
Abstract
Objective:
This study aimed to analyze the clinical characteristics of five cases of Chlamydia psittaci pneumonia diagnosed using metagenomics next-generation sequencing (mNGS) and to provide help for its diagnosis and treatment.
Methods:
Five patients who were admitted to the department of Respiratory and Critical Care Medicine of Beijing Aerospace General Hospital between June 2020 and December 2021 and diagnosed with C. psittaci pneumonia using mNGS were selected, including one case with severe pneumonia. We analyzed the clinical characteristics, epidemiology, laboratory results, treatment, and prognosis of the five participating patients.
Results:
The main clinical manifestations were high fever, dry cough, chest tightness, shortness of breath, and myalgia. All five patients had a history of contact with poultry. The white blood cell count was normal or slightly increased, the lymphocyte count was significantly decreased, and the percentage of neutrophil granulocyte, C-reactive protein (CRP), erythrocyte sedimentation rate, and procalcitonin were significantly increased. Chest computed tomography showed inflammatory infiltration and consolidation of one or more lung lobes, possibly accompanied by pleural effusion and liver function impairment. Bronchoscopy mainly showed congestion and edema of airway mucosa with less sputum in the airway. In all patients, we detected the nucleic acid sequences of C. psittaci in alveolar lavage fluid or sputum using mNGS and confirmed the diagnosis of C. psittaci pneumonia based on clinical manifestations and exposure history. After adjusting antibiotics to a moxifloxacin-based treatment regimen, the disease improved. The application of the mNGS assay enables us to make faster diagnoses of diseases so that timely medication can be administered, thus shortening the duration of a patient’s illness.
Conclusion:
C. psittaci pneumonia has an acute onset, and fever and cough are common symptoms. A history of contact between the patient and birds is an important diagnostic clue; however, clinical symptoms and laboratory and imaging examinations lack specificity. The detection using mNGS of bronchoalveolar lavage fluid can quickly confirm the diagnosis and reduce missed diagnoses and misdiagnoses. Moxifloxacin-based therapy is effective, and patients require combination therapy if they have other bacterial infections.
Introduction
Chlamydia psittaci is an intracellular Gram-negative pathogen first isolated from parrots. It causes disease in humans and animals mainly through aerosol inhalation or close contact with infected secretions, feces, or feathers. C. psittaci occurs not only in parrots but also in pigeons and poultry, including chickens and ducks. One study found that among poultry sold in the market, the prevalence of parasitic diseases in chickens, ducks, and pigeons was 13%, 39%, and 31%, respectively (Chau S et al., 2015), and contact with birds or poultry was considered a major risk factor for human infection with C. psittaci. C. psittaci is highly pathogenic. Knittler and Sachs reported that C. psittaci is more pathogenic and has a faster reproductive rate than other chlamydiae; therefore, C. psittaci causes a more severe inflammatory response (Knittler and Sachse, 2015).
C. psittaci can survive in vitro and is therefore more likely to cause human-to-human transmission. In recent years, it has been reported in relevant foreign literature that C. psittaci pneumonia accounts for 1%–5% of community-acquired pneumonia (Qin et al., 2022). When humans come into contact with secretions, feces, or feathers of infected birds, C. psittaci enters the human body through the respiratory tract in the form of aerosols. After C. psittaci enters the human body, it first enters the reticuloendothelial cells of the liver and spleen to proliferate and then enters the lungs and other organs through the blood. Therefore, human infection with C. psittaci is a systemic infectious disease with flu-like symptoms, such as fever, chills, headache, and muscle aches. Severe infections can lead to pneumonia, respiratory failure, endocarditis, liver and kidney dysfunction, coagulation abnormalities, and gastrointestinal symptoms and can also involve the central nervous system (Qin et al., 2022; Shi et al., 2021). Pulmonary infection is the most common site, and systemic infections, such as in the circulatory system, digestive system, hematological system, and nervous system, may also be present (Fraeyman et al., 2010). Pulmonary imaging findings mainly indicate single lobe involvement (usually the lower lobe), significant plaque exudation, partial consolidation, and a small amount of pleural effusion.
