
Abstract
The role of CMV in ANCA-positive vasculitis is controversial. A 40-year-old man, with an unremarkable medical history, presented with progressive muscle weakness of all four limbs, accompanied by diffuse myalgia, arthralgia, and a 10 kg weight loss 2 months before admission to the Neurology Department of our hospital. Clinical examination revealed a flaccid tetraparesis with absent reflexes on the lower limbs and marked muscle atrophy. Electrophysiological investigations were consistent with a demyelinating motor polyradiculoneuropathy. Laboratory data showed AST=1137 IU/L (normal<37 IU/L), ALT=582 IU/L (normal<41 IU/L), C-reactive protein (CRP)=19 mg/L (normal<8 mg/L), CPK=13779 IU/L (normal<397). and LDH=911 IU/L (normal<192). CMV ELISA (serum) was strongly positive and CMV DNA by polymerase chain reaction (PCR) in blood and CSF also was positive. Immunologic screening revealed positive anti-myeloperoxidase antibodies anti-MPO=56,9 IU/mL (normal <9 IU/mL; ELISA). The inflammatory process involving the vessel walls and muscle fibers was histologically found in biopsy specimen of the muscle, with positive staining for CMV. The patient was treated initially with corticosteroids and intravenous immunoglobulins, but these therapies had very poor effect. Immunosuppressive therapy was instituted, resulting in a progressive partial recovery of all four limb weakness without relapses. We hypothesize that the CMV infection triggered an ANCA-positive vasculitis and its particular severe neurological involvement. An awareness of the association between CMV infection and vasculitis may have important therapeutic consequences.
Case Report
Neurologic symptoms consisted of progressive weakness in both lower limbs, for the last 2 months, causing progressive difficulty in walking and unsteadiness of gait, which gradually came up to the upper limbs without paraesthesiae, and bowel and bladder disturbances. The upper limbs were involved 15 days later, accompanied with diffuse myalgia, arthralgia, and a 10 kg weight loss.
Physical examination revealed a temperature of 37.3°C, blood pressure 135/94 mmHg, respiratory rate 16 breaths per minute, and heart rate 87 beats per minute. He was alert and there was no evidence of meningism.
Upon neurological examination, the patient was unable to stand and had weakness of all four limbs (motor grade 2/5). Muscle tone of the limbs was decreased. Deep tendon reflexes were diminished on the upper limbs and absent on the lower limbs, no pathological reflexes were elicited. The abdominal skin and cremasteric reflexes were present. The pinprick, light touch, and vibration senses were intact. Rectal tone and perianal sensation were normal. There was diffuse atrophy of limb muscles. The optic fundi, pupils, pupillary responses, external ocular movements, and cranial nerves were all normal. Finger-to-nose and heel-to-knee manoeuvers were accurate. Abdominal examination found moderate hepatomegaly. Heart and lungs were within normal limits.
The neurological examination indicated a motor polyradiculoneuropathy that was more evident in the lower limbs, with diffuse atrophy of limb muscles. Nerve conduction studies were consistent with a demyelinating motor polyradiculoneuropathy: motor nerve conduction velocities were delayed with elongated distal and F latencies, and myogenic records. Motor action potential and sensory action potential amplitudes were normal. The CPK and LDH levels were 13779 IU/L (normal<397) and 911 IU/L (normal<192), respectively.
The cerebrospinal fluid (CSF) was clear, colorless, and under normal pressure, with 1 white blood cell/mm3, glucose of 49 mg/dL, and protein of 28 mg/dL. Gram stain and subsequent CSF culture were negative.
