
Abstract
Asymptomatic chronic hepatitis B virus (HBV) carriers are at risk of developing complications of liver disease, but these patients are not recommended for treatment with antiviral drugs. In fact, antiviral drugs are ineffective in these patients in the immune tolerance phase, when they have inadequate levels of host immunity. We postulated that combination therapy of an immune modulator and antiviral drugs may have potential to help these patients. Twenty-five patients with incidentally-detected asymptomatic chronic HBV were immunized with hepatitis B vaccine (10 μg of hepatitis B surface antigen) intramuscularly five times (at 0, 1, 2, 6, and 12 mo) to induce HBV-specific immunity. The patients were also treated with lamivudine (100 mg) daily for 12 mo. The combination therapy was safe for all patients with asymptomatic chronic HBV, and no increases in alanine aminotransferase or liver damage were detected in any patient. Although all of the patients were expressing HBV DNA in their serum before treatment, HBV DNA became undetectable in 16 of 25 patients, and was reduced in 9 of 25 patients at the end of the combination therapy. Combination therapy with the antiviral agent lamivudine and an immune modulator (hepatitis B vaccine) represents a potential therapeutic option for the control of HBV without liver damage in asymptomatic chronic HBV carriers.
Introduction
Materials and Methods
To test our hypothesis, a group of HBV-infected patients without any subjective symptoms of liver diseases were enrolled in this study. HBV infection was detected incidentally in several hundred apparently healthy subjects when they visited our hospital for physical examinations. They came to our hospital to check for hepatitis B surface antigen (HBsAg), mainly for the following reasons: (1) to get a working visa to go to a foreign country, (2) due to the detection of HBV-infected subjects in their family, (3) before blood transfusion, and (4) during pregnancy. When HBsAg was detected in their sera, they were recommended to have a second assessment for HBsAg 6 mo later to ascertain if they were chronic HBV carriers. Informed written consent was obtained from patients with chronic HBV infection or their parents to participate in the 12-month combination therapeutic regimen after explaining the nature and purpose of the therapy. Liver biopsies were done in 14 patients. All 25 patients were expressing HBV DNA in their sera. Seven patients were expressing hepatitis B e antigen (HBeAg), whereas 18 patients were negative for HBeAg. Alanine aminotransferase (ALT) levels were above the upper limit of normal (>42 U/L) in eight patients. Eleven patients with similar clinical features were treated only with lamivudine to determine if the combination therapy had any added therapeutic benefit in chronically HBV-infected subjects. Blood samples were collected from each patient and the sera were preserved at −20°C until analysis. A complete blood count along with assessment of parameters of liver and kidney function were done in all patients at enrollment, before each vaccination, and every 3 months. In addition, all patients were informed that they should contact the director of the study (M.A.) if they had any changes in their physical condition. Serum ALT levels and prothrombin time were assessed using commercially-available tests. The cut-off value for abnormal ALT was set at 42 U/L. HBeAg was checked with an ELISA assessment kit (Abbott Laboratories, Chicago, IL). HBV DNA quantification was done via polymerase chain reaction using a commercial kit (Amplicon HBV Monitor Assay, RT-PCR; Roche Molecular Systems, Pleasanton, CA). The lower limit of detection was 500 copies of HBV DNA/mL of serum.
The ethical committee of Farabi General Hospital, Dhaka, Bangladesh, gave its approval, and this investigation was been performed in accordance with the principles of the Declaration of Helsinki.
The protocol of the combination therapy is shown in Fig. 1. All patients were given lamivudine at a dose of 100 mg/d for 12 mo. Hepatitis B vaccine (Engerix; GlaxoSmithKline, London, U.K.) containing 10 μg of HBsAg was injected intramuscularly five times (at the start of therapy, and 1, 2, 6, and 12 mo after therapy had begun). All patients were checked 2 h after vaccination to assess for any side effects.
