
Abstract
Chikungunya virus (CHIKV) has caused large outbreaks worldwide in recent years. Acute-phase CHIKV infection has been reported to cause mild to severe febrile illness, and in some patients, this may be followed by long-lasting polyarthritis. The mainstay of treatment includes nonsteroidal anti-inflammatory drugs and other disease-modifying agents, the use of which is based on the assumption of an immunological interference mechanism in the pathogenesis. The present study has been designed to generate preliminary evidence to test this hypothesis. The levels of 30 cytokines were estimated in serum samples of acute CHIKV-infected patients, fully-recovered patients, patients with chronic CHIKV arthritis, and controls, using a quantitative multiplex bead ELISA. The levels of the proinflammatory cytokines IL-1 and IL-6 were elevated in acute patients, but IFN-γ/β and TNF-α levels remained stable. IL-10, which might have an anti-inflammatory effect, was also elevated, indicating a predominantly anti-inflammatory response in the acute phase of infection. Elevation of MCP-1, IL-6, IL-8, MIP-1α, and MIP-1β was most prominent in the chronic phase. These cytokines and chemokines have been shown to play important roles in other arthritides, including epidemic polyarthritis (EPA) caused by Ross River virus (RRV) and rheumatoid arthritis (RA).The immunopathogenesis of chronic CHIKV arthritis might have similarities to these arthritides. The novel intervention strategies being developed for EPA and RA, such as IL-6 and IL-8 signaling blockade, may also be considered for chronic CHIKV arthritis.
Introduction
Chikungunya virus (CHIKV) is the prototype of the alphavirus genus of the family Togaviridae, which contains, in addition to alphavirus, the genus rubivirus. CHIKV was first reported in Africa as the causative agent of an epidemic in Tanzania, the erstwhile southern province of Tanganyika (34). CHIKV is transmitted by Aedes mosquitoes (mainly A. albopictus and A. aegypti). The virus has a 12,000-nucleotide linear positive-sense single-stand RNA genome containing two ORFs that encodes four non-structural, two structural, and two small proteins (E3 and 6K) (31,32).
Infection by CHIKV induces mild to severe disease characterized by fever, myalgia, arthralgia, rash, and headache (28). After the acute phase, polyarthritis may persist for several months to years (32). It has been suggested that this joint pain is similar in nature to that caused by the related alphavirus, Ross River virus (RRV) (24). At present there is neither any specific and effective therapy for CHIKF, nor any approved vaccine for its prevention, though a DNA vaccine construct developed recently appears to be promising (40). Treatment is mostly limited to symptomatic treatment. The pathophysiology of CHIKV infection and the basis for disease severity are incompletely studied. CHIKV replicates in vertebrates as well in insect hosts. The tropism of CHIKV for muscular satellite cells, which are considered to be the reservoir of the virus, may partially explain the long-lasting symptoms seen after CHIKV infection (28). Cytokines and chemokines could be important factors that influence the immunopathology of CHIKV infection. Although IL-2, IL-10, and IFN-γ have been implicated in the pathogenesis of CHIKV, only limited studies have been conducted on the cellular damage and the pathway leading to the secretion of these factors (17). In view of this gap in the knowledge about the immune pathology of CHIKV infection, we undertook the present study as a continuation of our earlier study (22), to further understand the immunobiology behind the chronicity that leads to bony erosion in patients with CHIKV infection. This study attempts to assess the role of various cytokines in the pathogenesis of CHIKV arthropathy by studying the levels of these cytokines in the serum of patients who had different clinical outcomes upon CHIKV infection.
Materials and Methods
Study subjects and specimens
Patients were recruited during an outbreak of CHIKF in the Dakshina Kannada District of Karnataka in India during early 2008 (21). Patients with complaints of fever and joint pain who visited a primary health center (PHC) in the area were screened for anti-CHIKV IgM antibodies using an ELISA test developed at National Institute of Virology, Pune, which had shown high specificity in in-house evaluation (11,44). Patients were interviewed and clinically examined by a physician at the time they reported to the PHC, and several times thereafter for a period of 10 mo. MRI images were obtained for some of the patients who had persistent joint pain, the findings of which have been reported earlier (22). The cohort of patients infected with CHIKV during the epidemic included those with varying severity and chronicity of symptoms. Twenty-two patients from this cohort were included in the present study and were divided into three groups based on their stage of illness and chronicity of symptoms. Six patients with acute illness formed group 1, and another six patients who had acute illness but recovered without chronic manifestations comprised group 2. Group 3 included 10 patients with chronic joint pain that persisted up to 10 mo post-infection. In addition, six apparently healthy individuals negative for CHIKV IgM on ELISA were included as controls. Blood samples were collected from the patients with acute illness (group 1) 5–7 d after the onset of symptoms, and from chronic and recovered patients (groups 2 and 3) during the 10th month after infection. Blood samples were collected from controls as well. Serum was separated and preserved at −80°C until processing.