Due to the atypical clinical symptoms of psittacosis pneumonia, conventional detection methods lack specificity and sensitivity and are easy to ignore, leading to misdiagnosis (de Gier et al., 2018). Therefore, few clinically diagnosed cases of psittacosis pneumonia have been reported. Metagenomics next-generation sequencing (mNGS), a new detection technology, can rapidly and accurately detect and identify microorganisms, including viruses, fungi, and atypical pathogens that are often difficult to culture, by comparing sequences. mNGS is increasingly used in the diagnosis of infectious diseases, especially when conventional diagnosis is limited (Chen et al., 2020). In this observational study, mNGS technology was applied to diagnose psittacosis pneumonia, and the clinical characteristics of the cases were retrospectively analyzed. In this article, the clinical manifestations, diagnosis methods, and treatment plans of psittacosis chlamydia pneumonia are comprehensively discussed and analyzed.
Materials and methods
Research participants
This observational study was conducted with five patients diagnosed with C. psittaci pneumonia using mNGS who were admitted to the Department of Respiratory and Critical Care Medicine of Beijing Aerospace General Hospital between June 2020 and December 2021. Diagnosis of C. psittaci pneumonia was based on clinical presentation and at least one of the following laboratory tests: (1) C. psittaci pathogen was detected in respiratory specimens; (2) in repeated serum samples, complement fixation experiments or micro immune fluorescence (MIF) experiments showed antibody titers at least fourfold higher than the upper limit of normal; (3) the titer of immunoglobulin M antibody against C. psittaci detected through the MIF assay was 1:16. Informed consent was obtained from all patients.
Methods
Data collection
For the selected cases, demographic and clinical data were extracted from electronic medical records with recorded medical histories and treatment details, while biological samples were collected within 24 h of hospitalization. Follow-up information (including symptom recurrence and adverse reactions) was obtained via structured telephone interviews at 6 months postdischarge. All data underwent dual-entry verification by independent researchers to ensure accuracy.
Metagenomics next-generation sequencing test sample processing and deoxyribonucleic acid extraction
Bronchoalveolar lavage fluid (BALF) specimens: bronchoscopy and bronchoalveolar lavage were performed under general anesthesia by professional bronchoscopy physicians who were trained in a standardized manner. Bronchoalveolar lavage fluid was attracted and obtained by an absorber. BALF was aliquoted into two 15 mL sterile polypropylene tubes (Axygen, USA) under a biosafety cabinet. One tube was treated with RNA stabilizer (RNAlater, ThermoFisher) for mNGS, while the other remained untreated for culture. Both tubes were stored at −80°C within 30 min postcollection.
Bronchoalveolar lavage fluid culture and BALF mNGS detection were performed, and the sample sizes were ≥3 and ≥5 mL, respectively. Sputum samples: if an artificial airway was established, a disposable sputum collector was used to obtain sputum; if no artificial airway was established, sputum was collected in the morning, and the patient gargled with a small amount of water at least three times before sputum retention and then breathed hard to cough up sputum from the deep respiratory tract and put it into the sputum box. The amount of sputum in each specimen was ≥1 mL; specimens were immediately sent for inspection after each collection.
Metagenomics next-generation sequencing detection process
(1) DNA extraction: the sample was broken and centrifuged, 600 µL of the supernatant was taken, and DNA was extracted using a DNA extraction kit (1901, Genskey, Tianjin, China); (2) library establishment: the extracted DNA was broken into fragments of 200–300 bp in size, and DNA end repair, adapter ligation, and polymerase chain reaction (PCR) amplification were performed using an NGS library construction kit (1906, Genskey). Amplified libraries and inserts were quality controlled using an Agilent 2100 Bioanalyzer (Agilent Technologies, Santa Clara, CA, USA), and DNA library concentrations were determined using quantitative fluorescence PCR; (3) sequencing: on-board sequencing was performed using an Illumina NextSeq 550 sequencer with a sequencing mode of SE75 and sequencing data size of ≥20 M reads; (4) bioinformatic analysis: low-quality and sequences <35 bp in length were filtered out. Using Burrows–Wheeler Aligner software alignment, the data of aligned human reference genome sequences in high-quality data were compared with a special large database of four microorganisms to obtain the number of sequences that can match a certain pathogen, and the possible pathogens were judged according to the level of the number of sequences and other clinical tests.
