
Abstract
In chronic hepatitis B virus (HBV) infection, inflammation-associated cytokines including proinflammatory cytokines are involved in the development and progression of liver fibrosis. The liver is a source of many cytokines that may influence liver function. High-mobility group box 1 (HMGB1) was identified as an inflammatory cytokine. HMGB1 is present in nuclei of all mammalian cells and is released both through active secretion from various cells and by passive release from necrotic cells. Here we explore the relationship between HMGB1 plasma levels and liver fibrosis. HMGB1 serum levels, HBV-DNA, and ALT values were significantly higher in patients with chronic HBV than in controls. In addition, HMGB1 serum levels were significantly higher in patients with low fibrosis (fibrosis score 1–2) compared to those with high fibrosis (fibrosis score 3–4). In the present study, we have shown that HMGB1 is a noninvasive, repeatable, and convenient marker for distinguishing advanced fibrosis from low fibrosis in chronic HBV patients. We believe that the inhibition of HMGB1 may reduce inflammation, apoptosis, and fibrosis, and may stop the progression of chronic liver disease. Furthermore, we are of the opinion that fibrotic progression in chronic liver patients may be prevented by the inhibition of HMGB1, and that this substance can be a new means of following chronic HBV treatment.
Introduction
High-mobility group box 1 (HMGB1) was identified as an inflammatory cytokine (3,4). Increasing evidence now points to multiple functions of HMGB1 in infection, tissue injury, inflammation, apoptosis, and the immune response (5). Chronic HBV infection suggests that inflammation-associated cytokines including proinflammatory cytokines such as tumor necrosis factor-α (TNF-α) and transforming growth factor-β1 (TGF-β1), and anti-inflammatory cytokines such as interleukin (IL)-10, are involved in the development and progression of liver fibrosis (6,7).
At present, liver biopsy remains the gold standard for diagnosing the presence of fibrosis and staging the disease. It can also provide additional information, such as allowing the identification of comorbidities. Nevertheless, liver biopsy remains an invasive procedure with a morbidity rate of 0.3–0.6% and a mortality rate of up to 0.05%. Most importantly, liver biopsies, particularly small biopsies, are a questionable gold standard due to limitations, including significant sampling error and poor intra- and interobserver concordance (8,9,10).
The development of routine diagnostic methods for the reliable quantification of HMGB1 in serum and plasma is required for further elucidation of the role of this multifunctional protein as a diagnostic and/or prognostic marker, and as a potential therapeutic target in immune and inflammatory disease. A role for HMGB1 in chronic viral hepatitis has not yet been identified. Therefore, in the present study, we explore the relationship between HMGB1 plasma levels and liver fibrosis.
Materials and Methods
We retrospectively included 67 treatment-naive chronic HBV infection patients who consecutively underwent liver biopsy at our centers (Department of Gastroenterology, Ataturk University Faculty of Medicine, and Department of Infectious Diseases and Clinical Microbiology and Department of Gastroenterology, Erzurum Research and Education Hospital, both tertiary medical centers in eastern Turkey) between April 2008 and May 2010. All patients underwent liver biopsy to determine the stage of fibrosis.
None of the patients in this study had hepatitis C or hepatitis D infections, decompensated liver disorder, autoimmune hepatitis, α1-antitrypsin deficiency, Wilson's disease, a history of excessive alcohol intake, or severe comorbid conditions, such as thalassemia, chronic renal failure, and severe heart failure. None of them received interferon or antiviral therapy before liver biopsy.
In order to minimize individual variations, serum levels of HMGB1 were determined in duplicate by an enzyme-linked immunosorbent assay (ELISA) (HMGB-1 ELISA Kit; USCNLIFE Science & Technology Co., Ltd. Wuhan, China). The sensitivity of these assays and the detection range were 3.5 pg/mL and 12.5–800 pg/mL, respectively. Serum samples from the time of liver biopsy, which had been stored at −20°C, were analyzed with PCR using the Qiagen HBV PCR kit (Qiagen, Hilden, Germany) according to the manufacturer's instructions. Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were quantified by automatic biochemical analyzer. HBsAg, HBeAg, anti-HBe, anti-hepatitis C virus, and anti-hepatitis D virus were tested for with ELISA kits (DIA.PRO Diagnostic Bioprobes S.r.l., Milano, Italy).
