
Abstract
The development of new diagnostic methods based on molecular biology has led to evidence of the important role of respiratory viruses in chronic obstructive pulmonary disease (COPD) exacerbations. Cytokines and chemokines are recognized as key actors in the pathogenesis of COPD. The objective of this study was to evaluate the association between viral infection and host cytokine responses in 57 COPD patients hospitalized with an acute exacerbation. Seventeen cytokines were profiled using a Luminex-Biorad multiplex assay in plasma samples collected in the first 24 h following hospital admission. Stepwise linear regression analysis was performed, taking into account the influence of seven potential confounding factors in the results. Twenty-four out of 57 showed radiological signs of community-acquired pneumonia (CAP) at hospital admission, 25 patients required admission to the intensive care unit (ICU), 20 had a bacterial infection, and 20 showed a detectable respiratory virus in pharyngeal swabs. Regression analysis showed that viral infection correlated with higher levels of interleukin-6 (IL-6) (log value of the coefficient of regression B, p=0.47, 0.044), and monocyte chemoattractant protein-1 (MCP-1) (p=0.43, 0.019), and increased admission to the ICU. Viral infection also correlated with higher levels of interferon-γ (IFN-γ) (p=0.70, 0.026), which, in turn, was inversely associated with the severity of illness. Finally, viral infection was independently associated with higher levels of tumor necrosis factor-α (TNF-α) (p=0.40, 0.002). Thus our study demonstrates that in patients with COPD exacerbations, viral infection is directly associated with higher systemic levels of cytokines central to the development of the antiviral response, which are also known to contribute to inflammation-mediated tissue damage. These results reveal a potential specific role of viral infection in the pathogenesis of COPD exacerbations.
Introduction
Materials and Methods
Patients
Fifty-seven patients with a pre-existing diagnosis of COPD and clinical signs of severe disease exacerbation requiring hospitalization were recruited from September 2010 to March 2011 in the Respiratory Medicine and Intensive Care Medicine Services participating in the study. Acute exacerbation of COPD was defined as a patient showing two symptoms (at least one major) for 2 consecutive days (14). Major symptoms were defined as increased dyspnea, sputum volume, or sputum purulence, and minor symptoms were increased cough, wheezing, sore throat, or coryzal symptoms. The definition of community-acquired pneumonia (CAP) was based on current American Thoracic Society and Infectious Disease Society of America guidelines (10). Five milliliters of whole blood were collected from each patient in the first 24 h following hospital admission in an ethylenediaminetetraacetic acid-containing venous blood vacuum collection tube. A pharyngeal swab (PS) and sputum sample were collected in parallel. All patients were treated with bronchodilators, antibiotics, and systemic steroids (IV methylprednisolone, 20–40 mg/day). Informed consent was obtained directly from each patient before enrollment. Thirteen healthy volunteers of similar age showing no clinical signs of infectious or inflammatory disease were recruited from the workers at the University of Valladolid, Spain. Both patients and controls remained anonymous. The protocol was approved by the ethics committee on clinical research of each of the participating centers.
Microbial diagnosis
Sputum samples were routinely gram-stained and cultured on general purpose media (blood, agar, chocolate agar, and McConkey agar). Fungal infections were screened by culturing sputum samples on Sabouraud agar containing chloramphenicol (19). Viral diagnosis was performed on RNA from pharyngeal swabs by reverse transcription-polymerase chain reaction (PCR)-based methods using reagents purchased from Roche (Swine Inf A/H1N1 detection set). The samples were also assessed by multiplex PCR (Luminex) with the xTAG RVP kit from Luminex-Abbott for infection with respiratory syncytial virus (RSV), influenza B virus, parainfluenza viruses 1–4, human metapneumovirus, enteroviruses, rhinovirus, adenovirus, bocavirus, and coronaviruses NL63, HKU1, 229E and OC43, in accordance with the manufacturer's instructions.
Cytokine profiling
Plasma samples were obtained after proper centrifugation of whole blood, and these were stored at −80°C until cytokine profiling. Plasma chemokine and cytokine levels were evaluated using the Bio-Plex Human Cytokine 17-Plex Panel (Bio-Rad, Hercules, CA), following the manufacturer's instructions.
Statistical analysis
The variable “presence/absence of viral infection,” along with a number of representative clinical variables, were entered into a stepwise linear regression analysis to evaluate their association with the levels of each of the cytokines profiled. Variables tested were: [Age], [Sex], [Presence of CAP (Yes/No)], [Necessity of Invasive mechanical ventilation (Yes/No)], [Admission to ICU (Yes/No)], [Viral infection (Yes/No)], [Bacterial infection (Yes/No)], and [Co-infection (virus+bacteria) (Yes/No)]. Comparisons of immune parameter levels were performed using the Mann-Whitney U test. All statistical tests were two-sided, and p<0.05 was considered significant. Data analysis was performed using SPSS for Windows 15.0 (SPSS, Chicago, IL).
