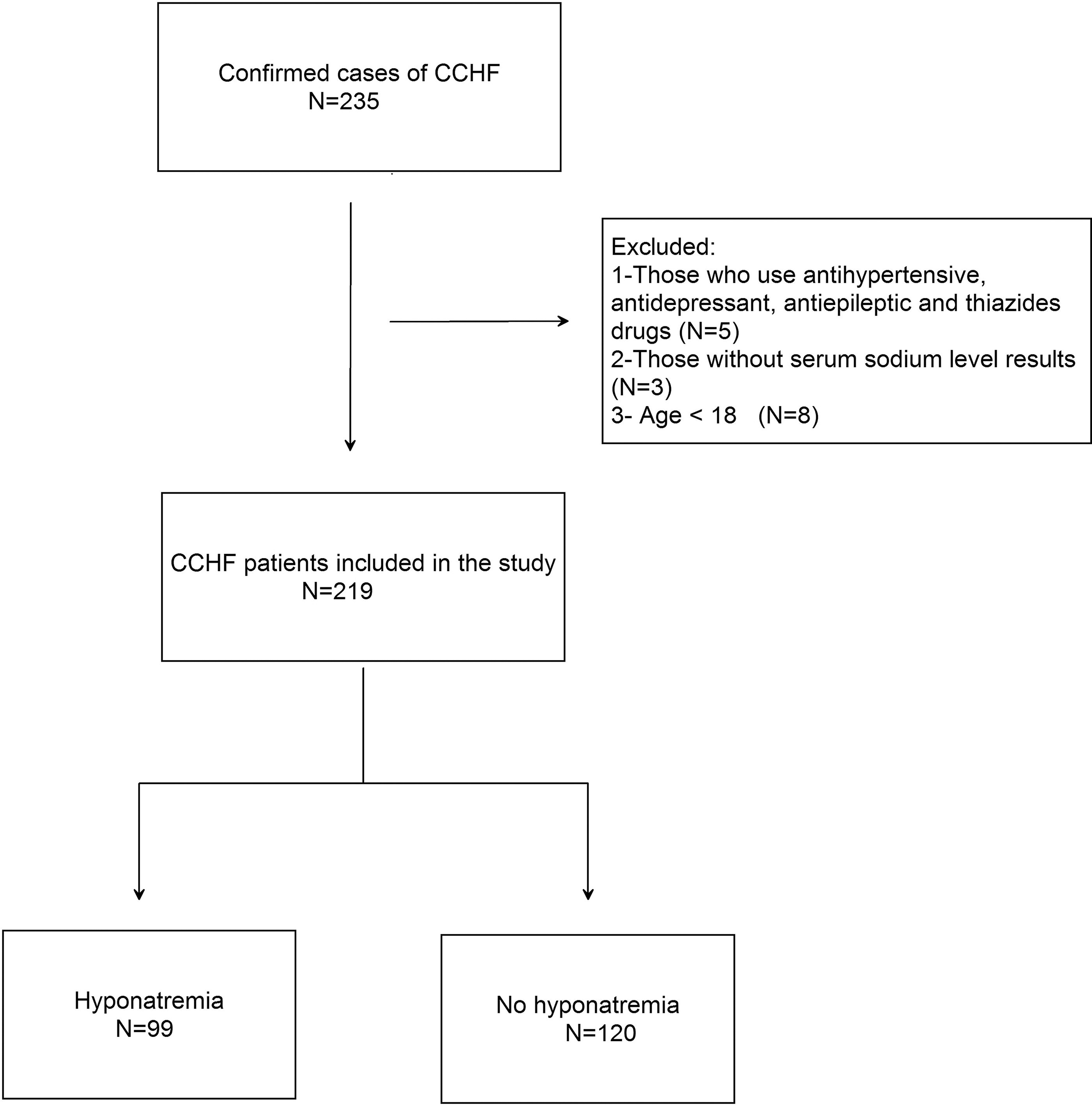
Flowchart in study.
