
Abstract
Influenza vaccination, which has been targeted to the elderly and those at serious risk of complications, is recommended. The purpose of this study was to determine antibody responses after influenza vaccination among Thai elderly persons living in the community. A total of 591 subjects consisting of 308 vaccinees and 283 non-vaccinees were enrolled in the study. Antibodies to H1N1, H3N2, and B viruses were detected by hemagglutination inhibition (HI) testing. The numbers of subjects who had protective antibody titers ≥40 and geometric mean titers (GMTs) of antibodies against A(H1N1), A(H3N2), and B viruses prior to vaccination were similar for the vaccine and placebo groups. The seroprotection rates and GMTs for influenza virus A(H1N1), A(H3N2), and B strains after influenza vaccination at 1, 5, and 12 mo in the vaccine group were significantly higher than those in the placebo group. The seroprotection rates for the A(H1N1) and A(H3N2) strains, but not the B strain, met Committee for Proprietary Medicinal Products (CPMP) criteria (>60%). GMTs and seroprotection rates against influenza B strain in the vaccinees at all time points were <40% and <60%, respectively, and significant differences between the vaccinees and the placebo controls were observed. The GMTs and seroprotection rates for influenza strains in those with pre-existing antibody titers ≥40 were significantly higher than those in the group with pre-existing antibody titers <40. These findings demonstrated that the elderly living in the community developed adequate antibody responses with sustainable titers throughout the 12-month study period after influenza vaccine immunization. Moreover, the presence of pre-existing antibody at a titer ≥40 prior to vaccination strongly affected the antibody response to influenza vaccination.
Introduction
Human influenza worldwide is caused by influenza virus types A/H1N1, A/H3N2, and B, but the disease caused by avian influenza virus subtypes H5, H7, and H9, were occasionally reported (5,9,21). Influenza virus contains a genome of eight RNA segments, two of which encode two envelope proteins, hemagglutinin (H) and neuraminidase (N). The serological assays for detecting antibodies to H protein are generally employed for diagnosis and measuring immunogenicity after influenza vaccination (8). We previously reported an efficacy of 56%, with a significant decrease in incidence of the disease after influenza vaccination in Thai elderly living in the community (23). However, the long-term antibody response after influenza vaccination has not yet been reported. The purpose of this study was to demonstrate the kinetics of the antibody response and seroprotection rates, both before and after influenza vaccination, during a 1-year study period. The criteria for vaccine assessment of the Committee for Proprietary Medicinal Products (CPMP) using an HI assay in paired sera have been established to evaluate influenza vaccine immunogenicity (7). To meet the criteria applied for adults aged >60 y, at least one of the following assessments should be achieved: (1) the seroconversion rate in the vaccinee group should be at least 30% higher than that in the placebo group, (2) a greater than twofold increase in mean geometric mean titer (GMT), or (3) a >60% seroprotection rate against at least one vaccine strain. Here we applied the CPMP guidelines to study the kinetics of the antibody response and seroprotection rates after influenza vaccination in the elderly living in the community for a 1-year follow-up period.
Materials and Methods
Subjects
A total of 591 elderly persons living in the communities within 10 km around Bangkok, Thailand, were enrolled in a double-blind case-control study from 1998 to 1999. In all, 308 subjects received vaccines, whereas 283 subjects received a tetanus toxoid injection as placebo. The mean ages±SD of the 308 subjects in the vaccine group and 283 in the placebo group were 68.2±6.4 y and 68.1±6.9 y, respectively. The study was approved by the Ethics Committee on Human Rights involving Human Research, Faculty of Medicine Siriraj Hospital, Mahidol University.
Vaccines
The vaccine used was the purified trivalent split-virus vaccine (VaxigripR) manufactured by Pasteur Merieux (Lyon, France). Each dose (0.5 mL) contained influenza A/Johannesburg/82/96 (H1N1), A/Nanchang/ 993/95 (H3N2), and B/Harbin/7/94, all with 15 μg of hemagglutinin. These vaccine antigens were in accordance with the recommendations of the WHO. A 0.5-mL dose of tetanus toxoid was used as placebo.