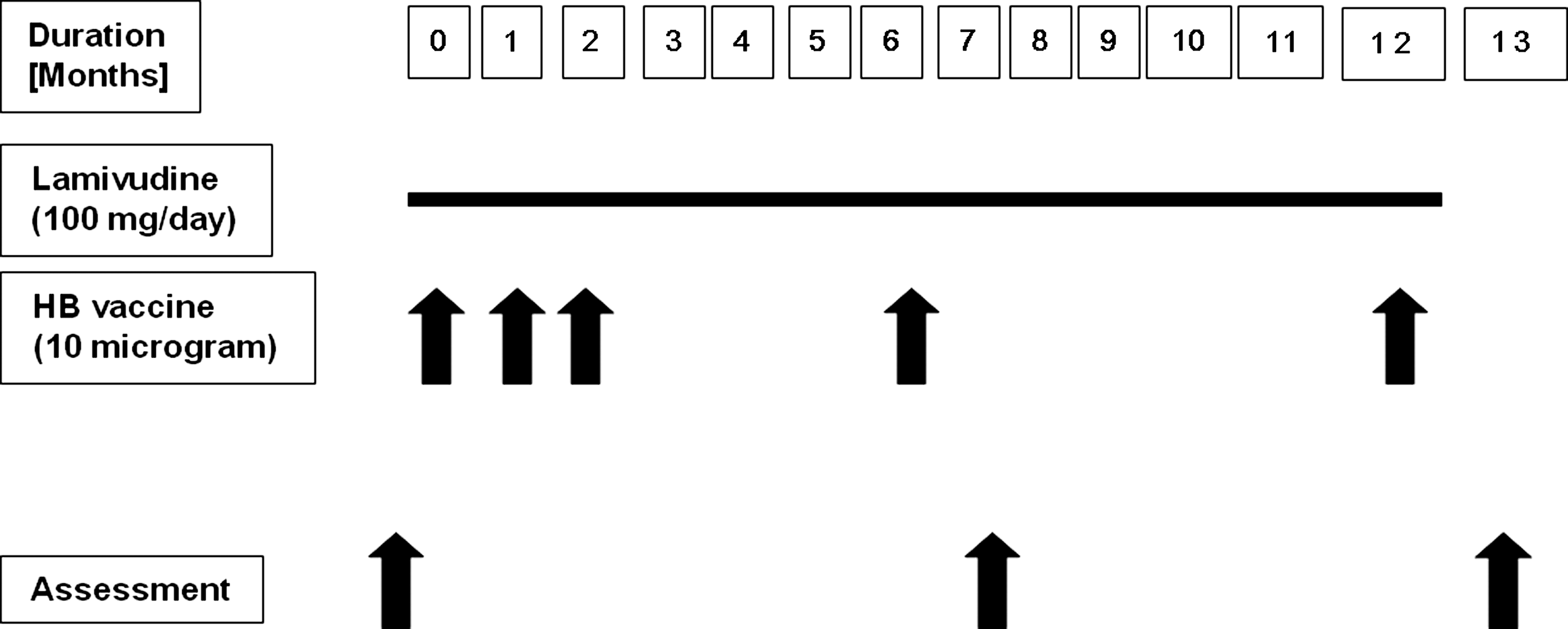
Protocol of the combination therapy used in incidentally-detected asymptomatic chronic hepatitis B virus (HBV)-infected patients. All patients were given lamivudine at a dose of 100 mg daily for 12 mo. Hepatitis B vaccine containing 10 μg of hepatitis B surface antigen was administered intramuscularly at 0, 1, 2, 6, and 12 mo. Health status was monitored periodically in all patients via total blood counts and assessments of liver and kidney function. Assessment of HBV-related virological and immunological markers was done at months 0, 7, and 13.
Results
All 25 patients continued the therapy for the entire duration of the clinical trial. No adverse effects of the combination therapy were detected in any of the patients. We also found no abnormalities in white blood cell counts or platelet counts in any of the patients, and no abnormalities in prothrombin time were seen. No elevations of ALT more than twice the pre-treatment levels were recorded in any patient, and no abnormalities in kidney function were seen.
