
Abstract
We tested the plasma of 51 HIV-1-infected children (23 naïve and 28 ART treated) for neutralization against five primary isolates (PIs) generated from adult Indian HIV-1-infected patients. The plasma exhibited neutralization potential with significantly higher neutralizing antibody titers in ART-treated children than naïve children against three out of five PIs (p<0.0001). Further, in treated children, neutralizing antibody titers were higher in those children with suppressed viremia (<1000 RNA copies/mL) than non-suppressors against two of the three PIs. We report here for the first time the neutralization potential of the plasma of HIV-1-infected Indian children.
Introduction
Neutralizing antibodies capable of neutralizing primary isolates are produced in HIV-1-infected individuals to a variable extent (1,20). Limited information is available on the neutralizing antibody responses in HIV-1-infected children. A greater understanding of HIV-1-specific immunity in HIV-1-infected children is important to develop interventions to reduce transmission and to modify disease progression, which may supplement existing antiretroviral drug regimens (5). Effective antiretroviral therapy (ART) offers hope to prevent the complications associated with HIV-1 infection. Treatment of HIV-1-infected children with antiretroviral drugs has many advantages. These include better immune recovery, reduction of serious bacterial infections including tuberculosis, which is prevalent in India and other resource-limited settings, and better growth and development of the child (21). In this scenario, the effect of ART on the neutralizing antibody response in HIV-1-infected children is not yet known. To date, there are no reports on the neutralization efficiency of the plasma of HIV-1-infected Indian children. Our objective was to characterize the neutralization efficiency of the plasma of HIV-1-infected Indian children, and correlate it with virological and clinical parameters.
Materials and Methods
We recruited 51 HIV-1-infected children for this study from the Pediatric Chest Clinic of our Institute after obtaining written informed consent from their parents/guardians. Children less than one and a half years old were excluded from the study, as they may contain maternally-derived antibodies. Clinical and demographic data were recorded using a structured questionnaire. Blood samples of these children were collected in EDTA Vacutainers. Plasma was separated by centrifugation at 300×g and stored in aliquots at −80°C until use. All the plasma samples were heat inactivated at 56°C for 1 h before their use in the neutralization assays. Viral load (Roche COBAS TaqMan HIV-1 v2.0) and CD4 counts (BD Biosciences, Franklin Lakes, NJ) were determined in these patients. The study was approved by the institute ethics committee.
We tested the neutralization efficiency of the plasma of HIV-1-infected children against five limitedly passaged primary isolates (PIs) and one reference isolate (SF162, obtained from the National Institutes of Health AIDS Research and Reference Reagent Program). We then correlated the neutralizing antibody titers with the treatment status, viral load, and clinical stage. All five primary isolates tested were generated previously in our laboratory from adult HIV-1-infected Indian patients. Sequence analysis of the C2-V3-C4 region of these primary isolates revealed that all of them belonged to clade C (AIIMS53, AIIMS65, AIIMS70, AIIMS126), and AIIMS151). The GenBank accession numbers of these PIs are AIIMS53 GU071081, AIIMS65 GU057986, AIIMS70 GU057985, AIIMS126 FJ940736, and AIIMS151 FJ940737. All of the viruses were expanded in PBMCs isolated from adult healthy seronegative donors for a maximum of two passages.