Laboratory and imaging examinations
Blood samples of all patients were taken in strict accordance with standard venous blood collection procedures after admission. Venous blood routine and blood biochemistry were analyzed using a whole blood cell analyzer and blood biochemistry analyzer, respectively. Serum CRP was measured using an immunofluorescence analyzer, and serum procalcitonin (PCT) was measured through the electrochemiluminescence method.
Results
Basic information and clinical manifestations of the five cases
The study included five Beijing residents (three females and two males) ranging in age from 36 to 84 years. Two had severe C. psittaci pneumonia. All of the patients had acute onset, fever with a peak temperature of 38.5°C–40°C, cough (mainly dry) and no obvious expectoration, all accompanied by fatigue. All five patients had a history of contact with birds or poultry. Two patients had dyspnea or shortness of breath, and blood gas analysis suggested respiratory failure (see Table 1).
Basic Information, Clinical Features, Treatment and Outcome of the 5 Cases
Metagenomics next-generation sequencing test results
A bronchoscopy was performed, and BALF was collected from the four younger patients and saliva from one patient. Forty-nine C. psittaci-specific sequences were detected in sputum specimens from patient 1 using the mNGS technique, 90 sequences were detected in the BALF specimen of patient 2, 88 sequences were detected in the saliva specimen of patient 3, 314 sequences were detected in the BALF specimen of patient 4, and 134 sequences were detected in the BALF of patient 5 (see Table 2). The other microorganisms were either commensal respiratory flora or environmental nonpathogens, which were unlikely to synergistically contribute to the observed symptoms.
mNGS Results
Laboratory examinations
