
Abstract
Hepatitis C virus (HCV) infection causes chronic hepatitis, which gradually progresses to liver cirrhosis and subsequently to hepatocellular carcinoma (HCC). Angiogenesis plays a major role in chronic inflammation and may have prognostic value in disease progression. This study was designed to evaluate vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), and tumor necrosis factor-α (TNF-α) as prognostic factors of disease progression in Egyptian patients with different stages of HCV-related cirrhosis and HCC. VEGF, PDGF, and TNF-α were measured using enzyme-linked immunosorbent assay (ELISA) in 82 HCV-infected patients (20 mild, 20 moderate, and 20 severe cirrhosis patients, and 22 HCC patients), and 20 healthy controls. Our results showed comparable increases in VEGF and PDGF levels in those with increasing clinical stages of disease, with maximal production seen in HCC patients. A gradual elevation of TNF-α levels was seen also in HCV-infected patients at different stages of disease and HCC. A statistically significantly positive correlation between serum levels of VEGF, PDGF, and TNF-α, and grade of disease was recorded. Thus assessment of these parameters in those with different stages of disease may be helpful in choosing the best treatment strategy, and indicate that anti-angiogenic therapy may be useful.
Introduction
Among the factors contributing to liver damage during chronic HCV infection, angiogenesis, or the formation of new blood vessels, has been reported to play a significant pathogenic role (13 –15). Tumors cannot grow beyond a certain size, generally 1–2 mm, due to a lack of oxygen and essential nutrients (16). Accumulation of inflammatory infiltrates and the development of fibrosis increases resistance of the tissue to blood flow and delivery of oxygen. Under these circumstances angiogenesis may occur, leading to upregulation of the pro-angiogenic factors responsible for vascular remodeling and new vessel formation (17 –19). Various soluble growth factors can induce neovascularization into the tumor by inducing endothelial cell proliferation, supplying required nutrients, and allowing the tumor to grow (20 –22). Angiogenesis in HCC is based on these same fundamental principles (21,23 –25). Induction of endothelial cell growth and differentiation require that pro-angiogenic factors interact with their corresponding receptors as they are expressed and activated in cells (26). This expression is normally localized to the cell surface, although proteolysis has also been described, which results in the appearance of receptors in the serum (27), which are then considered soluble factors. Determination of angiogenic factors and their soluble receptors in the serum may represent an important tool for the follow-up of diseases in which angiogenesis has been demonstrated at the molecular level, such as chronic HCV, autoimmune liver disease (28), and HCC (29).
Clinical follow-up of liver disease often involves using invasive techniques such as biopsies, procedures that are not without risks. Therefore it is important to identify serum markers that may provide information about the extent of disease progression without the need for biopsies. The first step in identifying such factors is to focus on molecules that play a role in the development of a given disease. Then its levels in the serum should be studied, and possible associations between those levels and disease progression should be investigated. Determination of angiogenic factors and their soluble receptors in the sera of HCV-infected patients may represent an important tool for the follow-up of liver disease patients (30). Thus, the present study aimed to investigate the clinical significance of angiogenesis, as assessed by serum levels of vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF), and the proinflammatory cytokine tumor necrosis factor-α (TNF-α), as prognostic factors of disease progression in Egyptian patients with different stages of HCV-related cirrhosis and HCC.
Materials and Methods
Patients and controls
The study participants were a group of patients admitted to the outpatient clinic of the National Liver Institute, Menofia University, Sadat City, Egypt. All investigations were done in accordance with Menofia University health and human ethical clearance committee guidelines for clinical research. Institutional research committee approval was sought before carrying out the study, and all patients gave their informed consent. History and clinical examination findings were gleaned from hospital records.