Specimen collection
A 10-mL venous blood sample was collected from each subject during the first visit prior to vaccination or placebo injection to detect baseline antibodies to influenza viruses. Then sequential blood samples were collected at 1 mo, 5 mo, and 12 mo to determine antibody responses after vaccination.
Hemagglutination inhibition (HI) test
Details of the HI test procedure are described elsewhere (3,6,16,23,28). Briefly, serum non-specific inhibitor was treated with receptor-destroying enzyme from Vibrio cholerae (Denka Seiken, Tokyo, Japan) overnight at 4°C, followed by inactivation at 56°C for 30 min. Non-specific agglutinator was removed by absorption with 50% chick red blood cells. The test antigen panel comprised of influenza A(H1N1), A(H3N2), and influenza B viruses were provided by the WHO.
Data and statistical analysis
Data were analyzed using SPSS version 11.5 software. A serum sample with HI antibody titer ≥10 was considered to be positive for influenza antibody. An HI antibody titer <10 was assigned the value of 5. The level of protective titer was defined as HI titer ≥40. The seroprotection rate was given as the percentage of subjects with a protective HI antibody titer ≥40. The CPMP criteria for the annual influenza vaccine (7) was used for the assessment of acceptable immune responses. The criterion of the seroprotection rate for each strain approximately 3 wk after vaccination for adults aged over 60 y is >60%. The vaccine responder rate was calculated as the proportion of subjects with at least a fourfold rise in HI titers and protective HI antibody titer ≥40. GMT was determined using SPSS version 11.5 with the option Mode Compare means/Mean/Option/Statistics: Geometric mean. Comparison of GMT values and mean fold increase (FI) in titers between the two groups were performed using the Mann-Whitney U test. Comparison of prevalence between the two groups was performed by the chi-square test. Fisher's exact test was performed for the analysis of contingency tables when sample sizes were small. The level of significance was assigned as p<0.05.
Results
Baseline HI antibody levels prior to influenza vaccination
The distribution of HI antibodies to A(H1N1), A(H3N2), and B virus strains in serum samples collected before vaccination is shown in Table 1. GMTs of antibodies against the A(H1N1), A(H3N2), and B strains prior to vaccination in the vaccine and the placebo groups were not significantly different (23.36 versus 23.92; 21.37 versus 18.90; and 6.28 versus 6.10, respectively; p>0.05 for all pairs analyzed). Also, seroprotection rates by percentages of subjects who had protective antibody titers of ≥40 to the A(H1N1), A(H3N2), and B strains in the vaccine group were not significantly different from those in the placebo group (43.8% versus 48.1%, 39.0% versus 34.6%, and 4.2% versus 3.5%, respectively; p>0.05 for all pairs analyzed).
GMT, geometric mean titer; HI, hemagglutination inhibition.
Antibody response after influenza vaccination
During 1 y of the longitudinal study, the HI assay was performed in blood samples collected at pre-vaccination, and 1, 5, and 12 mo post-vaccination, for evaluation of the sustainable antibody response. At 1 mo after influenza vaccination (Fig. 1), the GMTs of antibodies against A(H1N1) and A(H3N2) in serum samples collected from the vaccinees at all time points were significantly higher than those in placebo controls (354.90 versus 25.18, 238.29 versus 20.10, and 24.71 versus 6.17, respectively; p<0.001 for all pairs analyzed). Similarly, the seroprotection rates for the A(H1N1), A(H3N2), and B strains were statistically significantly higher in the vaccine group than in the placebo group (98.4% versus 49.1%, p<0.001; 96.1% versus 36.4%, p<0.001; and 47.4% versus 3.5%, p<0.001, respectively; Fig. 2). Nevertheless, only the A(H1N1) and A(H3N2), but not the B strain, induced seroprotection rates of greater than 60%.
