
Abstract
Common variable immunodeficiency (CVID) is a heterogeneous group of disorders with varied immunologic phenotypes and clinical manifestations. Patients with CVID are mainly characterized by decreased serum immunoglobulin levels, and increased susceptibility to recurrent bacterial infections, autoimmune disorders, and malignancies. Here we present a CVID patient who has developed a clinical polyclonal lymphocytic infiltration phenotype associated with severe and irreversible pancytopenia with unknown etiology. Progressive unilateral loss of vision and cytomegalovirus retinitis indicated the cause of patient's pancytopenia.
Introduction
The management of CVID has improved with immunoglobulin replacement therapy, and prophylactic antibiotics have increased survival of patients in recent decades (14,15). However, this treatment resulted in a higher frequency of non-infectious clinical complications in these patients (16). The main causes of these complications are immune dysregulation, T-cell deficiency, and a breakdown in central and peripheral mechanisms of tolerance induction or maintenance (17,18).
Cytomegalovirus (CMV) is a ubiquitous DNA virus and a member of the Herpesviridae family that frequently causes life-threatening infections in immunocompromised patients (19,20). Although the presence of severe viral infections such as varicella (21), herpes simplex virus (HSV), measles (22), and other chronic enteroviral infections (23) in CVID have been reported, severe CMV disease is an infrequent complication in CVID patients (24). Isolated CMV lymphadenitis, pneumonia, and gastrointestinal involvement have been reported in these patients (24). Here we describe a patient with CVID that presented with CMV infection leading to rhegmatogenous retinal detachment and pancytopenia.
Case Report
The patient is a male with a history of gynecomastia, umbilical hernia, and a lack of tonsils at birth. He is the first child of related parents, with no family history of immunodeficiency. He was fully vaccinated without any complication and was quite healthy until the age of 2 y, when he presented with severe recurrent diarrhea. He experienced recurrent episodes of upper and lower respiratory tract infections such as pneumonia, sinusitis, and otitis media, which required antibiotic therapy and hospitalization. At the age of 4 y, he was referred to the departments of infectious disease and clinical immunology of the Children's Medical Center Hospital for further evaluation. He was diagnosed with CVID based on panhypogammaglobulinemia (low IgG, IgA, and IgM; Table 1), poor responses to vaccines (anti-tetanus antibody=0.1, anti-diphtheria antibody=0.1, and anti-pneumococcal antibody=100 to 120), and after the exclusion of other antibody deficiencies associated with well-defined single gene defects. He received regular intravenous immunoglobulin (IVIG), which resulted in considerable improvement of his respiratory symptoms.
This patient developed photosensitivity, xerodermia, vitiligo, clubbing, splenomegaly, and bronchiectasis during the first 4 y of follow-up. At the age of 8 y, a non-caseating granulomatous lesion was documented in one of his neck's anterior chain lymph nodes, detected by excisional biopsy. The combination of splenomegaly and the granulomatous lesion led to the diagnosis of polyclonal lymphocytic infiltration phenotype in this patient.
At one of his follow-up visits at the age of 12, a complete blood cell count (CBC) showed leukopenia (white blood cells 2100/mm3) with an absolute neutrophil count of 760/mm3. Hemoglobin (Hb) was 11.9 g/dL, hematocrit (HCT) was 30.5%, and platelet count was 85,000 cells/mm3. Further hematological evaluations revealed abnormal cellular immunity, such as a decreased CD4:CD8 ratio and reduced T-cell response to blastogenetic agents. Although the etiology of pancytopenia was unknown, some evidence of autoimmunity-induced splenomegaly and viral-induced pancytopenia were postulated for this patient. There was no evidence of autoantibodies (e.g., antiplatelet antibodies) and Coombs' test was negative. All microbiological assays were negative for microorganisms.
Bone marrow aspiration showed hypocellularity, with increased macrophage numbers with occasional hemophagocytic activity. As on presentation he had lethargy, disorientation, and fever for more than 1 wk, macrophage activation syndrome (MAS) was suspected as a probable reason for the pancytopenia. He was initially treated with steroids, but developed jaundice and hepatitis within a month. Work-up for evaluation of hepatitis showed elevated ALT levels, increased bilirubin levels, elevated LDH levels, and decreased albumin, but the underlying cause was unknown. We continued steroid therapy, but there was no improvement in the condition of the patient. The etiology of his MAS was obscure at that time.
Within 6 mo, he had gradual visual impairment and developed conjunctivitis. Upon ophthalmological investigation, his right eye had hyperopia, and stellate keratic precipitates appeared on the right corneal endothelial surface. Anterior capsular opacity of the lens, a macular pigmented scar, vitreous hemorrhages, retinal hemorrhages in the superotemporal part of the retina with vascular sheathing at the equatorial portion of the fundus, and near-total retinal detachment were confirmed by ultrasound (Figs. 1 and 2); a 2+ relative afferent pupillary defect was detected.