Definitions and microbiological identification
The definitive diagnosis of CCHF was made by agent-specific IgM tests including enzyme-linked immunosorbent assay and/or reverse transcription polymerase chain reaction. Serum sodium levels were quantified using Atellica Solution Immunoassay and Clinical Chemistry Analyzers (Siemens Healthcare Diagnostics, Erlangen, Germany). Patients with serum sodium levels of 135 mEq/L and below were considered to have hyponatremia (Adrogué and Madias, 2000). Patients were classified as having mild hyponatremia if their serum sodium was 130–135 mEq/L, moderate hyponatremia if it was 120–129 mEq/L, and severe hyponatremia if it was <120 mEq/L (Spasovski, 2024). In addition, the SSI was calculated according to laboratory values and findings at the time of admission. The SSI is calculated with five parameters, namely, thrombocyte count (0–3 points), fibrinogen (0–3 points), activated partial thromboplastin time (0–3 points), bleeding (0–3 points), and somnolence (0–1 points). In this scoring system, a score of 0–2 points is classified as mild disease, 3–9 points as moderate disease, and 10–13 points as severe disease (Dokuzoguz et al., 2013).
Data and statistical analysis
Statistical Product and Service Solutions statistics package (version 23.0; Armonk, NY: IBM Corp.) was used for statistical analyses. The evaluation of the normal distribution of continuous variables was conducted using both visual (histogram and probability graphs) and analytical (Shapiro–Wilk test) methods. In cases where continuous variables did not demonstrate a normal distribution, the median (minimum–maximum) value was calculated. Numbers and percentages were calculated for categorical variables. Pearson’s chi-squared test and Fisher’s exact probability test were used to calculate categorical variables. The Mann–Whitney U and Student’s t-tests were employed for the analysis of continuous variables. A Spearman correlation analysis was conducted to assess the strength of the relationship between the variables. The statistical significance level was set at p < 0.05.
Results
In the study, the number of confirmed cases of CCHF between 2018 and 2023 was 235. Sixteen patients were excluded from the study, and the final number of patients included in the study was 219 (Fig. 1). The median (min–max) age of the patients was 54 years (18–87), and 154 (70.3%) were males. The number of patients with a tick bite history was 162 (74%). At the time of admission, the SSI classified 193 patients (88.1%) as having mild disease, 24 patients (10.9%) as having moderate disease, and 2 patients (1%) as having severe disease. The mortality rate observed in the 219 patients included in the study was 3.6% (Table 1).
Demographic Characteristics and Outcomes of the Patients with Crimean-Congo Hemorrhagic Fever
At the time of admission.
Min, minimum; Max, maximum.
In the study, among the patients with CCHF, there were 99 (45.2%) patients with hyponatremia, which was identified at the time of admission. In addition, the median (min–max) serum sodium value of the patients with hyponatremia was 133 (127–135) mEq/L. When the patients with hyponatremia were compared with patients with normal serum sodium levels, the presence of fever was found to be statistically significantly higher in patients with hyponatremia (p < 0.001). The SSI value was found to be statistically significantly higher in patients with hyponatremia (1 [0–10], p < 0.001). Moderate cases were observed to be statistically more frequent in the hyponatremia group compared with the group with a normal serum sodium level (p < 0.001). Mild cases were more common in the group with normal serum sodium levels (Table 2). The Spearman correlation analysis revealed a statistically significant inverse correlation between sodium and the SSI levels (r = −0.522, p < 0.001) (Figs. 2 and 3). In addition, all patients in the hyponatremia group had fever at the time of admission, which was statistically different compared with that of the group with normal serum sodium levels (p < 0.001) (Table 2).