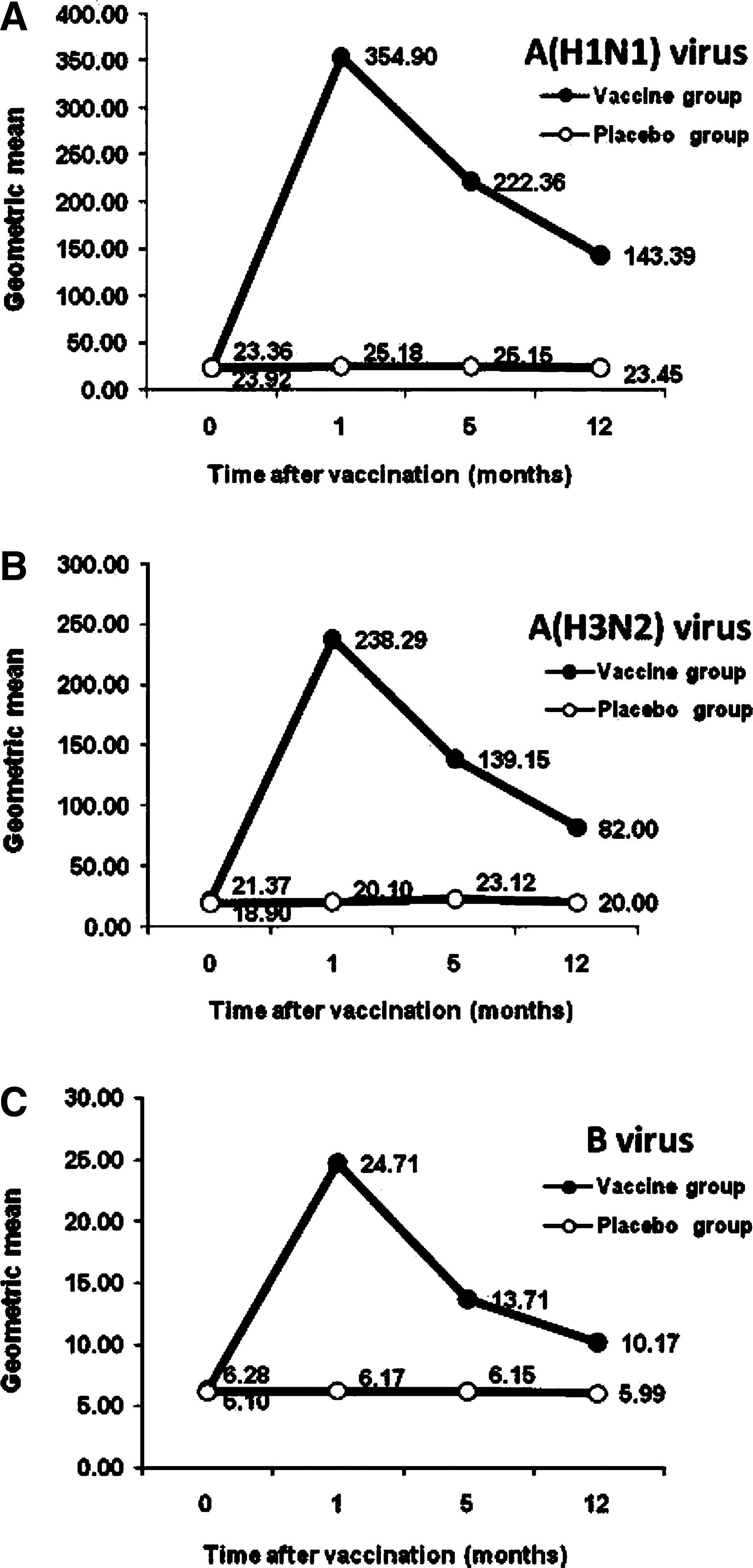
Kinetics of antibody response by GMTs during 1 y of influenza vaccination for the vaccine group (●) and the placebo group (○) for A(H1N1) (
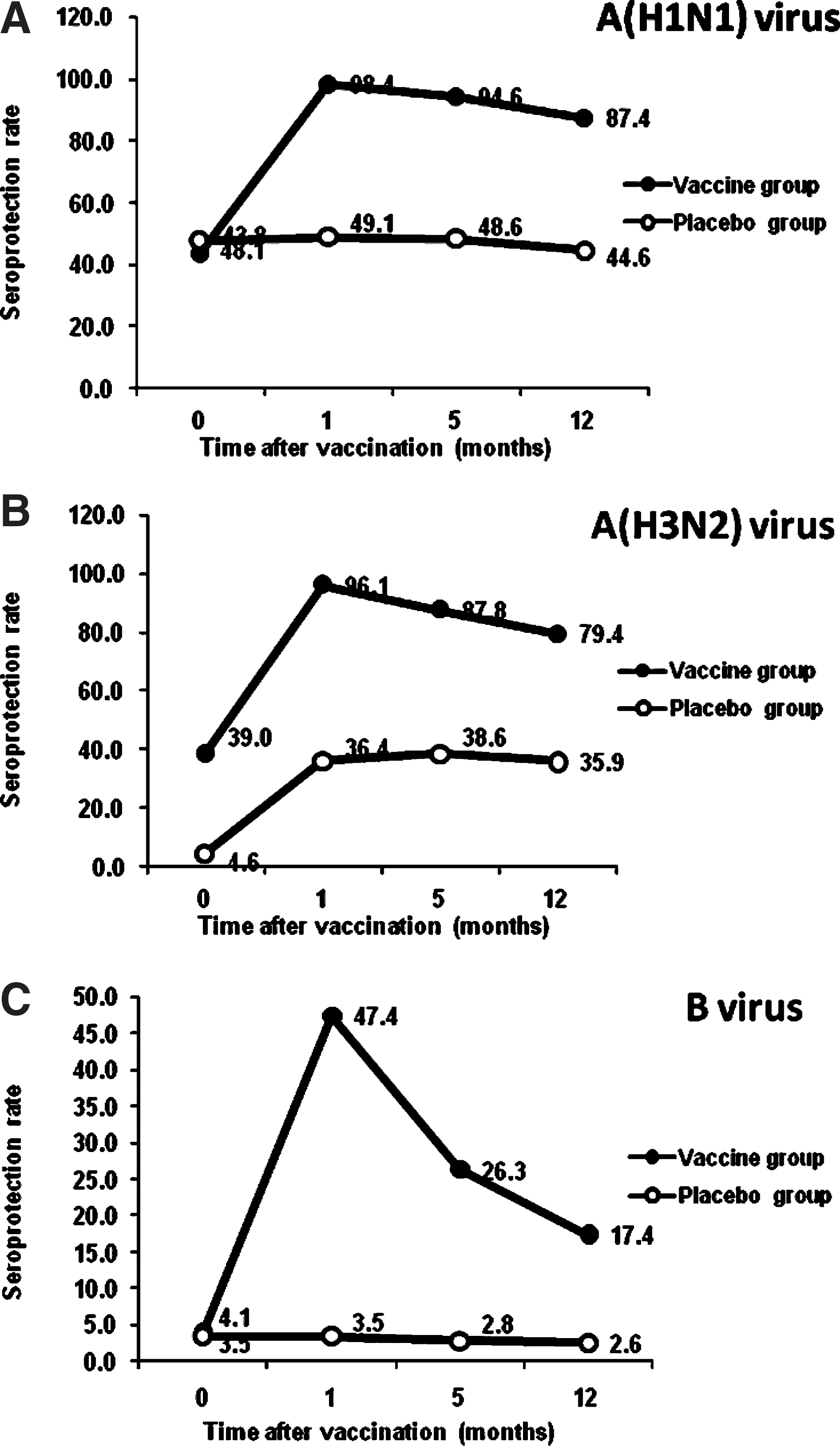
Seroprotection rates during 1 y of influenza vaccination for the vaccine group (●) and the placebo group (○) for A(H1N1) (
GMTs after influenza vaccination at 5 and 12 mo in the vaccine group were 222.36 and 143.39 for the influenza A(H1N1) virus, 139.15 and 82.00 for the A(H3N2) virus, and 13.71 and 10.17 for the influenza B virus. Moreover, the seroprotection rates against the A(H1N1) and A(H3N2) strains in the vaccine group were greater than 60%, and were significantly higher than those of the placebo group. The seroprotection rates for A(H1N1) at 5 and 12 mo were 94.6% and 87.4%, whereas those for A(H3N2) at 5 and 12 mo were 87.8% and 79.4% (Fig. 2). The GMTs and seroprotection rates against the influenza B strain in the vaccinees at all time points were less than 40 and lower than 60%, respectively, and significant differences were seen between the vaccinees and the placebo controls (Figs. 1 and 2).
The effect of pre-existing antibody at the protective titer level of ≥40 on antibody response after influenza vaccination
The effect of pre-existing antibody on the response to influenza vaccination was further explored. As the HI antibody titer of ≥40 was defined as the protective titer, the subjects were divided into two subgroups: the first subgroup had pre-existing antibody titers <40, and the second included subjects who had pre-existing antibody titers ≥40.