Laboratory tests showed: AST=1137 IU/L (normal<37 IU/L), ALT=582 IU/L (normal<41 IU/L), alkaline phosphatase=80 IU/L (normal<128 IU/L), gamma-glutamyl transpeptidase=10 IU/L (normal<50 IU/L), C-reactive protein (CRP)=19 mg/L (normal<8 mg/L), serum albumin=8 g/L (normal >35 g/L), creatinine=4 mg/L (normal>6 mg/L), low C3 and C4 fractions of complement, and normal urine analysis. An extensive immunological work-up revealed: rheumatoid factor (-), anti-nuclear antibodies (-), cryoglobulin (-), positive antineutrophil cytoplasmic antibodies (ANCA) with a serum titer of 40 IU/mL (normal<20 IU/mL; indirect immunofluorescence assays). Serum titers were 56.9 IU/mL (normal<9 IU/mL; ELISA) for myeloperoxidase-antineutrophil cytoplasmic antibody (MPO-ANCA), and 1 IU/mL (normal<3.5 IU/mL; ELISA) for proteinase 3-antineutrophil cytoplasmic antibody (PR3-ANCA). Results of complete blood count testing, urea and electrolytes, prothrombin time, and partial thromboplastin time were within normal limits. Abdomen computed tomodensitometry (CT) disclosed a homogeneous hepatomegaly.
The results of serological tests for HIV ELISA, hepatitis A IgM, hepatitis B surface antigen, hepatitis C virus, herpes simplex viruses (HSV), varicella-zoster virus (VZV), and Epstein-Barr virus were negative. Initial CMV serology by ELISA was strongly positive for IgM antibodies. A second serological test for CMV one month later showed seroconversion with appearance of serum anti-CMV IgG antibodies (17693 IU/mL), using a commercially available ELISA kit. CMV DNA by polymerase chain reaction (PCR) in blood and CSF was positive. PCR tests for other viruses were all negative.
Histologic examination of the muscle biopsy showed an inflammatory process (lymphocytes and neutrophils) on the vessel walls and between striated muscle fibers (Fig. 1). High-power examination revealed thrombosis without fibrinoid necrosis, suggestive of vasculitis. Some of the endothelial cells presented the characteristic aspect of CMV infection, and CMV inclusions were noted (Fig. 2). Direct immunofluorescence showed immunoglobulin deposits.