Virological assessment
HCV antibodies were measured using a third-generation enzyme-linked immunosorbent assay (ELISA) (Murex Biotech Ltd., Dartford, U.K.), and confirmation of the presence of serum viral HCV RNA in HCV-positive patients was performed using a standard polymerase chain reaction technique (Promega Corp., Madison, WI). Hepatitis B surface antigen (HBsAg) was measured using commercially available kits (Sorin Biomedica, Milan, Italy). All patient groups were positive for HCV antibody and HCV RNA, and negative for HBsAg. One-hundred and two HCV-infected patients were included in the study. Twenty healthy individuals with no history of previous liver disease, normal liver function, and negative HCV serology served as normal controls.
Sera were collected from all patients and controls. The sera were separated by centrifugation at 1500 rpm for 15 min at 4°C, aliquotted, and stored at −80°C until analysis. Alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP) (bioMérieux sa, Marcy l'Etoile, France), direct and indirect bilirubin (Roche Diagnostics Corp., Indianapolis, IN), and albumin (Human Gesellschaft Fur Biochemica Und Diagnostica Mbh, Wiesbaden, Germany), were all measured according to their respective kits' manufacturers' instructions.
Angiogenesis markers
Serum levels of VEGF, PDGF, and TNF-α were quantified by ELISA. The assays were based on the quantitative sandwich immunoassay technique, which uses immobilized monoclonal antibody and biotin-linked polyclonal antibody, both of which are specific against human VEGF, PDGF, and TNF-α. Commercially available matched paired antibodies were used (R&D Systems Inc., Minneapolis, MN). For measurement of VEGF, monoclonal antibody (anti-human VEGF, 1 μg/mL) was used as the first antibody (capture), and biotin-labeled anti-human VEGF polyclonal antibody (50 ng/mL) as the second antibody (detection). Anti-human PDGF monoclonal antibody (1 μg/mL), and biotin-labeled anti-human PDGF polyclonal antibody (100 ng/mL) were used as first and second antibodies, respectively. For TNF-α, the first anti-human monoclonal antibody (4 μg/mL), and the second biotin-labeled anti-human TNF-α polyclonal antibody (200 ng/mL) were used.
The first (capture) antibody was coated onto 96-well flat bottom microtiter plates (Griener Labortechnik, Kremsmunster, Austria) in phosphate-buffered saline (PBS; Sigma Chemical Company, St. Louis, MO) at 50 μL/well, and incubated for 1 h at 37°C, then overnight at 4°C in a humidified chamber. The plates were washed three times with washing buffer (PBS/0.05% polyoxyethylene-20; Tween-20), blocked with 200 μL/well of blocking buffer (PBS/0.05% Tween-20/5% fetal bovine serum [FBS]; Sigma) and incubated at 37°C for 1.5 h. Triplicate assays on 50-μL aliquots of serum samples were quantified by reference to recombinant human standards added to each plate and incubated for 1 h at 37°C. At the end of the incubation period, the plates were washed three times with washing buffer, and diluted second biotin-labeled antibody was added and incubated for 1 h at 37°C. After washing away any unbound material, peroxidase-conjugated streptavidin (Jackson ImmunoResearch, West Grove, PA) diluted 1:1000 was added at 50 μL/well, then the plates were incubated for 1 h at 37°C. After intensive washing, the enzyme reaction was carried out by adding 50 μL/well of substrate solution (equal volumes of 3,3′,5,5′-tetramethyl benzidine [TMB; 0.4 g/L] and H2O2 [0.02% in citric acid buffer; Kirkegaard and Perry Labs, Gaithersburg, MD). Color development was stopped by the addition of 50 μL/well of stopping buffer (1 M HCl) (Surechern Products, Needham Marker, Suffolk, England). The intensity of the developed color was measured by reading optical absorbance at 450 nm using a microplate reader (FLUOstar OPTIMA; BMG Labtech GmbH, Offenburg, Germany). The ELISA reader-controlling software processed the digital data of raw absorbance values into a standard curve, from which the VEGF, PDGF, and TNF-α concentrations of the samples were derived.