All patients included in this study underwent blood-related tests, such as blood routine, blood biochemistry, and inflammatory parameters, at admission. Laboratory examination showed that among the five patients, three had normal white blood cells, one had slightly elevated white blood cells, one had significantly elevated white blood cells, four had elevated neutrophils, and one had normal neutrophils; all five had increased ESR and CRP, three had elevated PCT, three had hyponatremia, and three had abnormal liver function (see Table 3).
Laboratory Value of the 5 Patients
Imaging examination
In the four patients reported in this article, the main manifestations of lung computed tomography (CT) were spot exudation and consolidation, and no obvious lymph node enlargement was found; however, one male patient with severe psittacosis pneumonia developed pleural effusion (see Figs. 1 and 2).
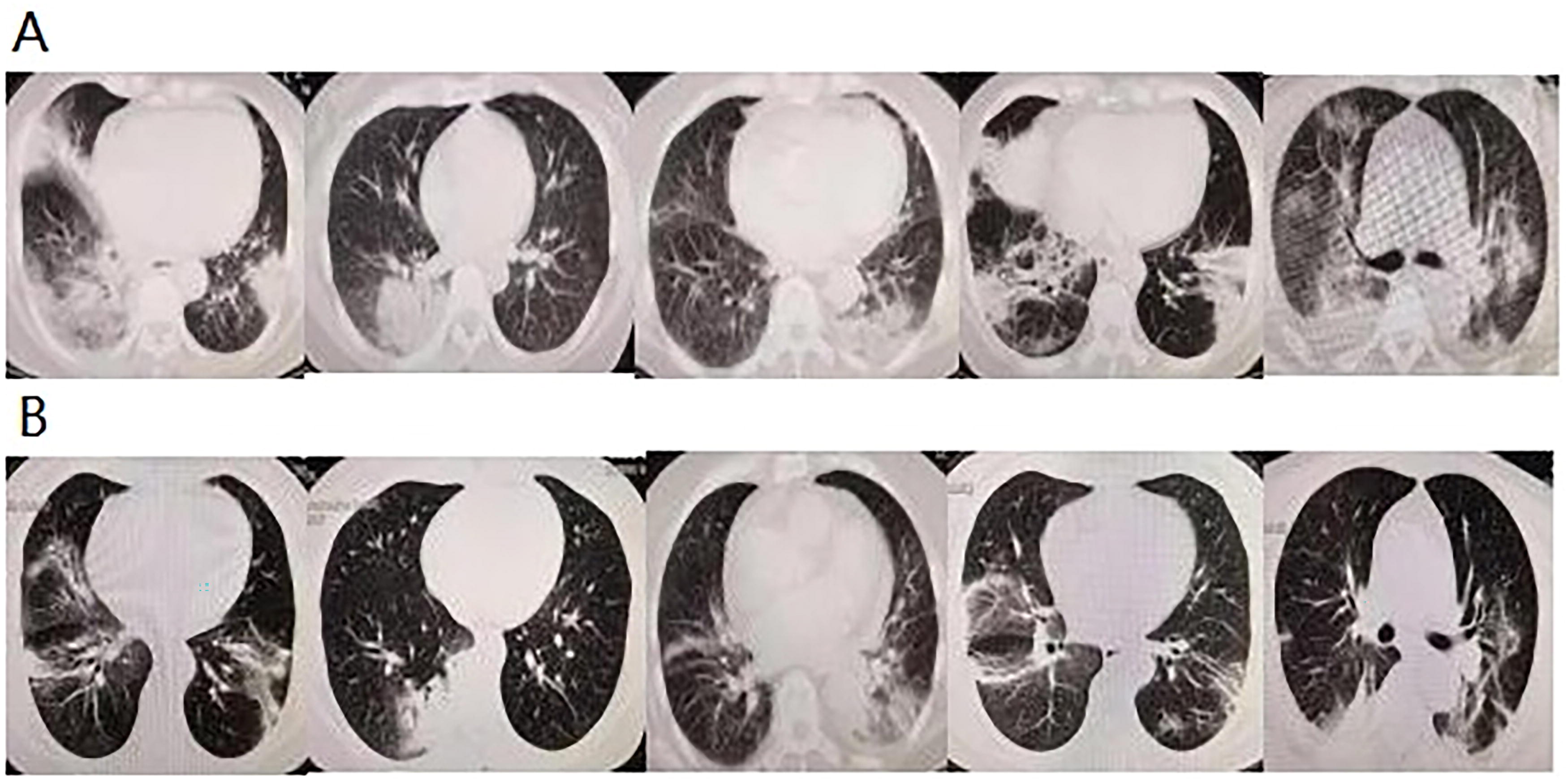
Mediastinal window of chest CT imaging of five patients.
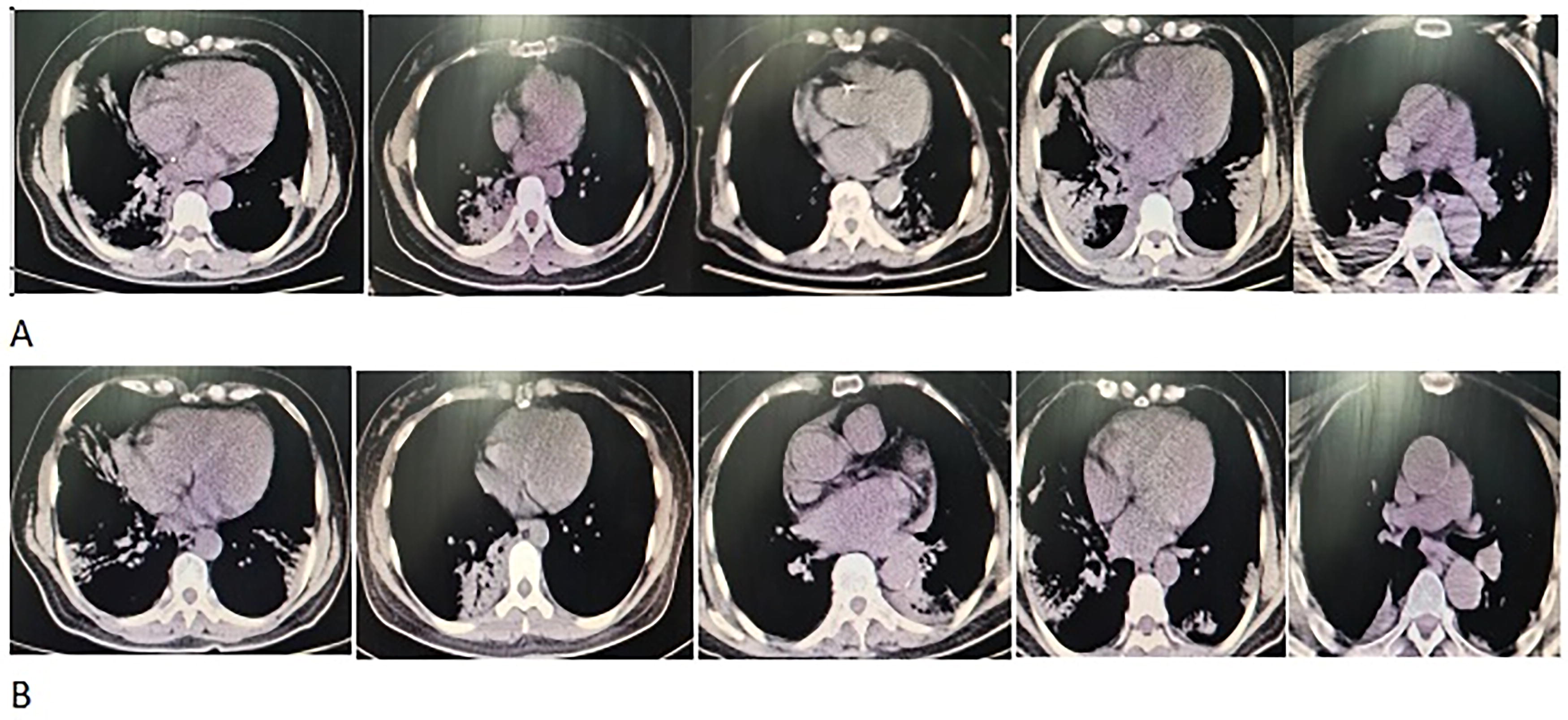
Chest imaging of five patients.
Treatment and prognosis
Combined with the clinical symptoms, contact history, chest CT, laboratory examination, and mNGS test results, all patients were diagnosed with C. psittaci pneumonia, and an anti-infection treatment regimen based on tigecycline, moxifloxacin, and levofloxacin was given to the patients to use together. Subsequently, the temperature of the five patients gradually returned to normal, the lesions in the lung were gradually absorbed, and the patients were discharged after improvement. The duration of treatment averaged 13 days. At the last follow-up (6 months postdischarge), no adverse reactions or symptom recurrence were reported, with vital signs and laboratory parameters within normal ranges.
Discussion
From the above cases, it can be seen that psittacosis pneumonia is not typical in clinical symptoms, routine laboratory examination, or chest imaging and lacks specificity, which is often ignored by clinicians and easily misdiagnosed. Its main clinical manifestations include high fever, chills, headache, myalgia, cough, and pulmonary infiltration. In severe cases, symptoms can also include severe pneumonia, septic shock, respiratory failure, liver and kidney insufficiency, abnormal coagulation