
Abstract
There are few studies on health-facility based prevalence rates for dual hepatitis B virus-hepatitis C virus (HBV-HCV) infection on a state-wide scale in Nigeria. In this study we determined the state-wide prevalence rate of dual positivity of hepatitis B surface antigen and anti-HCV antibody among hospital patients of Ekiti State, Nigeria, and identified associated factors. Consenting apparently-healthy patients visiting health centers in all local government area (LGA) headquarters of Ekiti State were consecutively selected to a total of 2000 individuals. Patient demographic data pertinent to HBV and HCV transmission were obtained using a structured questionnaire. Subsequently, serum samples prepared from the aseptically collected blood was tested for the presence of both HBsAg and anti-HCV antibody using DiaSpot test strips. The results were analyzed using binary logistic regression. Dual positivity of 7.40% was recorded among the study participants, with 9.80% and 12.80%, respectively, testing positive for HBsAg and anti-HCV antibody. The study patients were, however, most likely to be anti-HCV antibody positive. Nine of the 10 factors studied were independently associated with dual positivity. Five of these, in descending order of odds ratio, were: illiteracy (15.76, p=0.001); having ≥4 sexual partners (9.46, p=0.001); age range of 35–44 y (8.46,p=0.001); farming (7.33, p=0.001); and “not at all” to use of condoms during sexual intercourse (4.39, p=0.001). The dual positivity rate was relatively high, with unprotected sexual intercourse as the most probable mode of acquisition of HBV and HCV by the seropositive study participants.
Introduction
Invasion of the human body by either of these viruses is first recognized by innate immunity, and later by the cellular and humoral immune response (7 –11). The cellular immunity is comprised of CD4+ T-helper 1 and cytotoxic CD8+ T cells that target and bind endogenously processed viral proteins expressed on the surface of infected hepatocytes, which are eventually lysed (12,13). This mediates clearance of HBV and HCV from the body of immunocompetent infected humans, and causes immune-mediated liver damage (14). The specific humoral immune response is comprised of antibodies directed at specific antigens of HBV and HCV. The presence of HBsAg or anti-HCV antibodies is detectable by specific laboratory tests, and they thus serve as reliable markers of natural infection, which are useful in seroepidemiology (15 –18).
In the absence of specific medical interventions, a common occurrence of chronic hepatitis B (CHB) or chronic hepatitis C (CHC) infection is progression to liver fibrosis, cirrhosis, and finally to hepatocellular carcinoma (HCC) (19) and death. This characteristic, among others, makes dual infection a global health problem, since it is associated with more rapid hepatic fibrotic progression and more severe liver disease, with a higher risk of progression to cirrhosis and HCC (1,7,20).
The occurrence of dual infection has been reported in various parts of the world. Generally, the prevalence of dual infection was around 10–20% in patients with CHB, and 2–10% for those having anti-HCV antibody (21 –23). In Kosovo, laboratory testing of 70,348 blood samples from voluntary blood donors revealed a dual infection prevalence rate of 0.0002% (14/70,348), with 4.2% and 0.3%, respectively, for HBV and HCV infection. In the same study, males had higher prevalence rates for both HBV and HCV infection (24). Pennap et al. (6) reported a HBV and HCV co-infection rate of 8.85% (n=113) among apparently healthy people of a local community in Keffi, Nigeria. The study documented a 13.3% prevalence rate each for HBV and HCV infection. But in University of Benin teaching hospital in Nigeria, a lower rate of dual infection (0.57%, n=5760) among pregnant women was reported (4). In India, a dual infection rate of 0.95% (n=105) was recorded among STD clinic attendees (25).
With regard to risk factors, high-risk populations for concurrent infection with HBV and HCV have been identified. These include injection drug users (IDU, 42.5%) (26), patients on hemodialysis (3.7%) (27), recipients of organ transplants (8%) (28), HIV-positive individuals (66%) (29), and beta-thalassemia patients (10%) (30). Other risk factors for dual HBV-HCV infection are advanced age and certain races and ethnicities (31).