Statistical analysis
All statistical analyses were performed using SPSS version 10 (SPSS, Inc., Chicago, IL). Data are presented as means with corresponding SE. Comparisons between different groups of patients were performed by one-way analysis of variance. Tukey's test was used as a post-hoc test. Correlation among variables was determined using Pearson's correlation test. In all tests the level of significance was set at p <0.05.
Results
Clinical and demographic data of the studied population
We enrolled 82 HCV-infected patients in this study. All HCV patients had genotype IV. They were classified using the necroinflammatory grading system (31). Twenty patients had mild (MI), (Ishak score 3–8), 20 patients had moderate (MO) (Ishak score 8–13), and 20 patients had severe (SE) (Ishak score 13–18) cirrhosis, and 22 patients had HCV-related HCC. Hepatic fibrosis scores (31) were defined as mild fibrosis (Ishak score = 2), moderate fibrosis (Ishak score = 3 or 4), and severe fibrosis (Ishak score = 5 or 6). Twenty healthy individuals who were men and women with no history of previous liver disease, normal liver function tests, and negative HCV serology served as normal controls (Cont). Table 1 summarizes the demographic, clinical, and serological characteristics of the patients. A positive correlation (r = 0.377, p < 0.001) was found between the age of the patients and the progression of disease.
All data are presented as mean ± SE.
MI, mild cirrhosis; MO, moderate cirrhosis; SE, severe cirrhosis; HCC, hepatocellular carcinoma; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase.
HCV infection and angiogenesis factors
Serum levels of VEGF in HCV patients (MI, MO, and SE), although elevated over those in healthy controls, did not reach statistical significance. The results in Fig. 1 demonstrate a statistically significant difference in serum levels of VEGF in patients with HCC compared with normal controls (p < 0.001). Comparing patients at different clinical stages of HCV infection showed a comparable increase in VEGF production level at the different stages of disease, with a significant increase in HCC patients compared to those with MI (p < 0.001), MO (p < 0.01), and SE (p < 0.01) cirrhosis.

Serum levels of vascular endothelial growth factor (VEGF) in HCV-infected patients at different stages of infection. Results are expressed as mean ± standard error (Cont, controls; MI, mild disease; MO, moderate disease; SE, severe disease; HCC, hepatocellular carcinoma; a = groups statistically significantly different from controls; b = groups statistically significantly different from HCC patients; **p < 0.01, ***p < 0.001).
When considering PDGF, a significant difference was found between the levels of PDGF in the MI group, MO group (p < 0.01), and normal controls (Fig. 2). Patients who developed HCC showed high levels of PDGF compared to normal controls (p < 0.001). No difference in PDGF levels were found between the groups with different stages of cirrhosis. Significant differences in PDGF levels were found between each cirrhotic stage and HCC patients (p < 0.05, p <0.05, and p < 0.001, for the MI, MO, and SE groups, respectively).