function, heart damage, irritability, and coma. If there is no clear epidemiological basis for this disease, it is often misdiagnosed as common atypical pneumonia. Moreover, multiple organ systems are often involved, and it is easily misdiagnosed as Legionella pneumonia (Gacouin et al., 2012). Some 80% of the patients with psittacosis pneumonia had abnormal findings on chest radiographs, which showed different degrees of exudation and consolidation. The most common sign is single-lobe consolidation with air bronchograms. Radiating outward from the hilus of the lung or showing subpleural wedge-shaped plaques with uneven density, the solid change in the lateral field of the lung is serious, showing fan-shaped lesions; the more severe cases may involve the whole lung lobe. A CT scan can show that the lesion area may present solid nodules, ground glass lesions, and bronchial vascular thickening. The lower lobe is mainly involved, and the whole lung lobe may be involved in severe cases. A small amount of pleural effusion can be seen, and hilar lymph node enlargement is rare (Beeckman and Vanrompay, 2009).
The prevalence of parrot fever is 2.1% in patients with complicated or atypical pulmonary infection across 14 provinces and municipalities in China. The prevalence of this disease remains low and sporadic, ranging from 0% to 2.1%, as described in the literature (Hogerwerf et al., 2017). A patient’s history of avian exposure can be an important basis for the diagnosis of C. psittaci pneumonia, and patients with severe C. psittaci pneumonia are more likely to have elevated inflammatory biomarkers and elevated cardiac markers, which is consistent with the findings of the present study (Huang et al., 2023). Lung infection is the main manifestation of psittacosis, and BALF is usually recommended. C. psittaci is detected both in BALF and sputum but is higher in BALF, which suggests that BALF may be the best specimen to examine for C. psittaci; however, sputum can still be used, which is in line with the findings of the present study (Yuan et al., 2024).