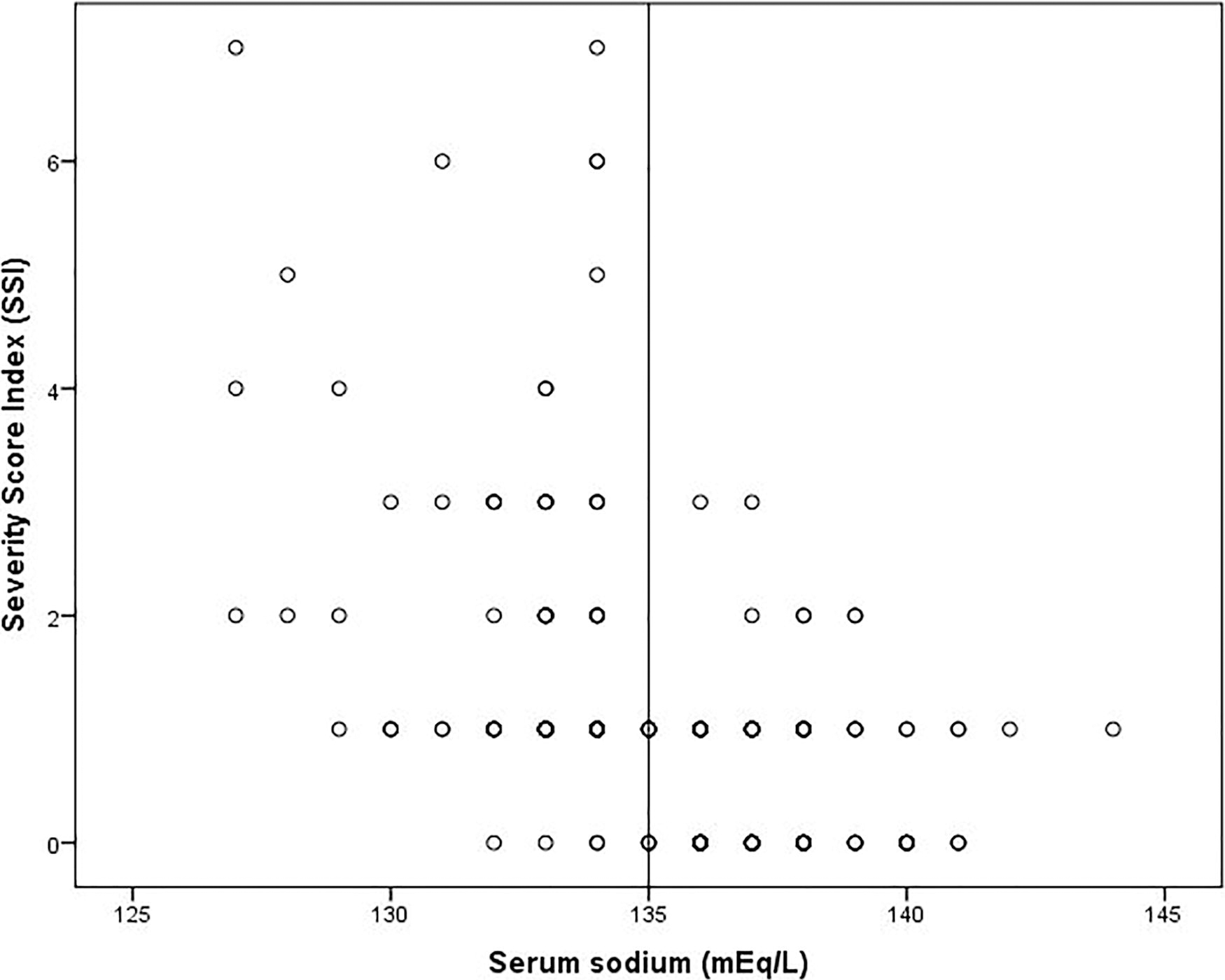
Scatter diagram of serum sodium level with severity score index.