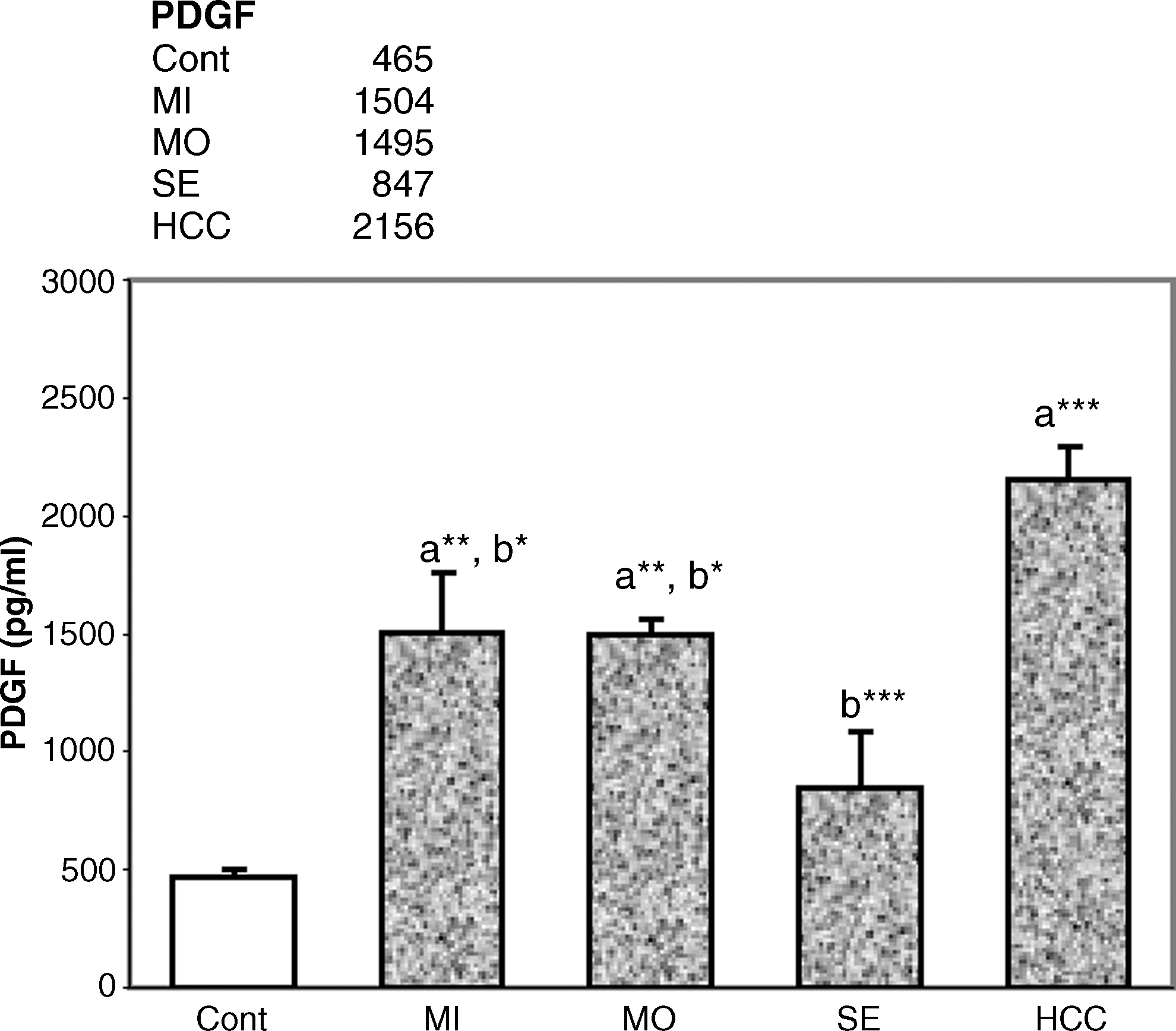
Serum levels of platelet derived growth (PDGF) in HCV-infected patients at different stages of infection. Results are expressed as mean ± standard error (Cont, controls; MI, mild disease; MO, moderate disease; SE, severe disease; HCC, hepatocellular carcinoma; a = groups statistically significantly different from controls; b = groups statistically significantly different from HCC patients; *p < 0.05, **p < 0.01, ***p < 0.001).
Compared with normal controls, gradual elevations in TNF-α levels were reported in HCV-infected patients with increasing severity of cirrhosis (p < 0.001), and HCC patients (p < 0.001) (Fig. 3). TNF-α levels in all three cirrhotic groups displayed high levels of TNF-α production; however, no statistically significant differences were detected between them. HCC patients had the highest levels of TNF-α.