Macular pigmented scar and retinal hemorrhage with perivascular distribution in CVID patient with severe CMV infection.
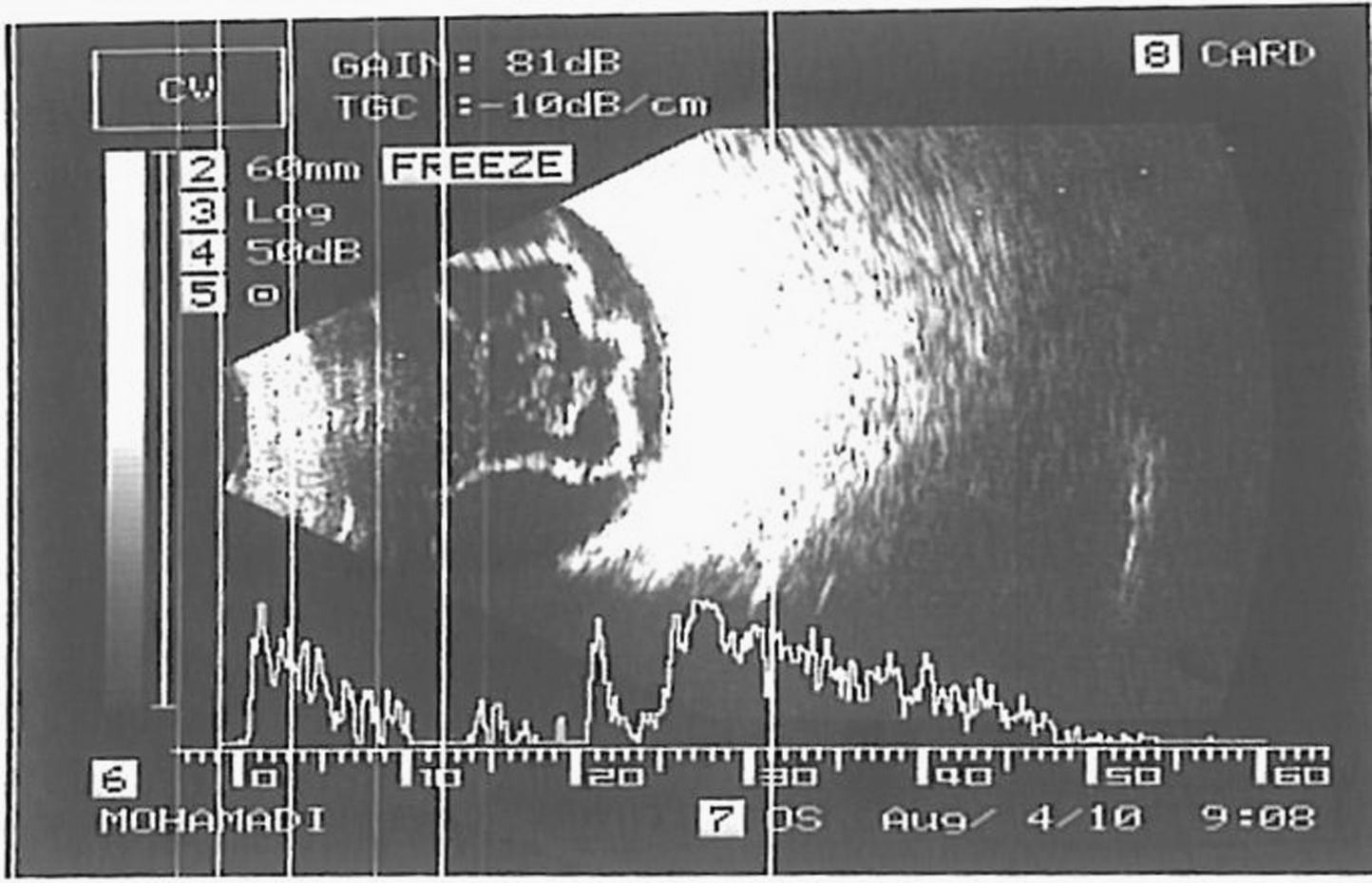
Near total retinal detachment confirmed by ultrasonography in CVID patient with severe CMV infection.
Antibiotics and antifungals were ineffective in improving his clinical condition. DNA of CMV was detected in his plasma, as well as in is aqueous humor, by polymerase chain reaction (PCR) by the fluorescent amplification-based specific hybridization (FLASH) method. The diagnosis of CMV retinitis was made based on the clinical findings seen by an ophthalmologist, and findings of DNA of CMV in the plasma and aqueous humor.