Results
Clinical and microbiological data
Most patients were elderly males (male: n=47, age [mean, SD] [72.7 y, 9.5 y]; female: n=10, [63.5 y, 12.3 y]). Twenty-four out of 57 showed radiological signs of CAP at hospital admission, 25 required admission to the ICU, and 10 critically ill patients needed invasive mechanical ventilation. Seven critically ill patients died. The cause of death was refractory hypoxemia (n=4), multiorgan dysfunction (n=1), and peritonitis (n=2). Twenty patients had a bacterial infection at sample collection, and 20 showed detectable respiratory virus in pharyngeal swabs. In the non-critically patients, infection by Pseudomonas aeruginosa was found in 2 cases, Staphylococcus aureus in 3 cases, and Haemophilus influenzae in 2 cases. In the critically ill patients, 1 case of infection with S. aureus, 1 case of Chlamydia pneumoniae, 5 cases of Streptococcus pneumoniae, 1 case of P. aeruginosa, 1 case of Aspergillus fumigatus, 1 case of H. influenzae, 1 case of Streptococcus epidermidis, 1 case of Streptococcus hominis, and 1 co-infection with Escherichia coli plus S. aureus were detected. In the non-critically ill patients, parainfluenza 3 virus was found in 1 case, coronavirus 229E in 2 cases, rhinovirus in 3 cases, influenza A H1N1 ns (new subtype) in 1 case, and metapneumovirus in 1 case. In the critically ill patients, 1 case of rhinovirus, 3 cases of RSV, 1 case of metapneumovirus, 6 cases of influenza A/H1N1 ns, and 1 case of influenza B were found. Two of the non-critically ill patients had co-infection by rhinovirus plus P. aeruginosa. For patients admitted to the ICU, 2 cases of co-infection with influenza A/H1N1nv plus S. pneumoniae, 1 case of co-infection with RSV plus S. pneumoniae, 1 case of co-infection with influenza A/H1N1nv plus P. aeruginosa, 1 case of co-infection with influenza A/H1N1nv plus A. fumigatus, and 1 case of co-infection with metapneumovirus plus S. epidermidis were found. Three of the critical patients with influenza infection had received the seasonal influenza vaccine.
Cytokine profiling
IL-1RA, IL-2, IL-4, IL-5, and IL-10 were not present at detectable levels in the vast majority of patients, so these mediators were not included in the statistical analysis. Multivariate regression analysis showed that the variable [admission to ICU] was associated with higher levels of IL-6, MCP-1, IL-8, and MIP-1β, and with lower levels of IFN-γ. The variable [viral infection] was independently associated with the existence of higher levels of TNF-α (Table 1). In turn, the variable [viral infection] was also associated with higher levels of IL-6 and MCP-1, adjusted by the variable [admission to ICU]. Stepwise analysis identified a positive association between IFN-γ and [viral infection], coexisting with an inverse correlation between this cytokine and the variable [admission to ICU]. Both the variables [viral infection] and [bacterial infection] were associated with higher levels of G-CSF. On the contrary, no significant correlations were found for the variable [presence of bacterial+viral co-infection]. Compared to healthy controls, patients with COPD exacerbations showed significantly higher levels of a wide range of cytokines. Patients admitted to the ICU showed higher levels of IL-6, IL-8, MCP-1, and MIP-1β than non-critical patients (Fig. 1). Patients with viral or bacterial infections showed higher levels of IL-6, G-CSF, and MCP-1, than COPD patients with an absence of detectable virus or bacteria. In addition, patients with viral infections showed higher levels of TNF-α than those without (Table 2). Patients with a co-infection by (virus+bacteria) also exhibited higher levels of IL-6 and MCP-1 than those with negative microbiology results (Table 2). Patients with CAP showed higher levels of IL-6 than those without radiological evidence of disease on chest x-ray (data not shown).