Multiplex cytokine assay
The concentration of 30 parameters, including cytokines, chemokines, and growth factors present in the serum samples, were estimated using the Human Cytokine 30 plex Kit (cat. no. LHC6003; Invitrogen, Carlsbad, CA) following the manufacturer's instructions. Beads with defined spectral properties conjugated to analyte (cytokine)-specific capture antibodies and 25 μL of 1:2 diluted serum samples were pipetted into the wells of a micro-titer plate supplied with the kit. Standards of known analyte concentrations were included for each parameter assayed. The plate was incubated for 2 h to allow binding of the capture antibodies to the specific cytokine. After washing the beads, analyte-specific biotinylated detector antibodies were added and incubated with the beads for 1 h. During this period, the analyte-specific biotinylated detector antibodies recognized their epitopes and bound to the appropriate immobilized analyte. After the removal of excess biotinylated detector antibodies, streptavidin conjugated to the fluorescent protein R-phycoerythrin (streptavidin-RPE), was added and incubated for 30 min to form a four-member solid phase sandwich. The levels of cytokines were analyzed using the Luminex 100™ instrument. The cytokines that were assayed included GM-CSF, IL-1β, IL-1RA, IL-6, IL-8, TNF-α, IFN-γ, IL-2, IL-2R, IL-4, IL-5, IL-10, IFN-α, IL-7, IL-12p40/p70, IL-13, IL-15, IL-17, eotaxin, IP-10, MCP-1, MIG, MIP-1α, MIP-1β, RANTES, EGF, HGF, FGF-basic, G-CSF, and VEGF (Table 1).
This table summarizes the median levels of 12 cytokines that showed a statistically significant difference in the distribution between any two groups of study subjects. The differences in the distributions of the remaining 18 parameters between any pair of groups of study subjects were not statistically significant. Among the cytokines/chemokines that showed significant difference between groups, IL1-receptor antagonist (IL1-RA), IL2-R, IL-6, IL-8, IL-10, IP-10, MIG, and MCP-1 showed higher levels in patients with acute CHIKF compared to controls. The levels of IL-1β, IL-5, MIP-1α, and MIP-1β did not vary much in acute patients compared to controls. The levels of G-CSF and RANTES were lower among acute patients than in controls.
Statistical analysis
The distributions of the parameters among the four groups of study subjects were studied using dot plots with median values. The difference in the median values of the parameters between pairs of groups was tested using a non-parametric test (Mann-Whitney U test). p Values <0.05 were considered statistically significant. Data are presented as the mean ± SEM calculated from triplicate samples from each experimental group.
Results
Several animal and human studies have shown that CHIKV replicates in the skin before disseminating into the liver and bones, causing arthritic joints (7). Newborn and young mice, with their high sensitivity to CHIKV infection, are valuable models for studying CHIKV pathogenesis (7). For example, a study using a highly pathogenic mouse model lacking the type I IFN receptor (lfnar−/−) revealed the importance of IFN in conferring increased susceptibility of host cells to CHIKV (7), as compared to other regulatory protein knock-outs, Cardif−/− or MyD88−/− mice. Following numerous animal studies, research on CHIKV cellular tropism in humans has attained only limited success. In vitro replication of the virus in human epithelial and endothelial cell lines and in fibroblasts and macrophages has been reported (37). Here we have conducted a comparative study of the cytokine profile triggered by CHIKV in acutely-infected, recovered, and chronically-infected patients.
Study groups
The age of the study subjects ranged between 25 and 55 y, with a mean age of 34.5 y (30.5 y for controls, 34.5 y for patients with recovered acute CHIKF, and 41.5 y for patients with chronic CHIKF). The difference in the mean ages of the controls (30.5 y) and the study subjects (37.5 y) was not statistically significant (t = −1.574, p = 0.128). No age matching was done while selecting the patients in each group, and therefore the higher mean age of patients with chronic arthritis reflects the higher chance of older patients to develop chronic manifestations after CHIKV infection.