Neutralizing antibody responses were assessed by neutralization assays using TZM-bl cells with a tat-responsive luciferase reporter gene as described previously (13). Briefly, 200 TCID50 of each virus (50 μL) was pre-incubated with different dilutions (ranging from 1:100 to 1:20,000) of heat-inactivated plasma (50 μL) in DMEM for 1 h at 37°C in 96-well flat-bottom tissue culture plates. Then, freshly trypsinized TZM-bl cells (1×104 cells in 100 μL of complete DMEM) were added to each well. Indinavir sulfate at a concentration of 1 μM and DEAE dextran at a final concentration of 25 μg/mL were added to ensure a single round of infection, and to increase the efficiency of infection, respectively. Cell controls containing cells only and virus control containing virus and cells were put up in the assay. The former serve for background luminescence, while the latter give the maximum luminescence due to infection. Plasma from two healthy children was taken as negative control. After 48 h of incubation at 37°C, 150 μL of the medium was removed from each well, and 50 μL of BrightGlo reagent (Promega Inc., Madison, WI) was added to each well and incubated for 2 min at room temperature. Luminescence was then measured using a Sirius luminometer (Berthold Detection Systems, Pforzheim, Germany). Percent neutralization was calculated for the test wells by dividing the relative luminescence units (RLU) of the test plasma by the virus control. Cell control RLU value was subtracted from the test RLU as background cut-off. The assays were repeated in duplicates at least twice and found to be consistent. Fifty percent neutralization titer (ID50 titer) representing the reciprocal dilution at which there was 50% neutralization against each virus for all the plasma samples was calculated by non-linear regression using the method of least squares. Statistical analyses were done with GraphPad Prism 5.0 software. The Mann-Whitney U test was used to compare the two patient groups. A p value<0.05 was considered significant.
Out of the 51 children recruited, 23 were antiretroviral-naïve and 28 were ART-treated. The majority of the infected children were boys (43 out of 51), with a median age of 8 y (range, 2–16 y). The median age at diagnosis was 4 y (range, 6 mo to 12 y). The median duration of treatment of the children on ART was 3 y (range, 6 mo to 8 y). All the HIV-1-infected children were managed as per national treatment guidelines (19). The CD4 cell counts were comparable for the naïve (median 600 cells/μL, IQR 415–999) and treated (median 640 cells/μL, IQR 378–1051) children (p=0.97). The viral loads of the treated children (median 1373 RNA copies/mL, IQR 47–3945) were less than those of the naïve children (median 3510 RNA copies/mL, IQR 400–40800, p=0.2).