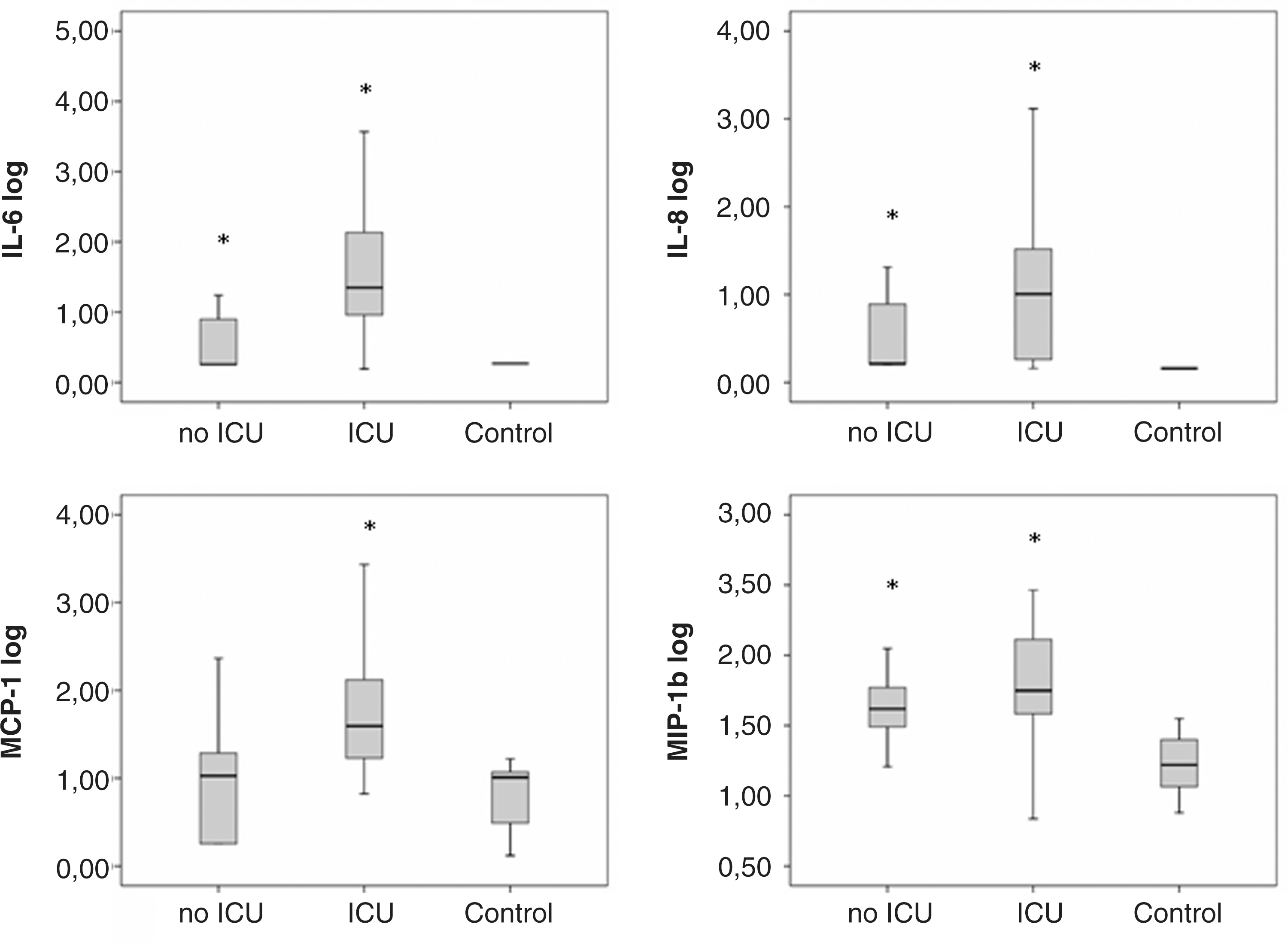
Cytokine levels in critically and non-critically ill COPD patients. All the cytokines are represented as log values, and showed significant differences between critical and non-critical patients. The healthy control group is represented for comparison purposes (*p<0.05 significant difference from the control group).
Logarithmic values were used for cytokine levels.
B, coefficient of regression; SE, standard error of B.
Significant differences with the group [negative for microbes].
Significant differences with the group [healthy controls].
Results are showed as median [interquartile rank] (pg/mL).
Discussion
In the past, the role of viral infection in COPD has been underestimated, since the absence of appropriate diagnostic methods precluded the identification of respiratory viruses in the respiratory samples obtained from these patients. The host immune response plays a major role in this disease, and is characterized by exacerbated inflammation of the bronchial tree. There is little information on how viral infections influence host immune responses in patients with COPD exacerbations. By performing stepwise linear regression analyses, we evaluated the association between viral infection and the levels of 17 cytokines in plasma from 57 patients hospitalized for severe COPD exacerbations, taking into account the relative influence of six major clinical variables on the results.