At 1 mo after influenza vaccination, the antibody response was apparent in terms of seroprotection rates, GMTs, and mean FI in antibody level, for the titers before and after vaccination, as shown in Table 2. After vaccination, the GMTs against all vaccine strains for the A(H1N1), A(H3N2), and B strains in the group with pre-existing antibody titers ≥40 increased to a significantly higher level (p<0.001) than those in the group with pre-existing antibody titers <40. Similarly, the seroprotection rates for all influenza strains were also significantly higher in the group with pre-existing antibody titers ≥40. In contrast, the mean FIs in antibody levels were significantly higher in the group with pre-existing antibody titers <40. However, these results were true for the analyses of the A(H1N1) and A(H3N2) strains, but not for the influenza B strain.
Statistical significance level set at p<0.05.
At 1 mo after vaccination, the percentages of vaccine responders were determined in the subjects with pre-existing antibody titers <40 or ≥40 (Table 3). The results showed that the subjects with pre-existing titers <40 developed a ≥fourfold increase in HI antibody titer against the A(H1N1), A(H3N2), and B strains, of 93.5%, 93.1%, and 56.3%, respectively, whereas 89.2%, 61.7%, and 38.5%, respectively, of the subjects with pre-existing antibody titers ≥40 did. Clearly the subjects with pre-existing titers <40 who responded to the vaccine responded better than those in the group with pre-existing antibody titers ≥40.
Discussion
The main protective benefit of influenza vaccination is related to the antibody response to the hemagglutinin (H) component of the trivalent vaccine strains (14). The HI assay generally employed for vaccine evaluation is dependent on the antibodies that inhibit the interaction between the receptor binding domain within the HA1 domain of influenza virus hemagglutinin and the sialic acid receptor on red blood cells (14). Following the CPMP criteria for vaccine evaluation and immunogenicity testing, HI antibody titers ≥40 have been accepted as the level for protection against influenza virus infection (3,6,16,23,28). In the present study, the kinetics of the antibody response after influenza vaccination in the elderly living in the community were investigated by HI assay. At 1 mo after vaccination, the GMTs of antibodies against the A(H1N1), A(H3N2), and B strains were significantly higher in the vaccinees than in the controls. These results are inconsistent with the findings of other studies of elderly individuals (3,6,11,13,16,23,28,30). The GMTs of antibodies to all influenza vaccine strains in our study persisted above the protective level throughout the 12-month follow-up period. The antibody response of the type B strain was lower than those of the type A strains. The explanation for this result might be due to the properties of the type B vaccine antigen and/or the type B test antigen used in the HI test. The result of the low antibody response against the type B strain is consistent with the previous reports (2,25).