Results
The plasma of children exhibited neutralization potential against the isolates tested (Supplementary Tables 1 and 2; see online supplementary material at
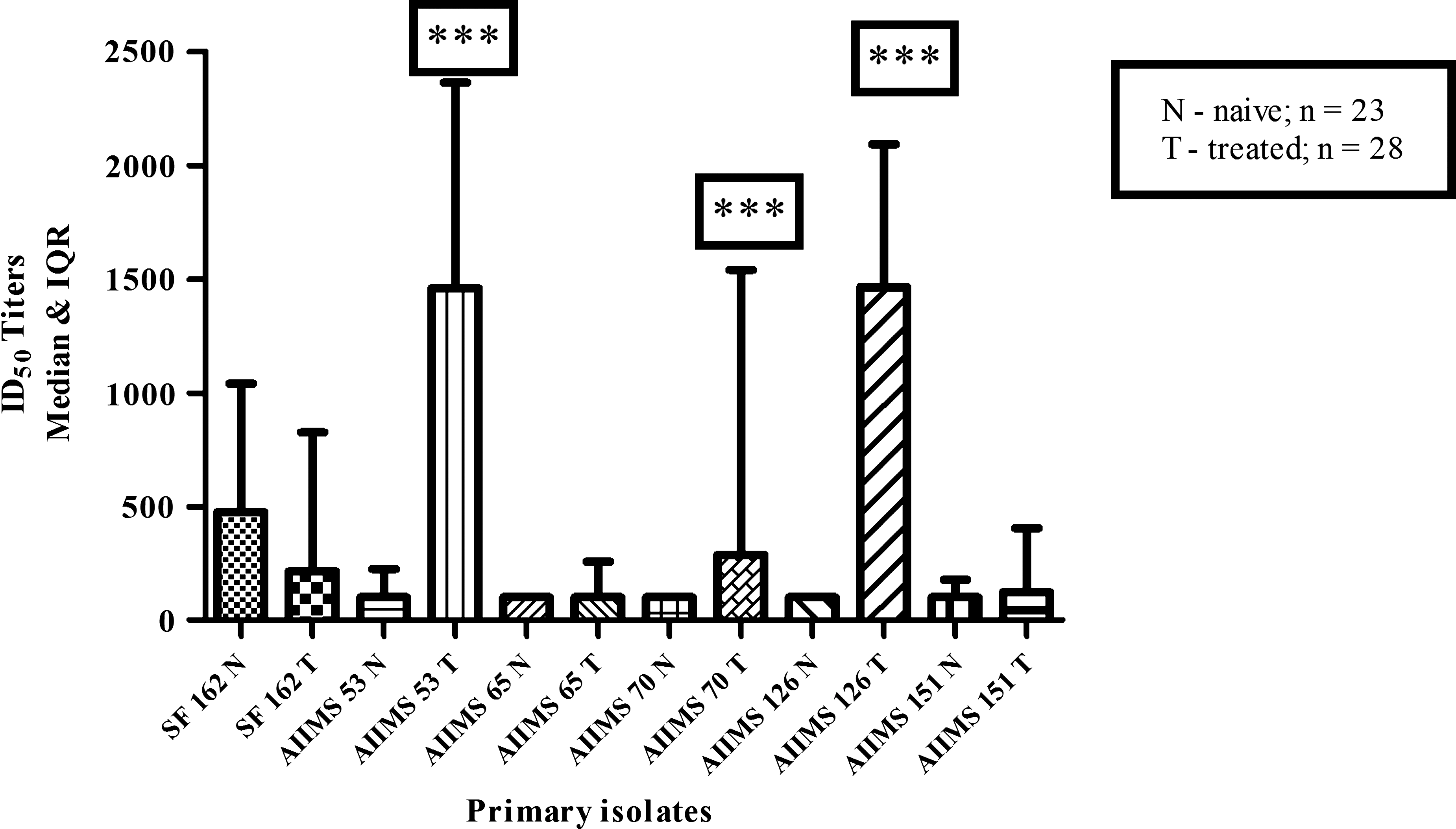
Comparison of the neutralization titers (median ID50) between the naïve and antiretroviral therapy (ART)-treated HIV-1-infected children (***p<0.0001 by Mann-Whitney U test). The bars represent median ID50 titers with inter-quartile range (IQR). Median ID50 titers for naïve and ART-treated children were calculated from the individual ID50 titers of the plasma of each of the children against each of the primary isolates in the respective groups.
To correlate the neutralization titers with the viremic status, we divided the naïve and treated children into naïve suppressors (NS; n=7), naïve non-suppressors (NN; n=8), treated suppressors (TS; n=7), and treated non-suppressors (TN; n=10) based on viral load (suppressors had <1000 RNA copies/mL, and non-suppressors had >1000 RNA copies/mL). Viral load data were unavailable for 8 naïve and 11 treated children. We compared the neutralization titers between the two groups of naïve children, and found that they were comparable (AIIMS53 p=0.27, AIIMS65 p=0.68, AIIMS70 p=0.33, AIIMS126 p=0.62, and AIIMS151 p=0.17). On comparing the neutralization titers between the two groups of treated children, the plasma of TS children exhibited significantly higher neutralization potential against AIIMS70 (p=0.03), and approached significance for AIIMS126 (p=0.09), while they were comparable (AIIMS53 p=0.71, AIIMS65 p=0.94, and AIIMS151 p=0.16) against the rest of the PIs (Fig. 2).

Comparison of the neutralization titers (median ID50) between treated suppressors (TS, n=7, viral load<1000 RNA copies/mL) and treated non-suppressors (TN, n=10, viral load >1000 RNA copies/mL) HIV-1-infected children. The bars represent median ID50 titers with inter-quartile range (IQR). Neutralization titers were higher against two PIs (AIIMS70 and AIIMS126) for the plasma of TS children compared to TN children (*p=0.03, #p=0.09 by Mann-Whitney U test).