He was treated with daily intravenous ganciclovir for 1 wk and had a vitrectomy done with multi-break retinal detachment and lensectomy with intraocular lens implantation after admission. No active retinitis lesions were found at the time of the surgery. CBC was rechecked to assess the effects of ganciclovir and showed that his pancytopenia had improved. He received a topical antibiotic (chloramphenicol), betamethasone drops, and cycloplegic drops after surgery in a tapering manner for nearly 1 mo. The retina was attached and no visible retinal lesions such as retinitis or other inflammatory disorders were detected 1 mo after surgery. After complete retinal attachment, there was a diffuse pigmentary change in the retina, especially in the midperipheral areas of the retina and along the vessels. His final best corrected vision at 6 mo after surgery was 20/40 after silicone oil removal.
Discussion
Common variable immunodeficiency (CVID) is a clinically and immunologically heterogeneous disorder characterized by low levels of immunoglobulins versus normal or nearly normal numbers of circulating immunoglobulin-bearing mature B cells. Recurrent respiratory and gastrointestinal infections, mostly with encapsulated bacteria, are typical manifestations of CVID (4,6,7). CMV infection was identified as having 8.6% hematological and 5.5% ophthalmological complications in immunocompetent patients (25). However, there is no evidence of an increased incidence of CMV infection in CVID patients (26).
In our patient, bone marrow aspiration showed hypocellularity, with evidence of hemophagocytosis, so MAS could be responsible for the pancytopenia (27,28). It is well known that viral infections can trigger MAS (29). After the development of retinitis, CMV DNA was detected in the blood of our patient, showing that this virus could be responsible for the MAS. The improvement of pancytopenia seen after treatment of the CMV retinitis with ganciclovir is also evidence for CMV-induced MAS.
After the initial events of pancytopenia and MAS, CMV retinitis developed after 6 mo. Ocular CMV disease in immunocompromised individuals usually affects the retina, just as in our patient who developed CMV retinitis. Unilaterality of involvement was a unique manifestation of our patient, as most of the time CMV involvement is bilateral (30). CMV retinitis starts as a large cotton-wool spot, and in the active phase is always accompanied by a low-grade vitritis and a faint granular border of intraretinal infiltrates representing the new foci of viral activity in the normal retina (31). CMV infection causes vision loss in several ways. Most commonly the infected retina is destroyed, and patients develop an absolute scotoma due to retinal necrosis. The optic disc can also become involved, and the vision can be lost even when the amount of retinitis is still minimal. In some patients, paramacular CMV infection produces macular edema, which is a reversible cause of visual loss if treated before the active virus progresses through the fovea. Lastly, CMV retinitis can cause a retinal detachment, most commonly of the rhegmatogenous type, because there is vitreous traction on the thin atrophic retina. The posterior vitreous usually adheres to the retina, and the combination of low-grade vitritis with a thinned retina causes the vitreous to pull the retina forward, leading to its detachment (32,33). In our patient, CMV retinitis caused retinal detachment and visual impairment.
The diagnosis of CMV retinitis in our patient was established late and resulted in retinal detachment. Although the diagnosis of CMV retinitis can be established by a high level of CMV IgM antibody (>300 U/mL), accompanied by IgG-specific antibody detection, this method cannot be applied to CVID patients treated with regular immunoglobulin infusions. Therefore, molecular diagnostic methods such as PCR appear to be more specific and faster than serological or viral isolation tests (34,35). Another problem in the diagnosis of CMV retinitis in these patients is the late occurrence of visual loss once vision is normal, unless the optic disc or fovea is involved (33). As the lesions begin in the periphery, patients may not complain of symptoms. Moreover, the patients, especially children as in our case, as well as most other CVID patients, often do not notice an increase in floaters or new scotomas.
Treatment of CMV retinitis is individualized and depends on the location of the active retinitis and the immune status of the patient. Currently available anti-CMV agents include ganciclovir and its prodrug valganciclovir, foscarnet, cidofovir, fomivirsen, ganciclovir implants, and oral valganciclovir (36,37). In this case the use of ganciclovir, as well as surgical therapy, had a desirable outcome. However, in immunocompromised patients with severe CMV disease, the potential benefits of antiviral therapy are not entirely clear and should be evaluated with randomized controlled trials.
Conclusion
In every CVID patient presenting with MAS and associated cellular immune defect, the underlying cause should be identified. Steroids are useful for the treatment of MAS, and in CVID patients with impaired immune system, the CMV infection may endanger the life of the patient.
Footnotes
Author Disclosure Statement
No competing financial interests exist.