Viral infection was associated with higher levels of IL-6 and MCP-1 in plasma, which was associated with increased severity of illness. IL-6 is a pleiotropic cytokine involved in various aspects of the host immune response to infection, most notably the acute inflammatory response (5). Seemungal and associates found evidence of a tendency toward higher plasma and serum IL-6 levels in those with COPD exacerbations of viral origin (16). Hutchinson and colleagues found that the addition of IL-6 levels increases the specificity of a clinical case definition for viral infection in COPD patients (6). High levels of IL-6 have also been described in patients with critical respiratory conditions due to severe influenza infections (2,8). MCP-1 is a potent chemoattractant for eosinophils, memory T cells, and monocytes, thus contributing to the accumulation of proinflammatory cells at the site of infection (15). High levels of MCP-1 in plasma have been described in patients with pandemic H1N1 pneumonia (8), and infection by the severe acute respiratory syndrome-associated coronavirus (3).
Critical illness is characterized by the development of the systemic inflammatory response syndrome (SIRS) (13). In agreement with this, critical illness was associated with higher levels of the innate immunity-related mediators IL-6, MCP-1, IL-8, and MIP-1β. Mechanical ventilation can itself induce a proinflammatory state in patients (12). Nonetheless, this variable did not independently influence the cytokine profiles associated with viral infection in our cohort of patients.
Viral infection was also associated with higher levels of IFN-γ, a T-helper-1 cytokine, in those with non-critical illness. IFN-γ promotes proliferation of antigen-stimulated T cells and the generation of CD8 cytotoxic T cells (18). This molecule is thought to help maintain homeostasis between the development of the autoinflammatory innate and adaptive immune responses, and could play a beneficial role in this disease (3).
Viral infection was independently associated with higher levels of TNF-α. This molecule is primarily a mononuclear phagocyte–derived cytokine that has pleiotropic effects on innate host responses to micro-organisms. While TNF-α does not directly mediate the migration of neutrophils, it regulates neutrophil–endothelial cell adhesion molecules and CXC chemokines, which recruit inflammatory cells to the site of infection (18). Although we failed to find significant differences in TNF-α levels between patients with viral or bacterial infections, regression analysis supports the notion that viral infection is strongly involved in the generation of the marked TNF-α response seen in COPD exacerbations. Other chemokines such as IP-10, which were not profiled here, have shown value as biomarkers of rhinovirus infection in those with exacerbations of COPD (14).
G-CSF was a marker of both viral and bacterial infection. G-CSF is the principal cytokine controlling neutrophil development and function, and could thus mediate recruitment of these cells to the lungs. We have recently reported the negative association of G-CSF with severe pandemic influenza outcomes (1). Co-infection by (virus+bacteria) was more frequent in the most severe patients, and those admitted to the ICU, but on the contrary it was not independently associated with higher or lower levels of cytokines in plasma, perhaps due to the low number of co-infected patients.
Finally, patients with the presence of detectable virus or bacteria showed higher levels of innate immune mediators (IL-6, G-CSF, and MCP-1) than those with negative microbiological results, probably as a consequence of more intense stimuli of the immune system due to the presence of high microbial loads.
Taken together, our results suggest that viral infection in COPD exacerbations is a principal contributor to the secretion of a group of chemotactic and T-helper mediators typically involved in the defense against intracellular microbes, but that are also able to induce inflammation-mediated tissue damage.
Why is viral infection such an important inducer of the secretion of inflammatory mediators in COPD? Cigarette smoking is a major pathogenic factor in this disease. In fact, 88% of our patients showed a had a history of smoking. Studies on murine models have demonstrated that cigarette smoke selectively augments the airway and alveolar inflammatory responses induced in the lung by viral pathogen-associated molecular patterns and viruses (7).
A drawback of our study was the limited diversity of viral and bacterial infections present in our cohort. Another drawback is the absence of cytokine profiles in respiratory samples, which may better mirror the pathogenic events taking place in the lungs of these patients. The potential consequences of viral infection for the clinical outcomes of patients with COPD need to be studied in the future, as do the potential effects of preventive interventions such as vaccination.
Conclusion
Our study demonstrates that viral infection is directly associated with increased proinflammatory and chemotactic responses at the systemic level in COPD exacerbations, revealing a potential role of viral infection in the pathogenesis of this disease.
Footnotes
Acknowledgments
The authors acknowledge the support of the Ministry of Science, Spain (MICCIN-Fondo de Investigaciones Sanitarias), and the Health Council, Junta de Castilla y León (JCYL-IECSCYL-SACYL): Programa Grupos Emergentes, EMER07/050, proyectos de investigación sanitaria, PI081236, and Programa de Investigación Comisionada en Gripe, GR09/0021. The authors thank Verónica Iglesias for her assistance in cytokine profiling.
Author Disclosure Statement
No competing financial interests exist.