The infected children were grouped according to the clinical stage of infection (19). Among the naïve children, 12 belonged to stage 1, 9 belonged to stage 2, and 2 belonged to stage 3. The two stage 3 naïve children were recruited just before they were initiated on ART. Among the ART-treated children, 24 belonged to stage T1, 3 belonged to stage T2, and 1 belonged to stage T3. We correlated the neutralization titers with the clinical stage of infection by comparing asymptomatic (stage 1/T1) and symptomatic (stage 2 and 3/T2 and T3) naïve and treated children. Asymptomatic (stage 1) naïve children were significantly better at neutralizing the AIIMS126 isolate (p=0.02) compared to the symptomatic (stage 2 and 3) naïve children. The neutralization titers were comparable between the two groups of naïve children against the rest of the PIs, and against all of the PIs between treated symptomatic and asymptomatic children who were receiving ART (data not shown).
Discussion
Previous studies conducted in HIV-1-infected children have shown that the presence of neutralizing antibodies to primary isolates correlated with a better clinical status (4,9,24). The levels of neutralizing antibodies, however, could not predict disease progression in HIV-1-infected children (25).
In this study, we found that the plasma of HIV-1-infected children was able to neutralize the heterologous PIs efficiently. We observed significantly higher neutralization titers in the ART-treated children against three out of the five PIs tested compared to naïve children. The presence of antiretroviral drugs in the plasma could affect the neutralization assays by causing “pseudo-neutralization.” One of the earlier studies done in adult HIV-1-infected patients has shown that the presence of ART drugs does not affect the neutralization of primary isolates beyond a 1:50 dilution of the test plasma (2,7). Hence we used different dilutions of the test plasma, starting at 1:100, and ranging up to 1:20,000, as our cohort contained both naïve and ART-treated children. ART results in a decrease in viral load and an increase in the CD4 counts of HIV-1-infected patients. ART leads to a decrease in antibody titers as evidenced by previous studies (8,16,17). Neutralization of lab-adapted isolates by the plasma of ART-treated patients has been shown to be decreased due to the decrease in antibody titers directed against the viral envelope (8,17). We also found lower neutralization titers against the tier 1 isolate SF162 in the treated children (Fig. 1). Neutralization of primary isolates by ART-treated individuals has shown variable results. Kim et al. (2001) found that neutralization of primary isolates was higher in ART-treated individuals with prolonged suppressed viremia (12). Other studies have found that the neutralization titers were decreased in ART-treated individuals with suppressed viremia (3,17). The variation in the results observed could be due to the difference in the primary isolates tested in these studies. We found that among the treated children, those with suppressed viremia had higher neutralizing antibody titers than those with increased viral loads (Fig. 2). This may be suggestive of a better neutralizing antibody response in treated individuals with suppressed viremia than those with increased viral loads, though further confirmation is needed. Alternatively, efficient neutralizing antibodies may help to reduce viremia in these children (11,14,15,22). The present study may not help to ascertain this cause-and-effect relationship. One of the reasons for the better neutralization response in ART-treated children could be due to the priming of B cells by the virus before initiation of ART, which might become activated even by the low levels of viremia due to their restored immune function, or may be due to the removal of some unidentified viral factor whose influence is overcome by the suppressed viremia, as suggested earlier (12,15). The findings reported here need to be confirmed by studying a large number of patients.
For the first time, we have studied the heterologous neutralization efficiency of the plasma of HIV-1-infected Indian children. We did not identify the clade of the infecting virus in these children. Also, the viral load data were unavailable for some children. These constitute the major limitations of this study. The potency and breadth of neutralization needs to be assessed by testing the plasma against a large panel of viruses of different clades.
Footnotes
Acknowledgments
We thank the study participants. This work was supported by a grant from the Indian Council of Medical Research (grant no. HIV/50/137/2010-ECD-II).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.