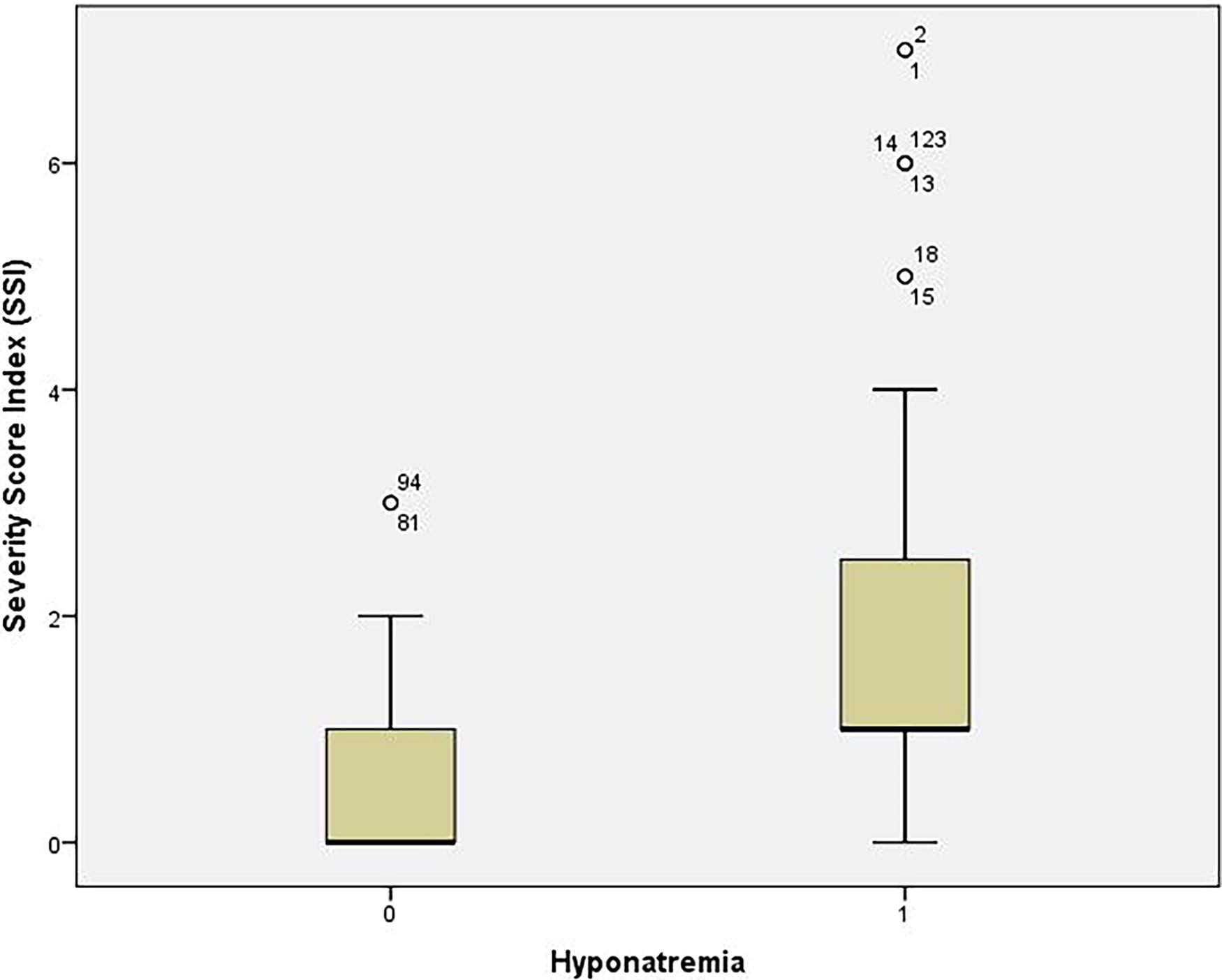
Boxplot of the severity score index according to the presence of hyponatremia (group 0 = 136–145 mEq/L, group 1 ≤ 135 mEq/L, p < 0.001).