To our knowledge, there is little literature on the state-wide prevalence of dual HBV-HCV infection and the associated human variables in Ekiti State, Nigeria. This study was therefore designed to determine the health-facility-based prevalence of dual HBV-HCV infection in apparently-healthy individuals visiting health care centers in Ekiti State, and to evaluate factors associated with dual infection, and identify the most probable routes of transmission of the viruses.
Materials and Methods
Study area
We conducted this study in the 16 local government areas (LGAs) that make up Ekiti State, Nigeria, between January and November 2009. The state is located between latitude 7°4’ N of the equator, and longitude 5°15’ E of the Greenwich meridian at approximately 300 meters above sea level. The surface area is 5887.089 km2, with an estimated population of 2,735,186 (Ekiti State Ministry of Information, 2010).
Study population
The study population comprised a mixture of people residing in all the LGAs of Ekiti State during the study period. They were made up of indigenous and non-indigenous persons of different ethnic, religious, educational, and social backgrounds. The occupations of the people of Ekiti State include civil service, farming, trading, and artisanship, among others.
Study design
This was a cross-sectional, health-facility-based study. In order to obtain a study sample representative of the state, participants were selected from each LGA's headquarters (Table 1). To further buttress this, mostly utilized health-care center in each headquarter was used as sampling location. Approval to carry out the study was granted by the officials of each health-care center. Designated hospital staff members clearly explained, in English or in the individual's dialect, the objectives and procedures of the study to each prospective participant. Apparently-healthy individuals that verbally consented to participate were consecutively recruited for the study. Pertinent demographic and behavioral data that might influence transmission and acquisition of HBV and HCV were obtained using interviewer-administered questionnaires. Demographic data included age, gender, educational status, occupation, marital status, and LGA (2,44), while behavioral data included the number of sexual partners and condom use during sexual intercourse (3) (Tables 2 and 3). The participants were assigned identification numbers and were assured that all information obtained would be treated with the utmost confidentiality and used solely for the purpose of our research. The data collected are shown in Table 2. Inclusion criteria were apparently-healthy persons visiting health facilities in the headquarters of the LGAs, and there were no exclusion criteria. The research was carried out according to ethical research standards.
HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus.
Reference group.
Odds ratios of the other LGAs were statistically comparable to that of Oye LGA.
Data for 12 participants were removed due to irregularities, making a total of 1988 subjects.
Statistical significance set at p≤0.05.
HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus.
Reference group.
Odds ratios of the other LGAs were statistically comparable to that of Oye LGA.
Data for 12 participants were removed due to irregularities, making a total of 1988 subjects.
Statistical significance set at p≤0.05.
HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus.
Blood sample collection and serum preparation
Blood samples were aseptically collected by venipuncture. A 5-mL blood sample was collected using a disposable sterile needle and syringe from each participant. The blood sample was transferred into a labeled blood sample tube containing no anticoagulant. Serum was prepared from the clotted blood and stored at −20°C until used for serology.
Serological testing
Two different serologic tests were performed on each participant's serum sample. We tested for HBsAg with DiaSpot® HBsAg, a one-step HBsAg test strip (Bresta Perkasa, Djakarta, Indonesia). The kit uses a rapid chromatographic immunoassay for the qualitative detection of HBsAg (relative sensitivity and specificity: ≥99.0% and 97.0%, respectively). The test was carried out and interpreted according to the manufacturer's instructions. Briefly, the package containing the test strip was opened to attain room temperature before opening the sealed pouch inside. Each test strip, one per sample, was immersed vertically in the serum sample for at least 10–15 sec, after which it was removed and placed on a non-absorbent flat surface for 15 min before the test was read. Antibody to HCV in the serum samples was tested for using the DiaSpot HCV, a one-step hepatitis C virus test strip (relative sensitivity and specificity: ≥99.0% and 98.6%, respectively). This test was carried out and interpreted as described above for HBsAg detection in the serum samples.