The main criteria for clinical diagnosis of psittacosis pneumonia are symptoms of influenza-like severe acute respiratory syndrome and a history of contact with birds. Most patients have a normal white blood cell count. In this article, three patients had normal white blood cell counts, and one severely affected patient had an elevated white blood cell count. Because the clinical symptoms of psittacosis pneumonia are not typical, the clinical diagnosis mainly depends on laboratory diagnosis, which includes culture, serological detection, and PCR (Gacouin et al., 2012; Beeckman and Vanrompay, 2009). However, due to the low efficiency of pathogen isolation and culture of C. psittaci, the strict requirements for laboratory biosafety levels cannot be routinely performed (Nieuwenhuizen et al., 2018). Testing for C. psittaci is not routinely available in most hospitals in China, including many tertiary hospitals.
mNGS is a new microbial detection technology with high throughput, rapid and accurate identification of microorganisms through sequence comparison, and a wide detection range, which is used in the diagnosis of meningitis, encephalitis, and lower respiratory tract infection (Schlaberg et al., 2017; Wilson et al., 2019). In addition, many microbial cultures are negative in clinical practice, and mNGS can accurately and quickly detect infectious microorganisms, which is a key advantage over other detection methods. However, mNGS also has certain limitations. It does not easily distinguish between microbial colonization and pathogenic infection, it cannot determine the drug resistance of pathogenic bacteria, and it is more expensive than a general examination (Lal Gupta et al., 2020). Using mNGS in patients with atypical pneumonia is worthwhile and can shorten the time to diagnosis and the course of the disease and improve the prognosis. In previous studies, routine detection methods have included culture, complement fixation test, MIF, and PCR. However, these methods have various limitations in screening for psittacosis, such as low sensitivity/specificity and prolonged detection time, which lead to underdiagnosis or misdiagnosis of psittacosis (Duan et al., 2022). mNGS is effective in detecting the presence of psittacosis, especially in the presence of low-copy atypical pathogens (Gu et al., 2021). Its benefits include the following: (a) compared with culture and serological tests, mNGS has higher sensitivity and specificity, especially for low-copy atypical pathogens, and it has a greater ability to detect probable pathogens; (b) compared with targeted assays such as serological testing and PCR, mNGS identifies uncommon and unknown pathogens, and it can identify the potential coinfections of multiple pathogens, such as the respiratory and central nervous system; (c) mNGS enables faster detection.
Antibiotics with high intracellular activity, such as tetracycline, macrolides, and neofluoroquinolone, should be selected for the treatment of this disease, the main mechanism of which is interference with DNA and protein synthesis (Kohlhoff and Hammerschlag, 2015). For the treatment of psittacosis, tetracyclines, such as doxycycline or minocycline, are usually recommended as the first choice, whereas macrolides, such as erythromycin or azithromycin, are recommended when tetracyclines are contraindicated (Ni et al., 2023). Quinolones have been documented to be effective in the treatment of C. psittaci pneumonia (DE Boeck et al., 2016). Therefore, we chose tigecycline, levofloxacin, and moxifloxacin and observed that the clinical effect on patients was ideal. Because this disease is different from common atypical pneumonia, the lesion absorption is slow, and the average time of lesion absorption is 6 weeks (reaching 20 weeks in elderly patients); therefore, it is currently believed that the treatment course must last at least 10–14 days (Jia, 1996).
A limitation of this study is the small sample size due to the low incidence, which may lead to less significant representativeness. However, the obtained results also have a certain reference value, which can enable clinicians to understand more clinical features of the disease and help improve the diagnostic level. In future studies, the sample size should be increased to increase representativeness.
Conclusion
In clinical work, clinicians should maintain vigilance for C. psittaci pneumonia, especially in critically ill patients, and recommend mNGS examination as early as possible to confirm the diagnosis promptly; this can help reduce misdiagnosis and missed diagnoses and improve prognosis.
Footnotes
Authors’ Contributions
W.W. conceived of the study and design it. C.-L.Y. and Q.-S.X. participated in the data collection and helped with the data analysis. All authors took part in drafting and revising the article. All authors read and approved the final article.
Ethics approval and consent to participate
The study followed the basic principles of the declaration of Helsinki and was approved by the Ethics Committee of Beijing Aerospace General Hospital (2023-LC-54).
Written informed consent was obtained from all participants.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.