
Abstract
A patient with well-defined acute HIV infection who developed concomitant pulmonary tuberculosis during the retroviral acute syndrome is reported here. In this patient high levels of T-regulatory cells (Tregs) and a low proliferation response to M. tuberculosis were initially detected, which normalized throughout follow-up. This case calls for the consideration of tuberculosis in patients in the early stages of HIV, and emphasizes the need for further study of the potential causal relationship between Treg cells and the risk of TB reactivation in HIV patients.
Introduction
Regulatory T cells (Tregs) have been implicated in the modulation of immune responses to avoid overactive immunity. In HIV infection, following the initial acute infection, Tregs are upregulated and may contribute to suppression of anti-HIV immunity, promoting acute viremia and facilitating persistent infection, while in chronic infection gradual depletion of these cells allows the development of immune activation (4,5). On the other hand, patients with tuberculosis (TB) present with an upregulation of Tregs, which contributes to decreased production of interferon-γ and IL-10 and suppresses immune responses to TB antigens (6,7). In addition, individuals latently infected by TB present with a rapid depletion of M. tuberculosis-specific Th-1 cells during the acute phase of HIV infection due to direct viral infection of these cells, mostly expressing the surface co-receptor CCR5 (8).
Case Report
In May of 2008 a 33-year-old man was examined because of high fever and night sweats of 5 days' duration, skin rash, and oral and perianal ulcers. He denied having cough or expectoration, or close contact with anyone with cough or confirmed TB. His medical history included frequent use of inhaled cocaine, risky sexual behavior with multiple unprotected sexual relationships with women and men in the past months, syphilis treated 4 y prior, and a positive hepatitis C serology in 2004. Abnormal laboratory values included WBC count 3400 cells/μL, hemoglobin 15.6 g/L, platelets 90,000/μL, AST 74 U/L, and ALT 108 U/L. A chest x-ray and serologic studies (including HIV) were ordered, antipyretics were prescribed, and a follow-up visit was scheduled for the next week. At the next visit the patient's fever and rash had gradually disappeared. The chest x-ray showed a small patchy infiltrate with micronodular shadows in the apical segment of the right upper lobe, but he denied having respiratory symptoms. A MEIA fourth-generation screening HIV test (to detect antigen and antibodies against HIV1/2) was reactive, with a negative Western blot (WB). Two weeks after initial presentation the patient developed a productive cough. The smear test was negative for acid-fast bacilli, and a sample was processed for tuberculosis culture. Twenty-five days later the patient was completely asymptomatic, but a chest computed tomography scan showed a patchy interstitial peribronchial shadow with calcified nodules in the upper right lobe and calcified lymph nodes in the pretracheal retrocaval space. At the same time, the tuberculosis skin test was negative, and a new WB showed gp160 and p24 bands. Baseline HIV-RNA viral load (bDNA) and CD4 count were 62,679 copies/mL (4.79 log10) and 419 (25%) cells/μL, respectively. At 38 days after the beginning of TB symptoms and sputum collection (53 days after the first evaluation at the emergency department), the sputum culture developed Mycobacterium tuberculosis that was sensitive to first-line drugs. That same day, the patient started 9 months of conventional treatment for TB, which was completed successfully. While on TB treatment, he maintained a consistently low viral load and high CD4 counts, and therefore antiretroviral therapy was not initiated. In June 2009, with a CD4 count of 357 cells/mm3, the patient started HAART, which he continues today. He has remained asymptomatic since then, and his recent laboratory values are viral load <50 copies/mL, and CD4 count 481 cells/mm3.
Percentages of Tregs were determined by peripheral blood flow cytometry using anti FoxP3, CD25, and CD4 antibodies as previously described (6). Initially (concomitantly with HIV seroconversion and the development of TB symptoms), the frequency of Tregs was higher and decreased over time. Concurrently, the proliferation in vitro of peripheral blood mononuclear cells to M. tuberculosis H37Rv strain [determined using the CFSE dilution method as described elsewhere (7)] was undetectable, although it showed a transitory increase after starting TB treatment (Fig. 1). The expression of CD38 and HLA-DR molecules on CD4 and CD8 cells remained high throughout follow-up, especially on CD8 T-lymphocytes (the median percentage of CD8+CD38+HLA-DR cells was 34%).