Statistical analysis
Here we present data generated with descriptive statistics. Statistical associations or a lack thereof between participant variables and prevalence rates of dual infection were determined using binary logistic regression analysis to estimate odds ratios (OR) with 95% confidence intervals (CI) (26,42). A p value ≤0.05 was set as statistical significance. The analysis was performed with SPSS 15.0 for Windows (SPSS Inc., Chicago, IL).
Results
Characteristics of study participants
A total of 2000 serum samples from participants comprising male and female individuals in the 16 LGAs that make up Ekiti State, Nigeria, were tested for HBsAg and anti-HCV antibody (Table 1). All were aged ≥15 y. The lowest (20) and highest (300) numbers of participants were from Emure and Ado LGAs, respectively. Other demographic characteristics of the participants are shown in Table 2.
Prevalence rate of dual seropositivity
Of the 2000 serum samples studied, 600 were found to be positive, giving an overall seropositivity rate of 30.00% (95% CI 28.00%,32.00%). Of all the positive samples, 148 (7.40%; 95% CI 6.25%,8.55%) had dual seropositivity, 196 (9.80%; 95% CI 8.50%,11.10%) were positive for HBsAg, and 256 (12.80%; 95% CI 11.34%,14.26%) were positive for anti-HCV antibody (Fig. 1). The lowest and highest prevalence rates for dual seropositivity were from Emure (0.00%, n=20) and Irepodun (0.00%, n=27), and Ekiti-west (15.79%; 95% CI 9.99%,21.59%; n=152) LGAs, respectively.
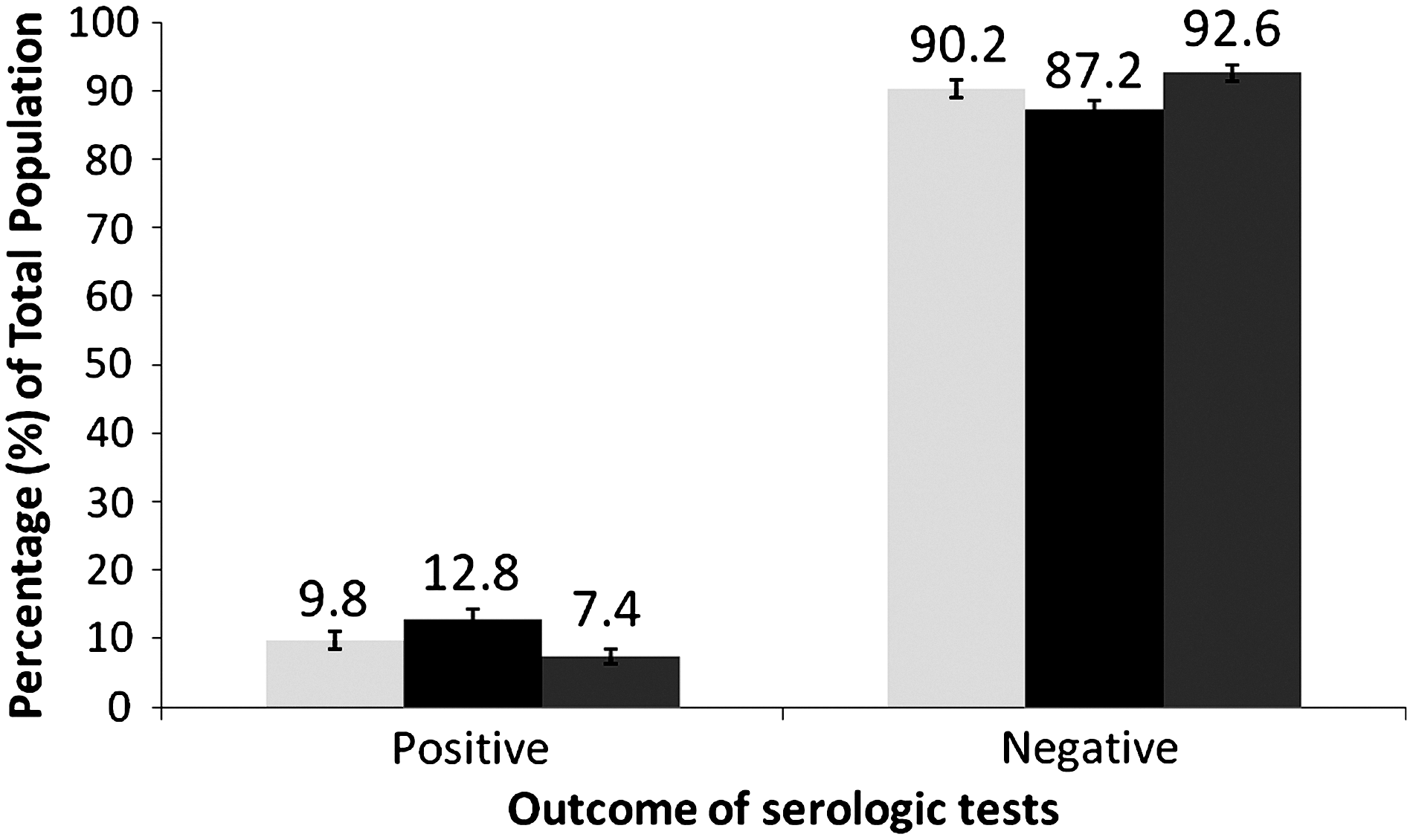
Overall prevalence rates for HBsAg positivity, anti-HCV antibody positivity, and dual positivity, among the study participants in Ekiti State, Nigeria, 2009 (blue, HBsAg; red, anti-HCV antibody; green, dual HBsAg/Anti-HCV antibody; vertical bar=95% CI).
Variables that were independently associated with dual HBsAg-anti-HCV antibody positivity are shown in Table 2, while those associated with each virus' single seropositivity are shown in Table 3.
Discussion