After written informed consent was obtained, each patient without contraindications for liver biopsy received an echo-guided percutaneous liver biopsy from the right hepatic lobe. The liver histology was evaluated by a single experienced pathologist who was blinded to the clinical status of each patient. Liver biopsies were evaluated before therapy by using the Knodell scoring system in all 67 patients (11). Twenty-seven healthy volunteers were recruited as controls. The control group was made up of live kidney transplant donors at our hospital who participated voluntarily in the study.
Continuous data are expressed as the mean ± standard deviation and were analyzed using Student's t-test. Categorical data were expressed as counts and percentages and analyzed by the chi-square test. Correlations among the study variables were tested by Pearson's correlation coefficient. Multiple linear regression analysis was used with fibrosis scores as dependent variables to allow adjustment for age, gender, ALT, HBV viral count, and serum HMGB1 levels. All calculations were performed using SPSS v.11.0 (SPSS Inc., Chicago, IL), with the level of significance set as a two-tailed p < 0.05. Area under the receiver operating characteristics curve (AUROC) was used to illustrate the diagnostic ability of the HMGB1 serum level to distinguish between low fibrosis (fibrosis score 1–2) and high fibrosis (fibrosis score 3–4).
Results
Individual characteristics of the patients and controls are shown in Table 1. HMGB1 serum levels and ALT values were significantly higher in patients with chronic HBV than in controls. In addition, HMGB1 serum levels were significantly higher in patients with low fibrosis (fibrosis score 1–2) compared to those with high fibrosis (fibrosis score 3–4). The HMGB1 levels in patients with chronic HBV and in controls are depicted in Fig. 1. No significant differences were noted in HBV-DNA and ALT values between patients with low fibrosis and those with high fibrosis.

Box plot demonstrating the serum high-mobility group box 1 (HMGB1) levels in normal controls and patients with low-fibrosis and high-fibrosis hepatitis B.
Patients versus controls: p < 0.05.
Low fibrosis versus high fibrosis: p < 0.05.
HBV, hepatitis B virus; HMGB1, high-mobility group box 1; ALT, alanine aminotransferase; NS, not significant; NC, not calculated.
Considering the entire study population, serum HMGB1 levels were positively correlated with ALT (r = 0.35; p = 0.001). However, serum HMGB1 levels were not correlated with HBV-DNA (p > 0.05). In a multivariate regression model, after allowance for potential confounders, serum HMGB1 levels were found to be a significant independent predictor of the degree of fibrosis (β = −0.029, p = 0.002).