Demographic and Clinical Characteristics, Laboratory Values, and Outcomes in Hospitalized Patients with Crimean-Congo Hemorrhagic Fever With and Without Hyponatremia on Admission
Bold data:statistically significant.
The results in the table are presented as n (%) unless stated otherwise.
At the time of admission.
Discussion
This study is a cross-sectional analysis of CCHF patient data over 5 years. To the best of our knowledge, there is no study in the literature on the relationship between CCHF and hyponatremia. Only one case report of hyponatremia with CCHF was reported in the literature (Özer et al., 2014). Hyponatremia occurs due to nonosmotic vasopressin release secondary to inflammation seen in classical infectious diseases, and this study investigates the indirect relationship between hyponatremia and disease severity. Interestingly, hyponatremia was detected in almost half of the patients in our study. This represents the inaugural instance of this phenomenon being documented in the scientific literature. We also found a statistically significant inverse correlation between disease severity at admission and serum sodium levels. In one study, the IL-6 level was associated with disease severity in patients with CCHF (Onuk et al., 2023). In addition, in other studies, IL-6 levels have been found to be statistically significantly higher in the mortal patient group than in the nonmortal patient group (Ergonul et al., 2006; Ergönül et al., 2017). It was shown that IL-6 plays a role in nonosmotic vasopressin secretion, resulting in hyponatremia (Swart et al., 2011). In another study, a linear relationship was found between IL-6 and hyponatremia (Dixon et al., 2020). In conclusion, the increase of IL-6, a proinflammatory cytokine, is associated with both CCHF disease severity and hyponatremia (Onuk et al., 2023; Swart et al., 2011). In many centers, the level of IL-6 is not a routinely measured laboratory parameter. Instead, this simple laboratory test (serum sodium value) may be useful indirectly in predicting the severity of the disease in centers with limited laboratory facilities. In addition, fever was found to be significantly higher in the hyponatremia group. It can be explained by the fact that inflammatory cytokines, which play a role in the pathogenesis of fever, cause hyponatremia by causing vasopressin secretion (Son et al., 2020). Other conditions that cause hyponatremia should not be ignored. In our study, we excluded patients using medications that could cause hyponatremia to avoid bias, namely, antihypertensive, antidepressant, antiepileptic, and thiazide drugs. In our study, a correlation was found between hyponatremia and the severity of CCHF. This situation is not unique to CCHF among infectious diseases. There are studies in the literature reporting that hyponatremia is associated with the severity of disease in various infectious diseases. For example, studies reporting that hyponatremia is associated with the severity of disease in pneumonia, human immunodeficiency virus infection, tick-borne encephalitis, and urinary tract infections have been reported (Braconnier et al., 2017; Królicka et al., 2020; Liang et al., 2024; Skudal et al., 2024). It has been reported that the inflammation-induced nonosmotic antidiuretic hormone release mechanism that we mentioned in the pathogenesis may also play a role in other infections seen with hyponatremia (e.g., COVID-19) (Frontera et al., 2020).
The present study is limited by its retrospective, single-center design and relatively small sample size. Furthermore, the limited number of deceased patients precluded an investigation into the potential impact of hyponatremia on mortality prediction. The strengths of the study are that it is the first study on hyponatremia in CCHF. It contains a 5-year data set. In addition, the study proposes a new parameter to predict disease severity. Further research is required to include a larger number of patients and investigate the effect of this treatment on mortality rates.
Conclusions
Mild hyponatremia was detected in almost half of the patients with CCHF. It was determined that the severity of the disease was milder in patients with normal serum sodium levels at admission compared with patients with low serum sodium levels. This may be useful in centers where laboratory activities are limited.
Footnotes
Author Disclosure Statement
No interests to disclose.
Authors’ Contributions
B.O.Ö: Conceptualization, data curation, investigation, methodology, writing—orginal draft preparation. A.B.: Supervision, writing—orginal draft preparation. Y.H.: Data curation.
Funding Information
No funding was received for this article.