With regard to the antiviral potential of the combination therapy, HBV DNA became undetectable (<500 copies/mL) in 16 of 25 patients (64%) after the completion of 12 mo of combination therapy (Fig. 2), and HBV DNA levels were reduced in all patients. The highest reductions in HBV DNA were seen in patients with comparatively lower baseline levels of HBV DNA; however, six patients with HBV DNA levels of >1 × 105 copies/mL became negative for HBV DNA after the combination therapy (Fig. 2). Eleven patients with comparable levels of HBV DNA were given lamivudine monotherapy for 12 mo. HBV DNA became undetectable in 4 of 11 patients (38%) in the lamivudine monotherapy group after 12 mo. Thus the combination therapy appears to have better antiviral potential than lamivudine given alone. Of the 25 asymptomatic chronic HBV carriers receiving combination therapy, 17 had normal levels of ALT, and 8 patients had elevated ALT levels. Combination therapy caused normalization of ALT in 7 of the 8 patients with elevated ALT. On the other hand, the levels of ALT dropped to normal in 4 of 11 patients receiving lamivudine monotherapy. Seven patients receiving combination therapy were HBeAg-positive, and 2 of the 7 (28%) became HBeAg-negative within 6 mo of starting therapy. HBeAg-negativity was seen in only 1 of the 11 patients (9%) in lamivudine monotherapy group.
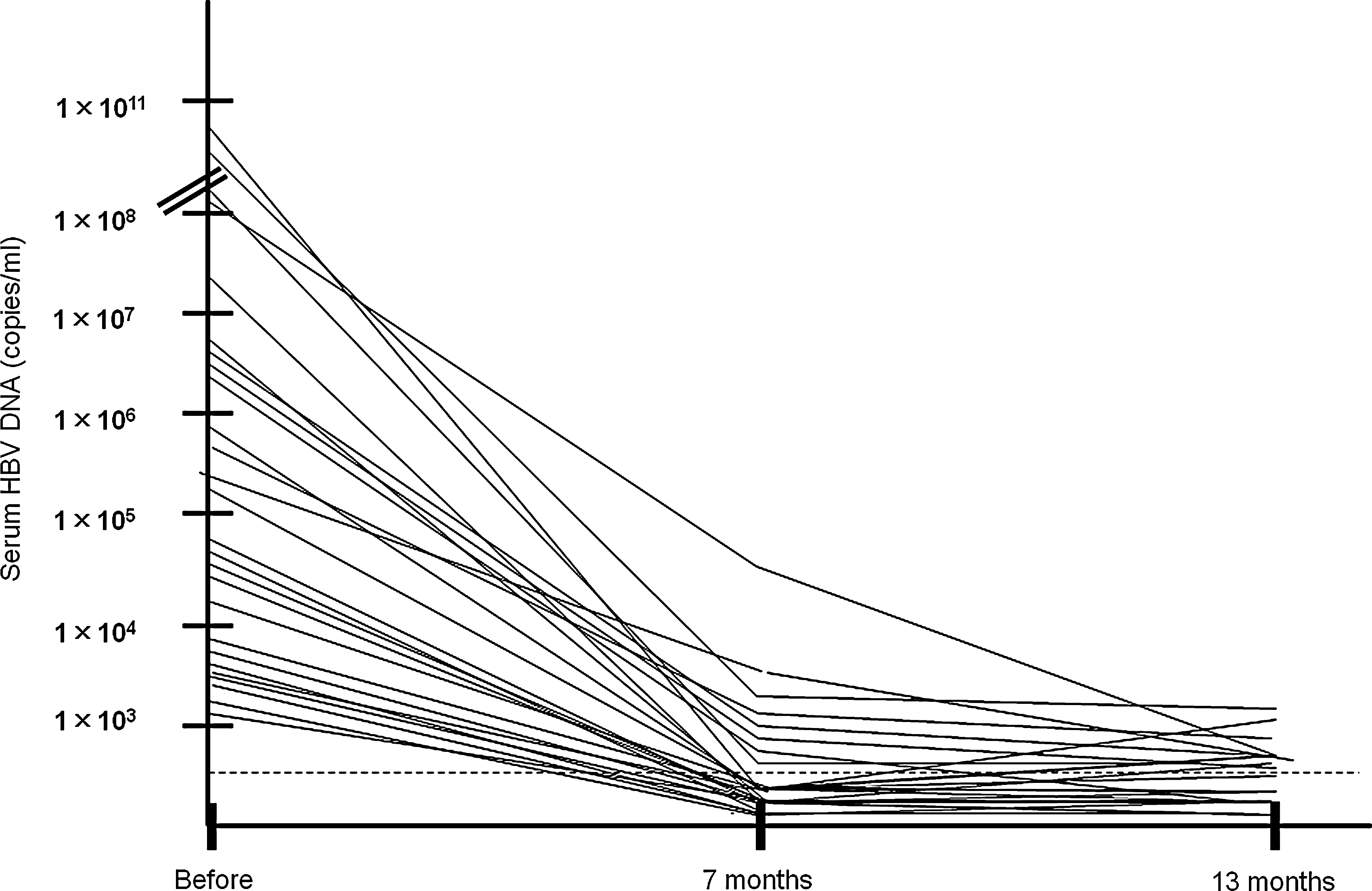
Reductions of HBV DNA were seen in all patients after combination therapy, and HBV DNA became undetectable in 16 of 25 patients in this series.
In this pilot study, we have shown that the combination of immune therapy (hepatitis B vaccine) and antiviral therapy (lamivudine) has potent antiviral potential in asymptomatic chronic HBV carriers. The extent of liver damage was also decreased in patients receiving the combination therapy. This is not the first study of combination therapy in patients with chronic HBV infection, but most of these clinical trials were carried out in patients in the immune clearance phase of chronic HBV infection (4,5). In addition, most of the published clinical trials were conducted in developed countries with advanced facilities. Our study is of interest