We observed that of the 2000 study participants, 7.40% (148) had dual infections. The non-overlapping bars of 95% CI show that significant differences existed between the dual positivity, HBV, and HCV prevalence rates. This implies that study participants were most likely to be anti-HCV antibody-positive, and least likely to have dual infections (Fig. 1). The point estimate of 7.40% for dual positivity lies outside the approximate range of 10–15% among CHB patients who also had HCV infection in Spain (32), Italy (21), Japan (33), Taiwan (34), and Iran (35). The rate recorded in this study was higher than the 0.3% (n=1500) dual infection rate found in southwestern Greece among the general population and selected groups (36), and was also higher than the 5.8% (n=1257) reported by Bini and Perumalswami (20) in the U.S. The dual infection rate recorded in this study was, however, lower than the 11.1% (n=207) documented by Cohan et al. (37) in Iran. Many reasons have been cited for the different rates, including differing geographic locations and time points of testing, and the types of kits and markers used for the detection of antigen/antibodies (45).
With regard to demographic variables, we observed the lowest dual infection rate among those with tertiary educations, and the highest rate among illiterates (Table 2). Analysis of the interaction of educational status and dual positivity notably showed that illiteracy was the overall strongest factor independently associated with dual positivity. Mehmet et al. (38) once found educational level to be a risk factor for contracting HBV. Since tertiary education apparently correlates with a high level of enlightenment, we inferred this as the reason for the lowest dual prevalence rate among those with a tertiary education, despite the fact that they constituted the majority of the study participants. One reason for the higher prevalence rate seen in our study compared to some others is that ours was a health-facility-based study, and this is where our patients were recruited. Other reasons for the higher or lower prevalence rates of these viral infections in this study compared to other studies might be the higher level of illiteracy, as illiterates are more likely to be involved in sharing sharp objects and shaving equipment, they are more likely to be involved in unsafe sexual practices (44), and they may have less adequate HBV vaccination (46). We therefore suggest an educational campaign regarding routes of transmission and acquisition of HBV and HCV to help people institute adequate preventive measures.