Cytokine responses in the acute phase
The typical antiviral response in humans is characterized by the induction of cytokines such as IFN-α/β, IFN-γ, IL-12, and IL-18, and the activation of macrophages, NK cells, dendritic cells, neutrophils, and complement (16). We measured the cytokine levels in blood samples taken from acutely-infected patients 5 d post-infection, and compared the levels with uninfected controls. Although IL-10 and IL-4 are not usually upregulated in viral infections, we found that the median IL-10 level was higher in acute patients compared to controls (Fig. 1). However, no rise in the level of IL-10 was observed in recovered and chronic patients. IFN-α/β upregulation occurs very early in the course of CHIKV infection (16), and by day 5 post-infection the levels return to baseline. The blood samples from acute patients were collected 5–7 d after the onset of symptoms, and by that time, IFN levels might have declined to baseline levels. IL-10 has been shown to have a negative role in immunity against West Nile virus infection (2), and perhaps a similar mechanism might also be responsible for the observed lack of any rise in the levels of IFNs.

Cytokine levels in acutely infected patients and controls. (
The inflammatory cytokine TNF-α levels were unchanged in patients with acute infections, but the other inflammatory cytokines such as IL-1β and IL-6 were found to be significantly high compared with healthy controls. This indicates that the signals of inflammatory response might have been mediated by IL-1 and IL-6 with the absence of TNF-α in patients suffering with CHIKV infection.
The median level of the proinflammatory cytokine IL-6 was significantly higher among acute patients compared to controls. While in patients who recovered fully its level returned to baseline, in patients with chronic arthritis the level showed a further increase by the 10th month, indicating a strong association with chronic arthritis. IL-6 has been shown to play a critical role in both the initiation and perpetuation of immunological dysfunction and inflammatory responses in various forms of autoimmune arthritis (20). Clinical trials have shown compelling evidence that neutralizing IL-6-mediated signaling provided significant clinical benefit in patients with RA (20). The clinical and radiological features of CHIKV arthritis closely resembled those of RA (22), and therefore IL-6 signaling blockade could potentially be an intervention strategy for CHIKV arthritis. IL-6 has an anti-inflammatory effect also, which is mediated through its inhibitory effect on TNF-α and IL-1β, and activation of IL-1RA and IL-10 (30).
Increased levels of IL-10 and IL-1RA were observed among acute patients in the present study, which perhaps indicates that the anti-inflammatory activity of IL-6 was coming into play in these patients. IL-10 and IL-6 are the two cytokines produced from macrophages, and they have two opposing functions, which depend on the absence/mutation of the SOCS3 binding site in gp130 of the SOCS3 gene in the macrophage; however, experimental studies showed that IL-6 induces an anti-inflammatory response (43). Increased levels of IL-6 may also partially explain the apparent absence of any TNF-α response in these patients.
Significantly increased levels of IL-1RA are observed in both acute (534.9 pg/mL) and chronic (594.4 pg/mL) patients suffering from CHIKF compared with healthy controls. This cytokine is mainly associated with T-cell activation and is secreted by activated T cells (35), and it mediates the immunological action against CHIKV.
There was a large increase in the level of IP-10 and a moderate increase in the level of MIG in acute patients. Both these cytokines are chemoattractants of monocytes, macrophages, T cells, NK cells, and dendritic cells, and they promote adhesion of T cells to endothelium. Elevated levels of these chemokines that are associated with the Th-1-type reaction, along with elevated levels of the anti-inflammatory cytokine IL-10, suggest a predominantly anti-inflammatory cytokine response in acute CHIKV infection, as has been reported earlier (26).
Neurological complications have been reported occasionally during CHIKF (6). MIG is important in contributing to host defense by promoting a protective Th-1 response against viral infection of the central nervous system (18). The present study showed elevated MIG levels in acute patients, and perhaps this chemokine provides defense against CHIKV infection of the CNS.
Cytokines and chemokine response in chronic CHIKV arthritis
The distribution of cytokines that were different among controls and patients with chronic arthropathy following CHIKV infection was analyzed. As shown in Fig. 2, six cytokines, namely IL1-RA, IL-6, IL-8, MIP-1α, MIP-1β, and MCP-1, had higher levels in patients with chronic arthropathy following CHIKV infection compared to controls. As in the case of acute patients, the levels of IL1-RA and IL-6 were elevated in patients with chronic infection as well. However, as described above, the level of IL-6 observed in chronic patients was much higher than that in the acute patients, indicating its strong association with chronic arthritis in CHIKV-infected patients.