The AUROC curve of HMGB1 for distinguishing between low fibrosis and high fibrosis was 0.754. For a cutoff value of 60 pg/mL, the sensitivity was 0.54, the specificity was 0.86, the positive predictive value was 0.68, and the negative predictive value was 0.77 (Fig. 2).
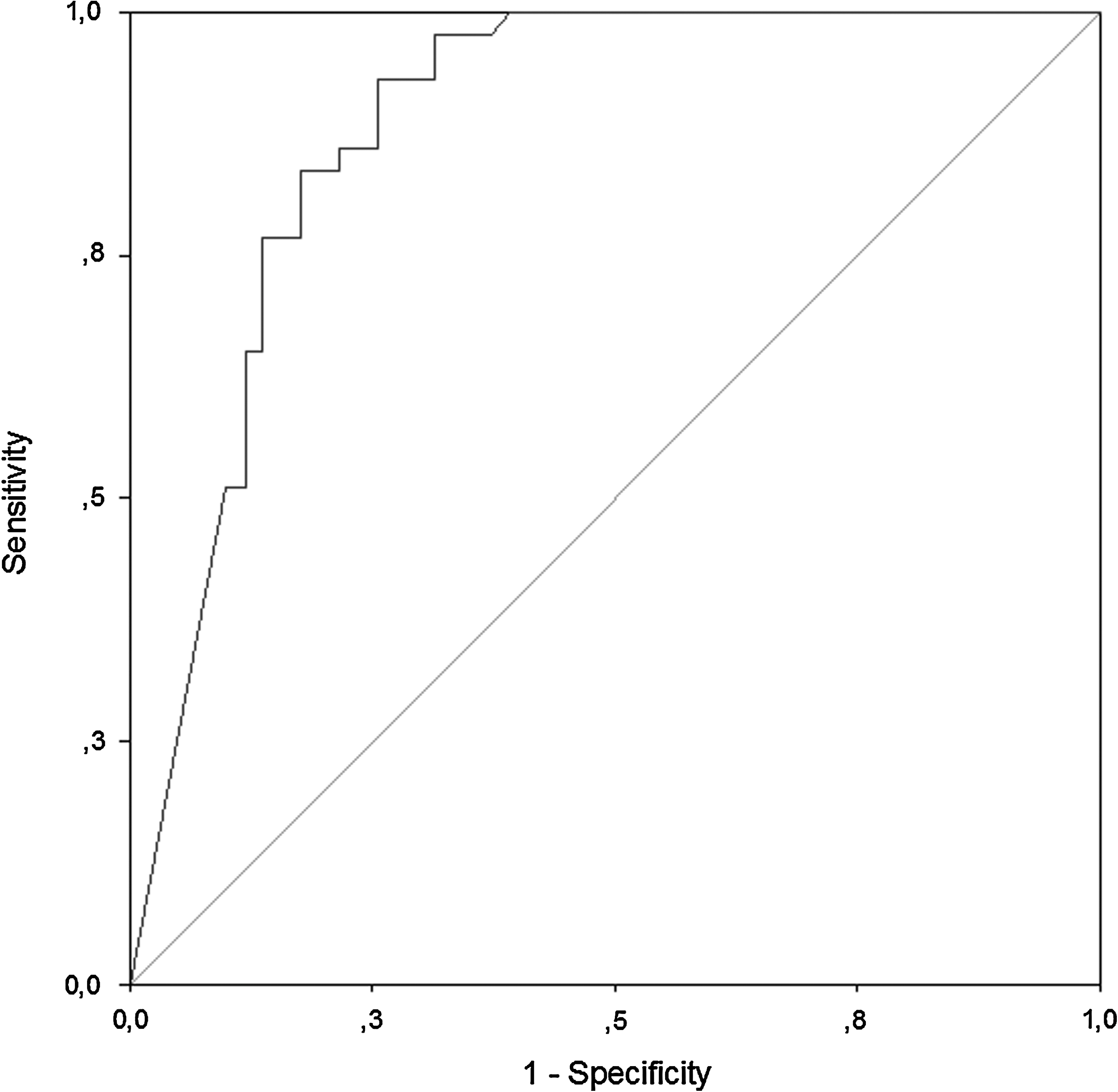
Receiver operator characteristic curve of the serum high-mobility group box 1 (HMGB1) levels for distinguishing between low fibrosis and high fibrosis.
Discussion
Chronic viral hepatitis is often silent, and thus a significant number of persistently-infected individuals remain unaware of infection, even for decades. Although HBV is an immune-mediated response rather than a cytopathic disease, the low-grade liver inflammation seen in chronic active hepatitis can lead to necrosis that is disseminated to the parenchyma and the perilobular regions. In patients with cirrhosis resulting from various etiologies, lymphocytic cell infiltration, along with macrophage accumulation, have been shown to occur within the fibrous bands in the liver (8,12,13,14,15). Co-stimulation of inflammatory and fibrogenic cells is therefore likely to occur, as apoptosis of damaged hepatocytes stimulates the fibrogenic action of liver myofibroblasts (8,16). Fibrosis is usually considered a progressive linear event; however, clinical evidence suggests that fibrotic progression does not always have a fixed speed or follow a linear pattern, but instead can have slower or more rapid phases during its evolution (17). In HBV infection, antiviral therapy with viral clearance has been associated with a significant reduction in fibrosis (8,18).
The liver is a source of many cytokines that may influence liver function. Among the cytokines, increased intrahepatic expression of TNF-α, IL-1A and B, IL-2, IL-6, and IL-8 have been observed in chronic viral hepatitis (8,12). Several anti-inflammatory agents (e.g., IL-10 or TNF antagonists) have demonstrated efficacy in reducing inflammatory liver injury, and yet they may adversely increase viral titers in some hepatitis patients, confirming a dual role for proinflammatory cytokines in the pathogenesis of hepatitis (19).
HMGB1 has been identified as an inflammatory cytokine (3,4). HMGB1 may be released both through active secretion from various cells, including activated monocytes/macrophages, neutrophils, and endothelial cells, and through passive release from necrotic cells (4,5,20,21,22). HMGB1 can directly promote the secretion of proinflammatory cytokines (TNF, IL-1A/B, IL-6, and IL-8), and chemokines (MIP-1A/B) by peripheral blood mononuclear cells (PBMCs) (23,24). In turn, PBMCs also produce different cytokines that are potentially involved in viral-induced liver damage (8,12). HMGB1 acts as a chemoattractant for fibroblasts and endothelial and smooth muscle cells, which are cell types that significantly contribute to wound repair (24,25). Consequently, HMGB1 could directly stimulate fibroblast proliferation and participate in fibrogenesis (5).