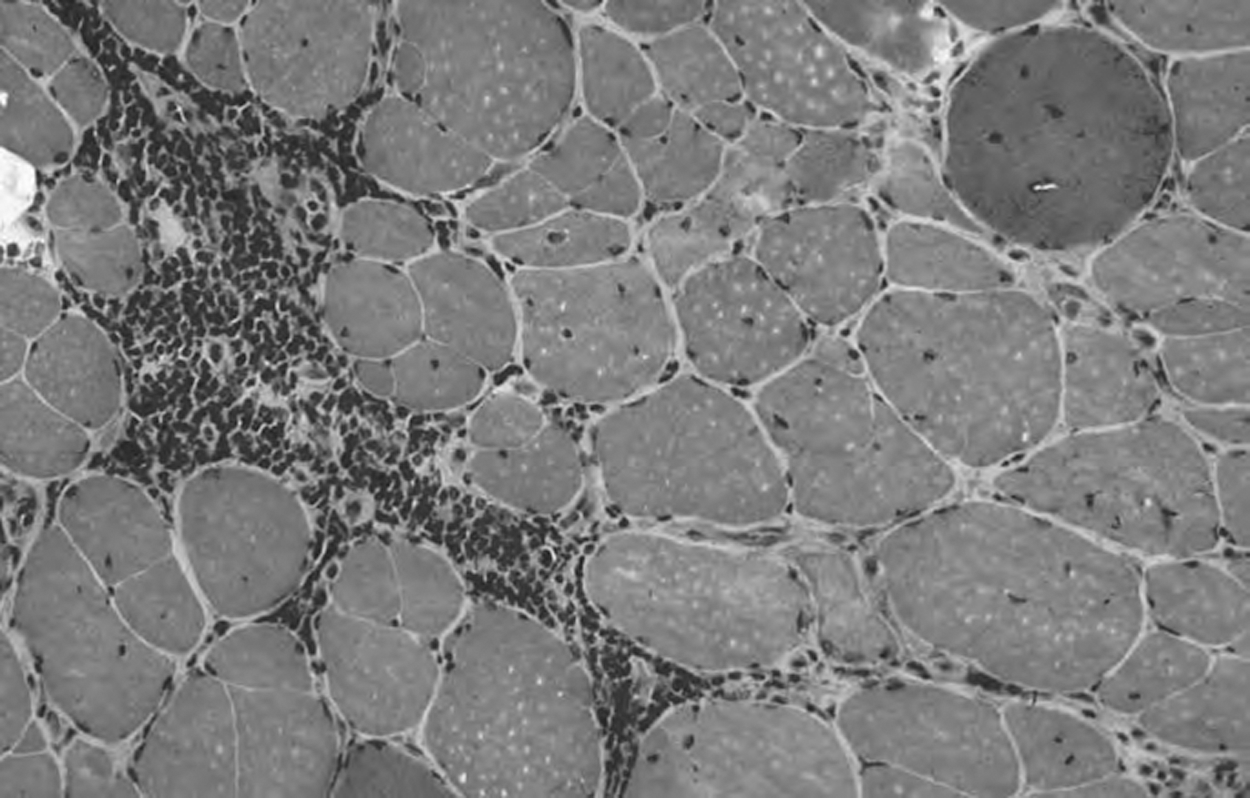
Muscle biopsy. Inflammatory process (lymphocytes and neutrophils) on the vessel walls and between striated muscle fibers. H&E stain. Medium magnification.
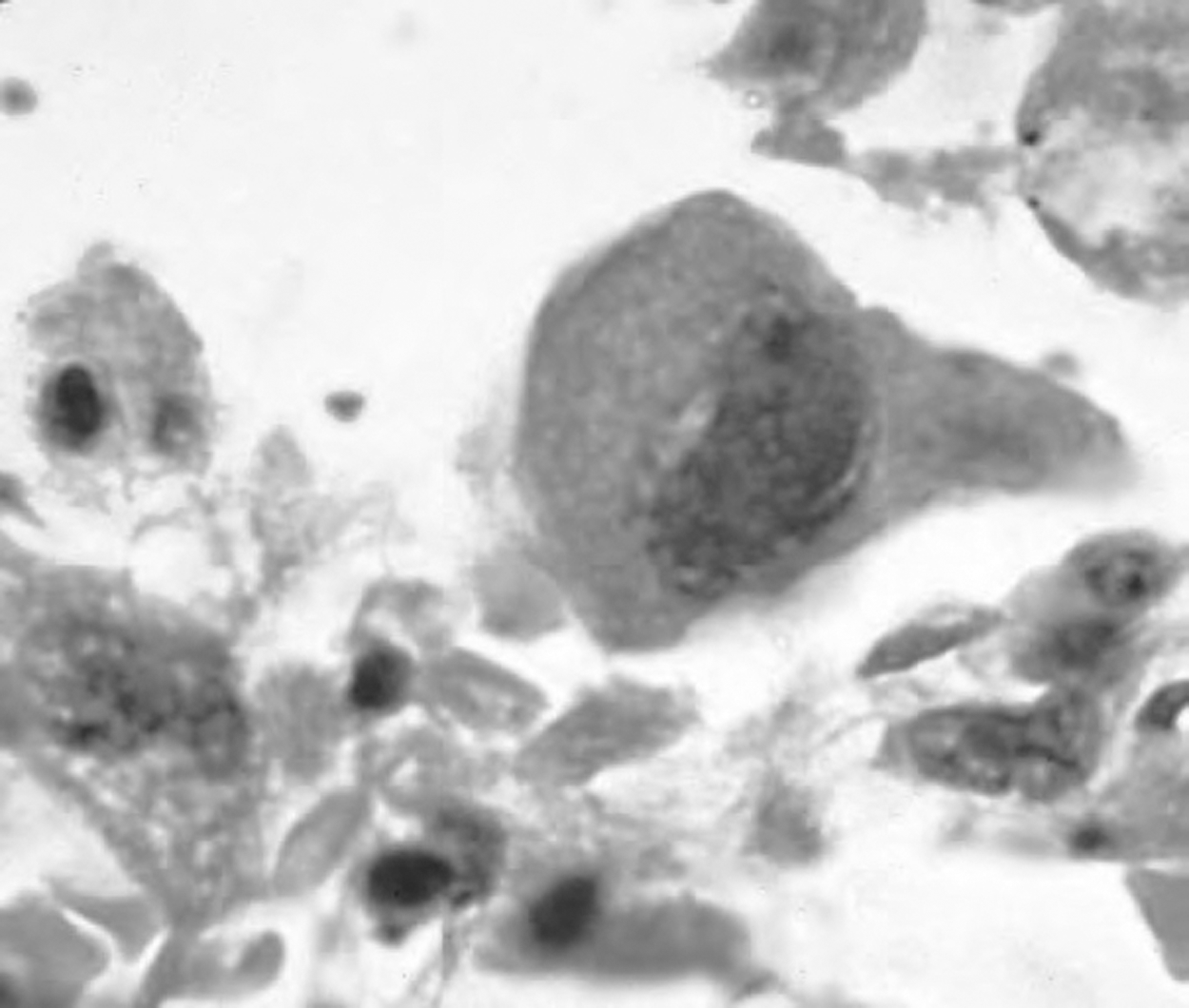
Characteristic aspect of CMV infection with both nuclear and cytoplasmic inclusions (X600).
Based on these findings, we made a diagnosis of acute neuromyositis complicating ANCA-positive vasculitis, combined with CMV liver injury, following cytomegalovirus infection in an immunocompetent patient. A course of intravenous immunoglobulins (0.4 g/kg/day) was instituted, and the patient was discharged after 5 days with little improvement. A high-dose of intravenous steroid therapy (6-methylprednisolone, 500 mg/day) for 6 days, followed by oral prednisolone (1 mg/kg/day) with gradual tapering over 6 weeks were instituted. Although, laboratory tests showed AST=464 IU/L, ALT=268 IU/L, CPK=9357 IU/L, and albumin=19 g/L, no clinical improvement was evident.
The patient was subsequently given a cyclophosphamide course (500 mg/m2 of body surface area), repeated every 2 months, for a total of 6 courses, resulting in a progressive partial recovery of all four limb weakness. The neurological sequelae were proximal muscle weakness (motor grade 3/5), absent ankle jerks with marked muscle atrophy. After the sixth pulse, laboratory findings showed AST=42 IU/L, ALT=38 IU/L, CPK=360 IU/L, albumin=32 g/L, CRP=5.9 mg/L, IgG anti-CMV=129 IU/mL, serum anti-CMV IgG antibodies=426 IU/mL, and anti-MPO=6 IU/mL.
Discussion