because it was done in asymptomatic and incidentally-detected chronic HBV carriers. Also, our study was performed in Bangladesh, a developing country with 140 million people. It is thought that Bangladesh harbors about 10 million chronic HBV carriers, and that 8–9 million of them appear to be asymptomatic chronic HBV carriers. Powerful antiviral agents are now commercially available in most countries (9,10), including Bangladesh. Also, a new vaccine containing both HBsAg and hepatitis B core antigen (HBcAg) is being tested for safety and efficacy in a Phase I trial (2). Combination therapy for more extended periods may be done in future clinical trials. We believe that a more effective combination therapy regimen can be developed by using more potent antiviral agents along with more potent therapeutic vaccines (containing both HBsAg and HBcAg), and that this would further increase its efficacy in asymptomatic chronic HBV carriers.
This study has also public heath ramifications for the management of HBV infection in developing countries as well as developed countries. The numbers of patients with incidentally-detected asymptomatic chronic HBV infection are increasing in both developed and developing countries, due to increased awareness of HBV infection, and more widespread HBV testing of the general population. Asymptomatic chronic HBV carriers represent a permanent reservoir of HBV with infective potential. It is difficult to assess the extent of liver damage present without performing a liver biopsy, and antiviral treatment is not usually recommended for these patients.
The results of this study show that combination therapy is effective in reducing HBV DNA infectivity in asymptomatic chronic HBV patients, without significant side effects. If the efficacy of combination therapy is confirmed by randomized controlled trials, it may represent a new treatment option for these patients.
Footnotes
Acknowledgments
The authors are grateful to the Miyakawa Memorial Research Foundation, Tokyo, Japan, for providing funds for virological and immunological testing to Mamun Al-Mahtab and Sheikh Mohammad Fazle Akbar.
Author Disclosure Statement
No competing financial interests exist.