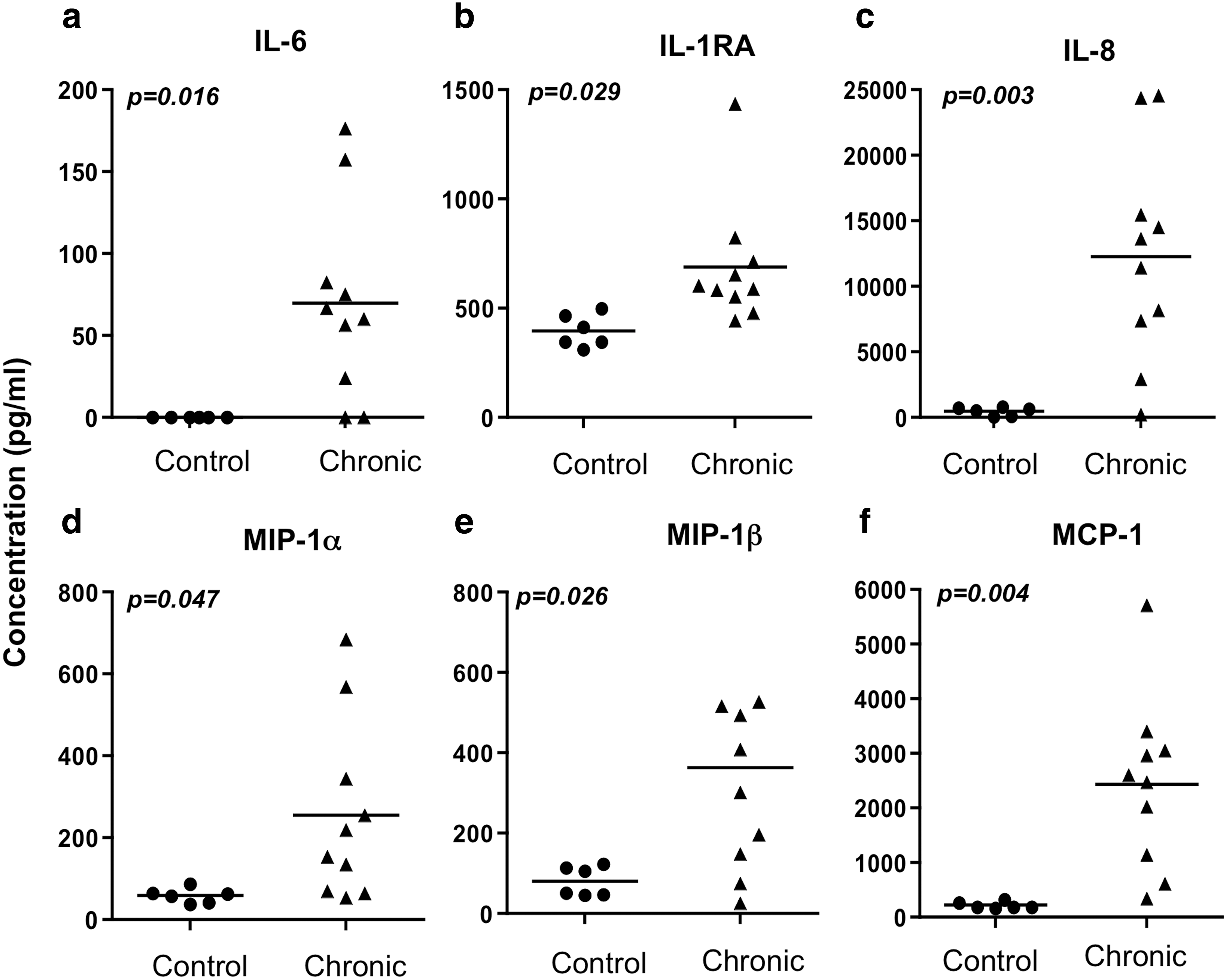
Cytokine levels in chronically infected patients and controls. (
The levels of IL-8 and MCP-1 were elevated many-fold in patients with chronic arthritis compared to controls, acute patients, and patients who completely recovered. Elevated levels of IL-8 in serum and synovial fluid of RA patients have been reported in several studies (13). IL-8 inhibition by monoclonal antibodies has been suggested as a potential treatment strategy in RA, though phase II trials thus far have not yielded promising results (14). Macrophages and fibroblasts infected with Ross River virus (RRV) have been reported to upregulate MCP-1 and IL-8 mRNA (23), indicating that IL-8 may be playing a similar role in EPA due to the alphavirus RRV as well. MCP-1 is implicated in other viral arthritides, including measles virus (42) and caprine arthritis encephalitis virus (29). Elevated levels of MCP-1 in serum and synovial fluid of active RA patients have also been reported (38). In the present study, MIP-1α and MIP-1β levels were also significantly elevated in patients with chronic arthritis as compared to controls and patients in the other groups. MIP-1α and MCP-1 have been identified as the most prevalent chemokines detected using adjuvant or collagen-induced arthritis models in rodents (4). Studies by Toh et al. (41), and Orhan Sezer (27), showed that these cytokines (MCP-1 and MIP-1α) play an important role in bone resorption, and inhibiting these chemokines using antibodies showed an improvement of artificially induced arthritis in rats. Recent studies on non-human primates suggest that there is an increased expression of MCP-1 during acute infection (16), but joint pathology could not be observed (39).