Symptomatic CMV infection in nonimmunocompromised hosts has traditionally been considered to have a benign, self-limited course. However, in the medical literature there are a considerable number of reports of severe clinical manifestations of CMV infection in immunocompetent patients. Those few patients who develop significant systemic disease and/or neurologic complications of CMV infection are far more likely to have an underlying reason (occult immunodeficiency, underlying chronic disease, or genetic susceptibility) (1 –4).
Thrombosis of the vascular system is one of the potential manifestations of CMV infection in patients with normal immune responses. Both local and generalized CMV infection resulted in vascular changes. Capillaries and small venules are the most targeted. Mononuclear cells are infected with the virus before endothelial cells, suggesting a role of mononuclear cells in transporting the virus, and thus, in spreading the infection. CMV directly invades vascular endothelial cells, causing membrane alterations that promote coagulation. CMV can also cause activation of vascular cells and the expression by the latter of adhesion molecules that react with platelets and leukocytes. Later changes include colonization of endothelial cells by CMV, frank vasculitis, and thrombotic occlusion. CMV infects endothelial cells, and the endothelium is a major reservoir of the virus during acute infection. Some evidence suggests that CMV may persist as a dormant virus in endothelial cells, being a source of subsequent reactivation. Superinfection with a different CMV strain may lead to development of IgM antibodies in previously IgG-seropositive patients. The CMV also increases the release of procoagulants, proinflammatory factors, and cytokines promoting endothelial cell proliferation and stimulating the expression of adhesion factors to the vascular endothelium. In addition, CMV-infected endothelial cells could be a target for natural killer cells, leading to further destruction of vessel surfaces (4 –9).