HBV infects hepatocytes without incurring direct cell damage (26). Thus both liver disease and viral clearance after infection is thought to be mediated by the cellular immune response to viral antigens (26,27). Hepatocytes can release HMGB1 in response to hypoxic conditions or oxidative stress, and some experimental studies have been carried out to determine if there is a role for HMGB1 in liver disorders (28,29). In experimental models, HMGB1 can also be released in response to polyinosinic-polycytidylic acid (a model of viral infection) (30,31). Ilmakunnas et al. have shown that HMGB1 is a marker of hepatocellular injury in human liver transplantation (20). Acute hepatitis is a viral-induced pathology associated with necrotic cell death that arises either via direct cytotoxic effects of the virus itself, or as a consequence of the inflammatory response to viral infection (19,28). Research carried out with inhibitors of HMGB1 have revealed significant reductions in tissue damage (3,4,20,21).
HMGB1 is known to function as an early-stage mediator in acute local damage, and as a late-stage mediator in sepsis (3). However, no studies have yet been carried out pertaining to the role of HMGB1 in chronic hepatitis. The purpose of this study was to investigate the relationship between serum levels of HMGB1 and the degree of fibrosis in patients with chronic hepatitis. Those with fibrosis levels of 1–2 according to the Knodell score were classified as the low-fibrosis group, and those with scores of 3–4 as the high-fibrosis group. Evaluation of the results revealed significantly higher levels of HMGB1 in low-fibrosis patients. As fibrosis levels rose, so did HMGB1 levels. This relationship was independent of HBV viral load or serum ALT levels. Decreased secretion of HMGB1 from the fibrotic liver may be explained by decreased stimulation of activated monocytes/macrophages, neutrophils, and endothelial cells, and a reduced number of necrotic cells due to the increase in fibrosis. In the follow-up of patients with chronic hepatitis B, a reduction in HMGB1 level may therefore be indicative of a decrease in hepatocyte numbers. In addition, for a cutoff value for HMGB1 at 60 pg/mL, the sensitivity was 0.54, the specificity was 0.86, the positive predictive value was 0.68, and the negative predictive value was 0.77. A cutoff value for HMGB1 of 60 pg/mL could allow HMGB1 to be used as an alternative method to the invasive liver biopsy for following the progression of chronic hepatitis patients. However, as the number of our cases here is small, studies with larger numbers of cases are necessary in order to define more precise cutoff values.
In studies performed to date, the effects of HMGB1 have mainly been examined in the context of systemic disorders and acute infections. Local effects have primarily been studied using in vitro studies, whereas in vivo studies have essentially been overlooked. In addition, little is known about the effect and importance of HMGB1 in chronic inflammation. Extensive studies are still needed in these areas.
Although the importance of HMGB1 in sepsis and acute local infections has been recognized, not enough investigation has yet been made into treatments that involve HMGB1. In rats with extensive liver damage, in one study of neutralizing antibodies against HMGB1, they were found to be effective (21). In addition, glycyrrhizin, a natural triterpene that has been long used in Japan to treat hepatitis, acts in a similar way by binding directly to HMGB1 and possibly impeding its interaction with receptors (24,26). No studies have yet focused on HMGB1 inhibition and its potential as a treatment for chronic liver disorders and liver fibrosis. However, Hamada et al. have reported that HMGB1 inhibition may be beneficial in pulmonary fibrosis (5). We believe that the inhibition of HMGB1 may reduce inflammation, apoptosis, and fibrosis, and may help stop the progression of chronic liver disease.
In the present study, we have shown that HMGB1 is a noninvasive, reproducible, and convenient marker for distinguishing high fibrosis from low fibrosis in chronic HBV patients. Furthermore, we believe that fibrotic progression in chronic liver patients may be prevented via the inhibition of HMGB1, and that this substance can be used to follow-up those undergoing chronic HBV treatment. In this study we did not endeavor to use HMGB1 inhibition as a means of treating chronic HBV infection. In spite of this, the results of our study show that HMGB1 has potential for the prevention and follow-up of fibrosis in chronic HBV patients. Prospective studies using larger numbers of patients should reveal the full potential of HMGB1 for the prevention and follow-up of fibrosis in chronic HBV and other chronic liver disorders. The results of such studies may provide a new agent for the prevention of the progression of fibrosis in chronic HBV, as well as offer new treatment options.
Footnotes
Author Disclosure Statement
No competing financial interests exist.