Distributions of the levels of cytokines among patients recovered from CHIKF without chronic arthritic symptoms, and among those with chronic arthropathy following CHIKF, are shown in Fig. 3. The levels of all the cytokines that were elevated in patients with chronic arthritis, namely IL1-RA, IL-6, IL-8, MIP-1α, MIP-1β, and MCP-1, returned to levels similar to those seen in controls, further indicating that the elevations in these cytokines are specific to patients who develop chronic arthritis.
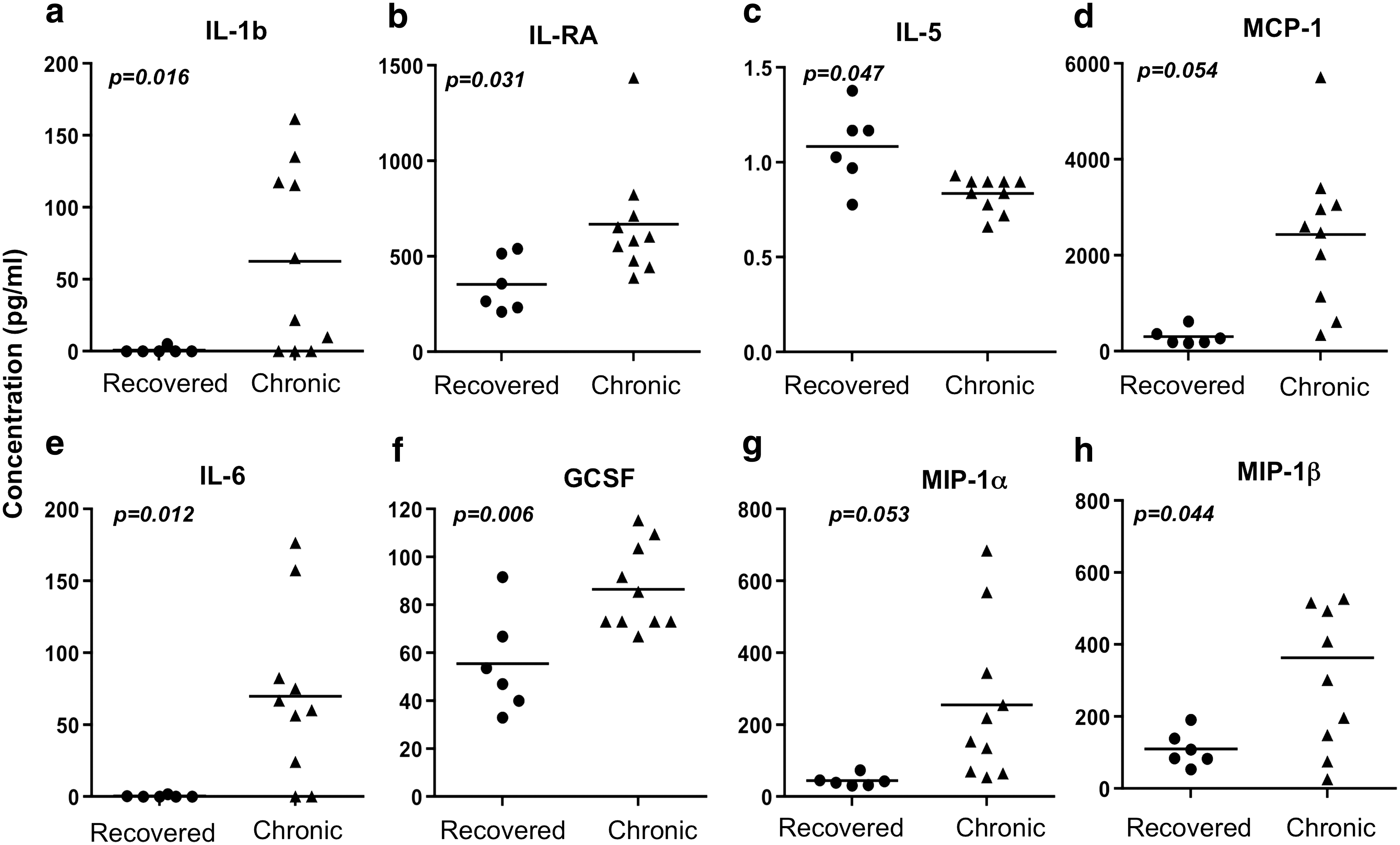
Cytokine levels in patients recovered from CHIKF without chronic arthritic symptoms, and those with chronic arthropathy following CHIKF. (
In the present study elevated levels of IL-5 were observed in patients who suffered and recovered from CHIKV infection, and suggested that IL-5 may have a function in bone homeostasis. A study of transgenic mice overexpressing IL-5 has indicated that IL-5 plays a role in bone homeostasis, although it is not clear whether this cytokine has a direct effect or if it is mediated through eosinophils or B cells (19).
Platelets are a major reservoir of RANTES in the peripheral circulation (8). Severe CHIKF has been characterized by thrombocytopenia. Thrombocytopenia can also reduce levels of circulating RANTES. Low levels of RANTES correlate with disease severity and mortality in individuals with severe malaria (12). In the present study, low levels of RANTES were observed in chronic patients, higher levels were seen in acute patients, and even higher levels were seen in recovered patients, compared with the healthy control group. These observations are in agreement with the above hypothesis, and we assume that the low levels of RANTES may represent the presence of virus/viral particles in the body, which may be the reason for this long-term chronicity.
Conclusions