A systemic vasculitis can be triggered by CMV infection, complicating the differential diagnosis with other vasculitis. CMV may productively infect vascular endothelial cells, causing a local vasculitis and ischemia. This differential diagnosis is very important, since the cytotoxic treatment is less aggressive in such cases. Alternatively, the host immune response to cells expressing viral antigen may be the stimulus for vasculitis. Since there are no pathognomonic appearances to mucosal or cutaneous lesions, biopsy of accessible sites is critical for diagnosis and expeditious initiation of appropriate antiviral therapy. The CMV-associated vasculitides represent a broad spectrum of diseases. The vasculitis after CMV infection is diffuse and basically involves the digestive tract, notably the colon, the central nervous system, and the skin.
Cutaneous vasculitis associated with CMV seems to be a more fulminant disease, with the majority of cases having a fatal outcome. These differences likely reflect the degree of viral burden and the state of immune competence. Additionally, since the virus itself is immunosuppressive, host defenses may be further compromised by the infection. The vasculitis in our case could be the result of an autoimmune process, triggered by the infection of endothelial cells, since we detected CMV together with vasculitis in the occluded vessel. Although this causal link is suggestive, the relationship between CMV, vasculitis, and thrombosis remains uncertain. CMV-dependent induction of adhesion molecules on the endothelium surface and synthesis of chemokines primarily may play an important role in neutrophils recruitment and virus spreading from endothelial cells to neutrophils. It also is possible that these events could foster development of thrombosis by injuring the integrity of the endothelium (8.10–13). A case of multi-organ disease and CMV-associated cryoglobulinemic vasculitis type II was reported in 2006 by Kramer et al.(14). Although a large collective experience assessing the impact of ganciclovir and foscarnet is not currently available, both the prompt initiation of antiviral treatment and a concurrent reduction in any immunosuppressive regimen, including steroids, should be undertaken since these therapeutic strategies have clearly improved the outcome for other CMV syndromes. As the number of recipients rises and the HIV pandemic spreads, we are likely to see an increase in the number of cases of vasculitis associated with CMV infection (8 –13).
The association between CMV infection and antineutrophil cytoplasmic antibodies, was first described by Meyer et al. (10), in a patient with axonal polyneuropathy complicating a necrotizing vasculitis with fibrinoid deposits. The combination of ANCA-positive vasculitis and reactivated CMV infection may have contributed to injury of the vessel wall with subsequent development of thrombosis. Patients with ANCA-positive vasculitis and CMV infection should receive prophylactic anticoagulant therapy with heparin. Such prophylactic anticoagulant therapy with heparinoids likely may improve morbidity and could prevent potential life-threatening pulmonary embolism. A better awareness of this association could improve morbidity and may lead to prevention of potentially life-threatening symptoms or disabling sequelae. In 2007, an association between Wegener's granulomatosis, CMV infection, and thrombotic thrombocytopenic purpura has been described. Only one observation regarding a fortuitous association of microscopic polyangiitis (anti-myeloperoxydase) with CMV infection has been reported. Rare associations of CMV with polyarteritis nodosa have been reported in the literature (10 –12). A potential association between ANCA-positive vasculitis, reactivated CMV infection, and venous thrombosis has been also described in 2001 by Wolf et al. (11). In all these cases, the patients were immune-suppressed because of treatment for vasculitis, and CMV was mostly implicated as opportunistic pathogen; immunomodulators were reinitiated after control of CMV infection with antiviral treatment (13).