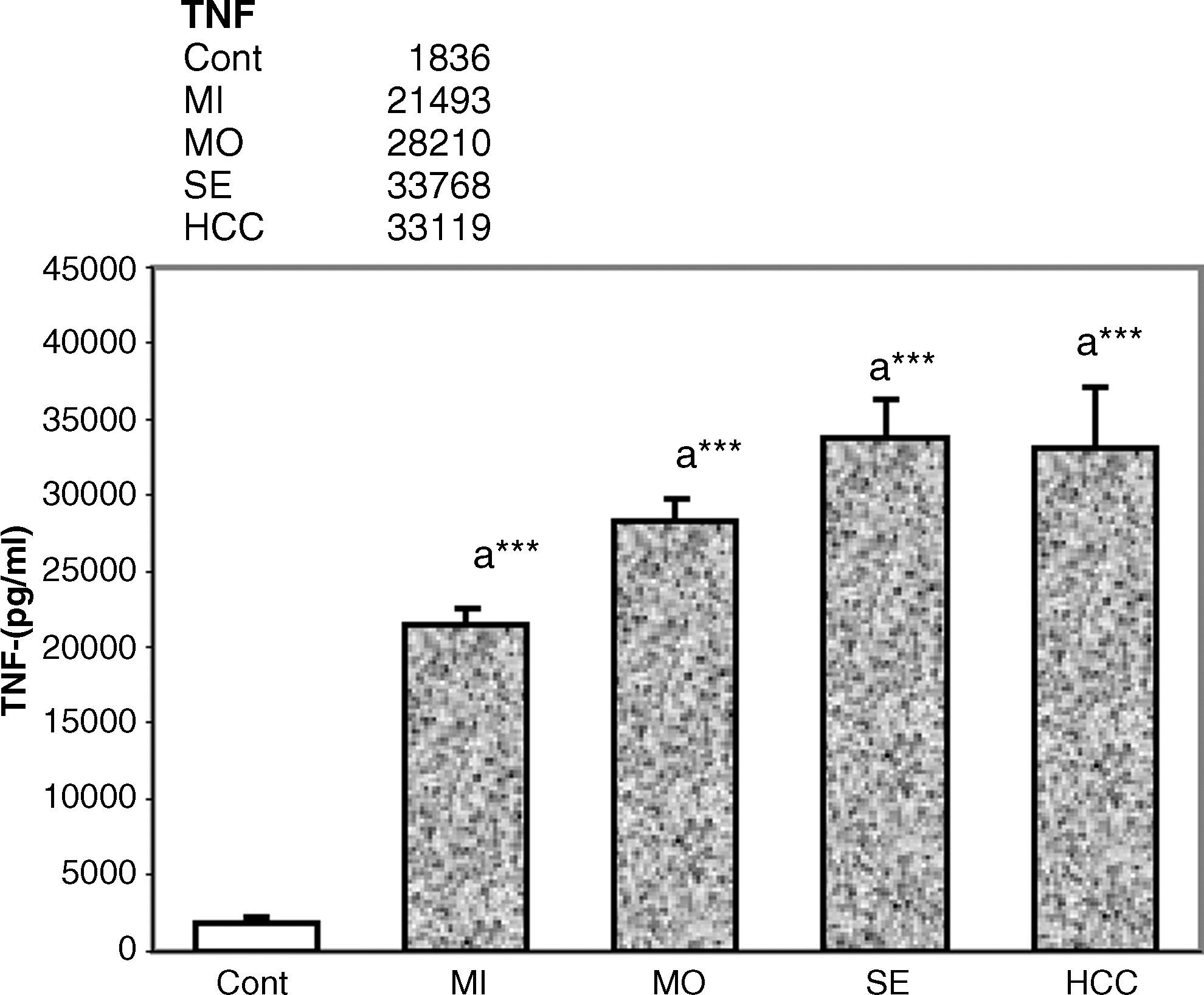
Serum levels of tumor necrosis factor-α (TNF-α) in HCV-infected patients at different stages of infection. Results are expressed as mean ± standard error (Cont, controls; MI, mild disease; MO, moderate disease; SE, severe disease; HCC, hepatocellular carcinoma; a = groups statistically significantly different from controls; ***p < 0.001).