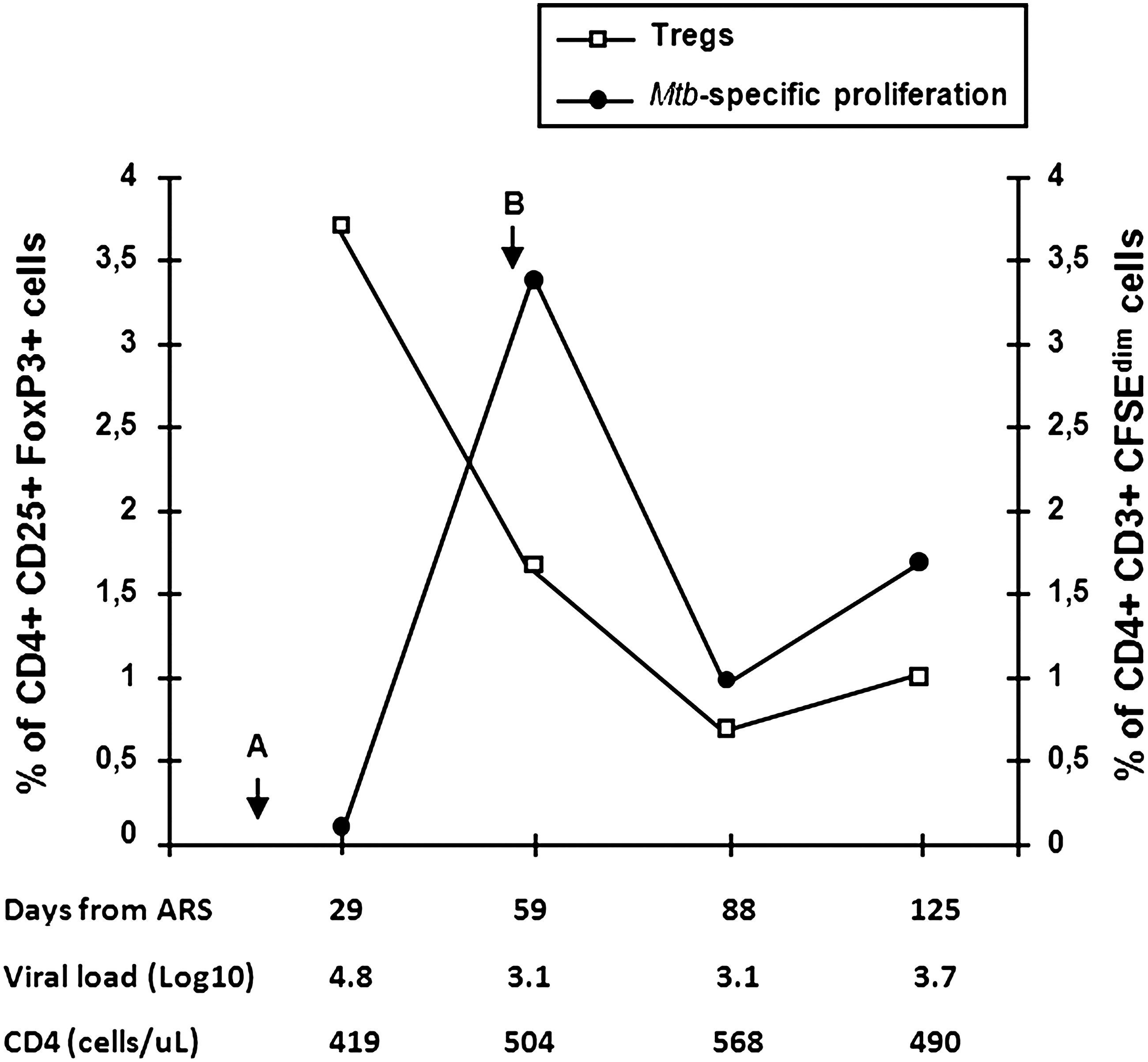
Frequency of Treg lymphocytes and proliferation responses to M. tuberculosis. Percentages of Treg lymphocytes were determined in peripheral blood by flow cytometry using anti-FoxP3, CD25, and CD4 antibodies. The proliferation of peripheral blood mononuclear cells to the M. tuberculosis H37Rv strain was determined in vitro in CD3+CD4+ lymphocytes using the CFSE dilution method. Tregs, MTB-specific proliferation, viral load (b-DNA), and CD4 count (flow cytometry) are shown for each follow-up sample (ARS, acute antiretroviral syndrome; arrow A indicates sputum collection, and arrow B initiation of TB treatment).
Our patient had a well-documented acute HIV infection. In addition, the clinical course of tuberculosis, the anatomic localization, and the radiology support the diagnosis of post-primary TB rather than a new infection.
Our patient is interesting for two reasons: (1) to the best of our knowledge, this patient is the first reported case of acute HIV infection and concomitant pulmonary TB; (2) in this patient we could detect initial high levels of Treg cells, which normalized after TB treatment. Although speculative, it seems plausible that immune dysregulation during acute HIV infection, in particular upregulation of Treg cells, may have contributed to a tolerant state (i.e., a negative TST and low proliferative responses to M. tuberculosis despite relatively preserved CD4 counts) that may have favored the reactivation of TB.
Conclusions
This case underlines the need to explore the role of Tregs, both in HIV-TB co-infected patients, and in the small subset of HIV patients who develop opportunistic infections during the acute phase of infection.
Patient Consent and Ethical Committee
This patient, who is participating in the Argentinean HIV seroconverters cohort “Grupo Argentino de Seroconversion (Site Fundación Huésped),” has read and signed the informed consent form for this cohort. In addition, the patient signed a specific consent form to publish this article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Authors' Contributions
O.S. conceived of the study and drafted the manuscript, M.F.Q. participated in the study design and carried out immunological studies, M.E.S. followed the patient and collected samples, G.T. participated in the immunological studies, and H.S. and P.C. participated in the coordination, analysis, and interpretation of the data. All authors read and approved the final manuscript.
Author Information
Omar Sued is currently working as regional advisor in HIV treatment and care at the Pan American Health Organization, Washington, D.C.
Acknowledgments
We are in debt to Dr. Oscar Bottasso from the Instituto de Inmunología, Universidad Nacional de Rosario, Argentina for his valuable comments, and to Drs. Sara Kaufman and Héctor Pérez from Hospital Fernández, Buenos Aires, Argentina, for their contribution to the clinical management of the case.
This work was partially funded by the Fogarty Training Program (AITRP grant # 5D43 TW0010137), Agencia Nacional de Promoción Científica y Tecnológica (ANPCyT) (PICT 34.271 to M.F.Q.), and the University of Buenos Aires (UBACyT X631 to M.F.Q.).