Analysis of the number of sexual partners showed a strong association with dual positivity. The participants that had one sexual partner constituted the bulk of this category (Table 2), and dual positivity increased as the number of sexual partners increased, with those having one or two being statistically comparable in dual prevalence rate. This observation has previously been reported (20). The respondents with ≥4 sexual partners were more than nine times more likely to have dual positivity compared to those with 1 or 2 sexual partners. We therefore inferred that the sexual route was a significant means of the spread of these viruses among the study participants.
The age of the study participants was also found to be independently associated with dual positivity, as previously observed (20). Although the transmission of HBV and HCV is not exclusively limited to those practicing unprotected sexual intercourse, the observation that dual positivity increased with increasing age (although there was a slight drop at age ≥55 y) was strange, as one would expect that those who are more sexually active (i.e., aged ≤34 y) should have a higher rate of dual infection (Table 2). One reason for this might be that subjects who were aged ≤34 y were students with a tertiary education. It was noteworthy that those aged ≥55 y had higher dual positivity than those aged ≤24 y or 25–34 y. Based on these observations and the report of Donovan (39), that sexual transmission of HBV was relevant for adults in resource-poor countries, we further inferred that sexual intercourse contributed significantly to the exposure of those who were dual positive.
Analysis of occupation revealed an independent association of this variable with dual positivity. We observed that though students comprised the majority of this category, they had the lowest dual positivity rate (Table 2). From the educational status, we inferred that the bulk of the students might be those with a tertiary education. Farming was the occupation with the highest dual positivity rate. In Nigeria, the majority of farmers (and those in trade/artisanship) are illiterate; this further corroborated the finding that a low educational level had a significant association with dual infection. Wasfi and Sadek (2), and Ophori et al. (40), also reported occupation as a pertinent risk factor.
The use of condoms during sexual intercourse was also independently associated with the prevalence of dual positivity. A limitation here was that we did not ascertain whether or not the use of condoms was with participants' spouses or with others. Those who responded “not at all” comprised the majority, and expectedly had the highest dual positivity rate. Though those who responded “at times” had higher a dual positivity rate than those who responded “always,” their dual prevalence rates were statistically comparable (Table 2). Our observation that those who responded “always” also had dual infections, though with the lowest dual positivity rate, made us suggest that the use of condoms during sexual intercourse was not foolproof, and that sexual contact might not be the only mode of acquisition of HBV and HCV among the study participants. Inappropriate use of condoms during sexual intercourse might also be contributory. In addition, we observed that 50.63% (642) of those who responded “not at all” to using condoms were married, a factor found to be associated with dual positivity in this study (Table 2). Not using condoms during sexual intercourse was therefore observed to be a risky sexual behavior, as previously reported (41).
We also observed an independent association of LGA with dual positivity. Study participants from Ekiti-west, Ido, Gbonyin, and Ado LGAs had about a 2–4 times higher likelihood of having dual positivity compared to those from Oye LGA (Table 2). Reasons for this might include the differences in sample sizes from the different LGAs, and the rural nature of many of the LGAs in Ekiti State (Table 1). Al-Faleh et al. (47) and Wasfi and Sadek (2) reported that residents of urban areas had higher HBsAg prevalence rates than those in rural areas. The reasons for this might include the high-risk behaviors such as unsafe injection and sexual practices that are more common in urban areas. The participants from the other LGAs were comparable in dual positivity rates to those from Oye LGA. Though studies revealing an association of dual infection with environment are scarce, Gogos et al. (36) observed an independent association of environment with HBV infection, while Ho et al. (42) reported that residing in and numbers of years of residence in villages were associated with anti-HCV antibody positivity.