Correlation between disease severity and angiogenesis factors
A statistically significant positive correlation between serum levels of VEGF (r = 0.372, p < 0.001), PDGF (r = 0.355, p <0.001), and TNF-α (r = 0.554, p < 0.001), and severity of disease was found. VEGF level was also directly related to PDGF level (r = 0.316, p < 0.001). Comparisons of the levels of angiogenesis factors with liver enzymes showed that VEGF was positively correlated with AST (r = 0.260, p < 0.01), ALP (r = 0.270, p < 0.01), and direct and indirect bilirubin (r = 0.263, p < 0.01 and r = 0.189, p < 0.05, respectively), and inversely correlated with serum albumin (r = −0.208, p < 0.05).
Discussion
In this study it was hypothesized that the assessment of surrogate markers in the serum may provide information about the extent of angiogenesis, and thus may represent a useful tool for disease characterization and follow-up. The work detailed here endeavored to evaluate the relationship between variations in serum levels of angiogenesis markers and stage of HCV-infection and progression to HCC.
The findings showed that chronically HCV-infected patients had elevated serum VEGF levels compared to healthy controls, although the difference was not statistically significant. This finding is consistent with those of previous reports, that showed increased hepatic VEGF mRNA and protein expression in chronic HCV patients compared to healthy controls (14,32,33). Mazzanti et al. (34) suggested that HCV-associated formation of vascular structures are directly caused by the virus, based on the finding of increased angiogenesis in patients with this infection, compared to patients with non-hepatic liver disease. Here the data showed a statistically significant positive correlation between serum levels of VEGF and severity of disease. A significant correlation between serum levels of VEGF and grade of inflammation was previously reported, suggesting that inflammatory mediators are involved in the induction of angiogenesis through the overexpression of VEGF (30). Also in support of this mechanism, a clear correlation was found between liver enzyme levels (AST and ALP), which are surrogate markers of hepatic disease, and levels of soluble angiogenesis factors (such as VEGF).
Our results demonstrated statistically significantly higher serum levels of VEGF in HCC patients than in normal controls and those with the three stages of cirrhosis. In several previous studies it has been reported that high serum VEGF levels precede venous invasion and metastasis in patients with HCC (35 –38). In HCC disease there is a significant relationship between serum VEGF levels and VEGF expression in tumor cells (39). This shows that serum VEGF levels are an indirect indicator of VEGF expression in tumors (40). VEGF expression in HCC tissues has also been correlated with tumor size and histologic grade (41). It is expressed by sinusoidal endothelial cells and hepatocytes, whereas more modest expression has been reported in Kupffer cells (41,42). Similarly to our findings, Yoshiji et al. (43) also showed that VEGF expression increases significantly during liver fibrogenesis and carcinogenesis. It has been postulated that platelets may serve as scavengers or storage sites of VEGF secreted by tumors, and the release of VEGF from platelets at distant sites of metastasis may play a central role in the hematogenous spread of cancer (37,44).
Concerning PDGF, a general elevation in PDGF relative to normal controls was found in HCV-infected and HCC patients. PDGF is another important factor in the generation of new blood vessels. Pericytes (PC) stabilize blood vessels via cell-to-cell contact, and secrete factors such as PDGF (45 –48). Cancer cells cause angiogenesis (46) through the spread of endothelial cells that secrete VEGF, and activation of PC cells expressing PDGF, although PDGF itself may also increase VEGF secretion (47,49). Apart from angiogenesis, overexpression of PDGF-BB was found to be associated with increased cell proliferation and tumor progression (50). In hepatitis other sources of PDGF, in addition to activated platelets, include macrophages and Kupffer cells (51,52). The biological significance of this connection is the stimulation of fibrogenesis and mitogenesis of Ito cells in the liver (53). According to Mannaioni et al. (52), as liver damage intensifies, PDGF is elevated in the serum, and its receptor (PDGF-R) causes inflammatory infiltration of vessels scattered in the connective tissues of the liver and proliferation of Ito cells. In chronic hepatitis there is a strong correlation between PDGF-R expression, activity, and morphological changes that progress to collagen deposition (51). Decreases in PDGF may thus be predictive of effective treatment and elimination of HCV (54). In this study, a positive correlation was found between serum levels of VEGF and PDGF. This association between variations in serum levels of angiogenesis factors (VEGF and PDGF), and the progression of chronic hepatitis C supports the critical role played by angiogenesis in chronic liver disease, as has been previously suggested (28,55). Furthermore, PDGF itself may also increase VEGF secretion (47,49). Thus it appears that our data reflect an association between levels of angiogenesis markers in chronic HCV patients and the formation of new hepatic vessels.