The trend over the past few years indicates that CHIKV has the potential to spread uncontrollably and cause large outbreaks with high attack rates (10). Although mortality rarely occurs, a significant proportion of infected persons suffer from prolonged and crippling arthritis, resulting in functional limitations (36,22). Since no specific antiviral therapy has been shown to be effective in shortening the duration of infection or in preventing or reducing the severity of arthritic symptoms, the mainstay of treatment is nonsteroidal anti-inflammatory drugs (NSAIDs). The preventive strategy is limited to vector control measures, which are very effective because of the peri-domestic breeding habits of the vector mosquito A. albopictus. In this situation, morbidity reduction through proper case management is of great importance. Current strategies using NSAIDs and disease-modifying agents are not completely effective. Other disease-modifying agents such as chloroquine and methotrexate have also been tried with varying success (5). These disease-modifying agents are immune-modulators, and their empirical use is based on an assumption that CHIKV arthritic lesions are at least partly mediated by immunological mechanisms. The present study was designed to generate preliminary evidence to test this hypothesis.
The cytokine response seen during the acute phase of the disease suggests a predominantly anti-inflammatory response to CHIKV infection. The cytokines IL-6 and IL-8 and the chemokines MCP-1 and MIP-1 appear to play an important role in the pathogenesis of chronic arthritis in CHIKV infection. The cytokine and chemokine response observed in chronic CHIKV arthritis patients has many features in common with that of RA and EPA caused by RRV. Perhaps the evolving intervention strategies targeting cytokine and chemokine pathways in RA and EPA, such as IL-6 and IL-8 blockade, might be applicable for chronic CHIKV arthritis as well.
We believe that these findings may aid in satisfying the urgent need to develop novel treatment strategies against this scourge. A clear understanding of the immune pathogenesis of this disease will help in devising new therapeutics.
Footnotes
Acknowledgments
The research was supported by funds from the Department of Biotechnology (BT/PR9372/Med/29/24/2007).
Author Disclosure Statement
No conflicting financial interests exist.