The present study showed that some of the elderly subjects had pre-existing antibodies to the vaccine strains prior to vaccination, which may be due to previous natural influenza virus infections, or previous influenza vaccinations. Interestingly, the data analysis at 1 mo after vaccination demonstrated that the GMTs and the seroprotection rates for the A(H1N1), A(H3N2), and B strains in the subjects with pre-existing HI titers ≥40 were significantly higher than those with pre-existing HI titers <40. Inversely, the values of the mean fold increase in antibody level and the number of vaccine responders were greater in the group with pre-existing HI titers <40. These results suggest that the pre-existing antibody might exert some influence on the antibody response against influenza vaccination. Similarly, other studies have reported that vaccinees with a history of influenza vaccination were better protected than those who were vaccinated for the first time (5). Furthermore, an increase in vaccine effectiveness was demonstrated with repeated annual influenza vaccination (1,15,27). These results suggest that influenza vaccination can boost the anamnestic response through memory B cells for antibody production (22). Though the impairment of immune function in the elderly was noted, their immune responses were quite functional, with the ability to induce an antibody response after influenza vaccination.
Several groups of investigators including our previous report on this group of subjects have demonstrated the efficacy of influenza vaccination in the elderly. Our previous report (23) demonstrated that the relative risk reduction in serological influenza confirmed the 56% efficacy of vaccination with an incidence of influenza-like illness of 4.83% in the vaccine group, compared to 10.88% in the placebo group. Chuaychoo et al. (6) conducted a similar study in which vaccine efficacy in the elderly was about 50%, but antibody responses to the vaccine were not significantly correlated with protection against laboratory-confirmed influenza illness. In fact, it is now generally accepted that the measurement of HI titers following vaccination does not give a complete picture of the responses in elderly populations (19). In addition, protection against influenza improves when vaccinations are received annually in subjects with a limited antibody response, suggesting that cellular immune mechanisms may also be important for protection in older adults (1,15,27). An additional advantage of vaccination in the elderly is the induction of influenza cross-subtype immunity. Our group previously reported that the seasonal influenza vaccine could induce cross-neutralizing antibody against H5N1 virus in the elderly (17), but not in 42 young vaccinees aged 25–40 y (unpublished data), or in 140 healthy subjects aged 20–45 y (26).
In the present study, the seroprotection rates for both the A(H1N1) and A(H3N2) vaccine strains, but not influenza B strain, met the CPMP criteria (a greater than 60% seroprotection rate in the elderly aged >60 y), and the antibody levels were sustainable as investigated in blood samples collected at different time points during the 1-year follow-up period. Even though the results for the influenza B strain were not substantial, the GMTs and seroprotection rates induced in the vaccine group were significantly higher than those in the placebo group. Overall, influenza immunization in the elderly living in the community was effective, and annual vaccinations should be recommended.
Footnotes
Acknowledgments
This work was supported by grants from the National Research Council of Thailand and the Chalermphrakiat Grant, Faculty of Medicine Siriraj Hospital, Mahidol University. The authors thank the WHO for kindly providing the influenza antigens. The authors also wish to thank all of the elderly persons in Taling Chan, Bangkok Noi, Bangkok Yai, Bang Phlat, Phasi Charoen, and Khlongsan, who participated in the study. The authors wish to thank Dr. Wichai Chattanavaree and Ms. Anjana Klangkaew for their assistance in performing the study, Mr. Suthipol Udompanturak for the statistical analysis, and Ms. Arocha Sapsakultong for preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.