It has been proposed that HCV-induced chronic inflammation and cytokine production may stimulate the development of fibrosis and liver cell proliferation that contribute to hepatocarcinogenesis (11). Previous studies have showed that liver angiogenesis is stimulated by inflammation-derived mediators (40,55), and fibrosis-associated hypoxia (56). TNF-α is one of the most potent proinflammatory mediators of the antiviral inflammatory response, and it enhances lymphocyte proliferation and differentiation and production of acute phase proteins, and induces cell apoptosis (57).
In this study, elevated TNF-α levels were seen in HCV-infected patients and HCC patients compared to normal controls. In accordance with our results, Castellano-Higuera et al. (58) demonstrated that patients with chronic HCV infection had higher TNF-α levels than controls. Overproduction of proinflammatory cytokines, particularly TNF-α, has been reported in patients with chronic HCV infection (59). Both in patients with chronic HCV infection and in experimental models, TNF-α levels in plasma, serum, and peripheral blood mononuclear cells are all increased (60). These results are consistent with our knowledge of the progression of chronic HCV infection, in which several mechanisms are involved, including activation of proinflammatory cytokines by the virus (61). A relationship between TNF-α, a potent inducer of inflammation and a key regulator of innate immunity, and liver inflammation (62) has also been found. Circulating TNF-α levels increase during HCV infection (63,64). Kato et al. (65) showed that HCV core protein C, and to a lesser degree NS4B protein, influence cell proliferation and production of proinflammatory cytokines such as IL-1, IL-6, and TNF-α. TNF-α is beneficial for the generation of the initial immune response against viruses, including HCV (66). Increased production of TNF-α in the T cells, NK cells, and dendritic cells of chronically HCV-infected hosts was previously reported, and may deter HCV clearance (67). TNF-α-producing cells (mainly of the macrophage/Kupffer cell lineage), and the expression of TNF-α and sTNFR are increased in HCV patients (68,69). Significant elevations in serum TNF-α levels in HCC patients, well above those of controls, were demonstrated in this study. Previous studies have also demonstrated that HCC patients have significantly higher serum levels of TNF-α than controls. Increased serum TNF-α concentrations are also associated with disease progression in some other types of cancer, and TNF-α is known as an important mediator of cancer cachexia (70).
Taken together, the results of this study show that chronic HCV patients have higher levels of soluble angiogenesis markers (VEGF and PDGF) than healthy controls. The demonstration of an association between variations in serum levels of angiogenic (VEGF and PGDF) and inflammatory (TNF-α) mediators and chronic HCV progression supports the critical role played by angiogenesis in chronic liver disease. This may have important clinical implications, and determination of these parameters at different stages of infection may be helpful in patient follow-up and treatment. However, more study is required to investigate the relationship between angiogenic and inflammatory mediators and disease progression, and to explore the exact mechanisms behind these effects.
Footnotes
Acknowledgment
This work was a collaborative effort between the Genetic Engineering and Biotechnology Research Institute and the National Liver Institute (NLI). The author would like to thank Prof. Mohsen Salama at the NLI for his support and aid in clinical classification of the patients.
Author Disclosure Statement
No competing financial interests exist.