The European Vasculitis Study Group (EUVAS) (2011) studied the prevalence and characteristics of peripheral neuropathies occurring in antineutrophil cytoplasmic antibodies vasculitis in 506 patients. Peripheral neuropathy is an occasional event in antineutrophil cytoplasmic antibodies vasculitis, affecting essentially the motor nerves, without systemic involvement threatening vital prognosis. The chronic neuropathy is often associated with advanced age and low serum creatinine. The neuromyositis entity is often explained by the presence of nerve ischemia secondary to vasculitis (3 –5,9,12,13).
No comprehensive interpretation of the association of CMV infection and vasculitis is yet available. The CMV may be only an opportunistic pathogen, or a trigger of ANCA-mediated vasculitis (in a patient already at risk for such disease), or rather a primary cause of the ANCA-mediated response. Some data strongly support a causal relationship, owed to the CMV intrinsic procoagulant properties. However, it seems unreasonable to assume that CMV is either an opportunist or the primary cause, since such presentations as offered in this report are apparently quite rare, and primary CMV infection is quite common. The apparent connection of CMV with inflammatory vasculitis deserves further studies, as confirmation of true causality does not exist yet (7,12,13).
The data identified regarding the need for specific antiviral treatment in immunocompetent patients with severe CMV infection are conflicting, although current opinion is that CMV infection in immunocompetent patients does not require treatment. Other reports underline the importance of specific antiviral treatment in patients with severe CMV disease. Moreover, further discernment of the true impact of CMV on the patients' diseases is warranted, to ascertain which treatment approach is indicated: immunosuppression only, immunosuppression plus anti-CMV therapy, or anti-CMV therapy only. In the absence of careful clinical description of outcomes associated with each treatment modality, and randomized controlled trials, it is premature to discuss treatment recommendations. So, no definitive conclusions can be drawn about the potential benefit of antiviral therapy for severe CMV disease based on these uncontrolled reports. The risks and benefits of specific antiviral treatment for severely ill patients are not adequately addressed (4,6,8,10 –12).
E 9-(1,3-dihydroxy-2 propoxymethyl) guanine (DHPG) (Ganciclovir)R is started at a dose of 10 mg/kg/day in two doses. The main side effects of the treatment are represented by neutropenia, thrombocytopenia, and liver toxicity. These disorders are reversible after discontinuation of treatment. Prolonged treatment is important to prevent disease progression and relapse. Very rare cases of ganciclovir resistance were reported. The phosphonoformate (Foscarnet)R is started at a dose of 120 mg/kg/day. The maintenance dose is 60 to 90 mg/kg/day. The side effects are mainly represented by nephrotoxicity and bone marrow toxicity. Foscarnet is often reserved in cases of intolerance or nonimprovement after 2–3 weeks of treatment with ganciclovir (8,12,14,15).
The mortality rate during CMV infection is very important in immunocompromised patients. According to Goliatsatos et al., poor prognostic factors in immunocompetent individuals are age and co-morbidities (renal failure, diabetes). Our patient did not have co-morbidities, but it must be remembered that even short-term corticotherapy may worsen the disease (4 –6,11,12).
Conclusion
CMV infection in immunocompetent patients is usually transient and does not exhibit many symptoms. However, severe life-threatening complications of CMV infection in immunocompetent patients may not be as rare as previously thought. An awareness of the association between CMV infection and vasculitis may have important therapeutic consequences, although treatment strategy remains controversial because of the uncertainty of that association. Further studies are needed to assess the potential role of CMV in ANCA-positive vasculitis, and randomized controlled trials are needed for a more conclusive answer on whether the use of antiviral treatment is indicated for immunocompetent patients suffering from severe CMV infection.
Footnotes
Acknowledgments
Jawad Oumerzouk drafted the manuscript. O Qamouss, Y Hssaini, and A El Jouehari participated in the bibliographic research. Ahmed Bourazza participated in the bibliographic research and corrected the manuscript.
Author Disclosure Statement
The authors received no specific funding. All the authors are from the Department of Neurology and Pathology, in the Military Hospital of Rabat (Morocco), without conflict of interest or financial aid.