With regard to marital status, unmarried single (presumably students) constituted the majority of the study participants, and had dual positivity rates statistically comparable to those who were separated/divorced/widowed. The married participants had the highest dual positivity rates, and were more than three times more likely to have dual HBV-HCV infection compared to separated/divorced/widowed and unmarried single persons (Table 2). From the earlier stated observations, these married persons probably belonged to the ≥35 y age group, the farming group, or those involved in trading/artisanship, who in Nigeria usually have low educational status, and as such were more likely to engage in unprotected sexual intercourse. Being divorced/separated was once reportedly associated with HCV infection (41), but in this study, it was being married that was strongly associated with dual positivity.
A history of blood transfusions was also independently associated with increased prevalence of dual positivity. This agreed with the results of Motta-Castro et al. (43), who reported this as a risk factor for HBV infection. Though those who responded “yes” to previous blood transfusions were lower in proportion, they had a significantly higher rate of dual infection (Table 2). This suggested that previous blood transfusion might be a means of contracting either virus. Alter et al. (41) reported a strong association of the receipt of a blood transfusion before 1990 with HCV infection. In the same vein, Reddy et al. (27) observed that the risk of dual HBV-HCV infection was greater among chronic renal failure patients, due to the frequent exposure to blood from transfusions and extracorporeal circulation during hemodialysis. However, Bini and Perumalswami (20) observed no association between blood transfusion prior to 1992 and dual HBV-HCV infection in the U.S. There were suggestions that prior to the advent of HIV/AIDS, there was no routine screening of blood and blood products from donors before transfusion. There were reports that infectious diseases transmissible through blood transfusions were highly prevalent in Africa, and in 2004 donated blood was not screened in 7% of countries for HIV/AIDS, in 22% of countries for hepatitis B, and in 51% of countries for hepatitis C (48,49). This might be another reason for the higher rate of viral infections found in this study compared to others. However, screening of blood and blood products from donors is routinely done in all blood banks and in most health care facilities in Nigeria before transfusion. This study therefore further reinforces the routine and compulsory screening of all blood and blood products before transfusion or organ transplantation.
The proportions of males and females with dual HBV-HCV infection observed in this work were higher than the 6.1% and 2.4%, respectively, by Bini and Perumalswami (20) in the U.S. Contrary to their observations, we observed that male gender was independently associated with dual prevalence (Table 2). A plausible explanation for this was not immediately apparent, as we noted that both studies involved higher numbers of males than females. Fejza and Telaku (24) also observed that males had higher dual HBV-HCV prevalence, but this was among voluntary blood donors. More frequent visits to barber shops, the sharing of sharp objects or shaving equipment, and a higher likelihood of being wounded, have been cited as possible reasons for the higher prevalence of hepatitis viral infections seen among males (2).
That “prior sexual intercourse” as a variable (Table 2) had no association with the dual prevalence rate appeared plausible, as the hepatitis viruses are not exclusively spread through unprotected sexual intercourse. This observation accentuated the contributions of other transmission routes.
We attempted the analysis of variables independently associated with either virus' prevalence rate, and observed that the strongest factor remained illiteracy. Table 3 shows these results.
In conclusion, Ekiti State, Nigeria, is highly endemic for HBV, and has a relatively high prevalence rate for dual HBV-HCV infection. Nine demographic factors were independently associated with dual infection, and eight were associated with monoinfection (Table 2), with educational status being the strongest factor. Based on our analysis, the most probable route of transmission/acquisition of HBV or HCV was sexual intercourse. In view of the report that co-infection of either HCV or HBV with HIV was independently associated with progressive chronic kidney disease among HIV-positive adults receiving combination antiretroviral therapy (50), and the other health risks posed by HBV and/or HCV in non-HIV-infected people, we recommend scaling up HB vaccinations, as well as a sustained educational campaign about the modes of transmission and acquisition of HBV and HCV, to minimize the spread of these viruses in Ekiti State, Nigeria.
Footnotes
Acknowledgments
We acknowledge the support of the management and staff of the health centers used for this study. We also appreciate the information provided by the Ekiti State Ministry of Information.
Author Disclosure Statement
No competing financial interests exist.