
Abstract
HLA-G is a class I HLA that has gained much attention due to its multiple functions in the immune system. More important, some studies found HLA-G may be detrimental in tumors and viral infections, and the detection of HLA-G expression might serve as a clinical marker in the prediction of clinical outcomes for certain types of carcinoma. We assessed the association between the development of Kazakh esophageal squamous cell carcinoma (ESCC) harboring high-risk HPV infection and the expression of HLA-G. The expression of HLA-G was detected by S-P immunohistochemical staining in 60 cases of Kazakh ESCC tissues and 40 cases of Kazakh tumor adjacent normal tissues. HPV16 infection in ESCC was detected by genotype-specific polymerase chain reaction. HPV16 infection rate in Kazakh ESCC was 35.0%, significantly higher than that of the infection rate of the adjacent normal tissues 15% (p<0.05, OR=3.051; 95% CI: 1.103–8.438). The expression of HLA-G in Kazakh ESCC was 75.0% (45/60), significantly higher than that of tumor adjacent normal tissues (17.5%; p<0.05); expression of HLA-G was slightly higher in HPV16-positive than HPV16-negative ESCC, but the difference was not statistically significant (p>0.05). The positive expression rate of HLA-G was closely related to depth of invasion and clinical stage (p<0.05 for all), but was not related to age, sex, tumor location, histologic grade, and nodal status (p>0.05 for all). Overexpression of HLA-G was a characteristic feature of Kazakh ESCC; HLA-G may be involved in Kazakh ESCC carcinogenesis and HPV infection.
Introduction
Several studies have demonstrated that high-risk human papillomavirus (HPV) infection is associated with esophageal carcinoma (particularly HPV type 16), especially in geographic areas with a high incidence of ESCC (23,24). In our previous study, we observed a significantly high prevalence of HPV infection in a case-control study (10,11). However, HPV infection may not be the only factor to cause tumor growth. Infected cells may develop mechanisms to escape from the immune response, leading to persistent HPV infection and oncogenic transformation.
HLA-G is a nonclassic major histocompatibility complex class Ib antigen, which was characterized by expression restricted to the fetal–maternal interface on the extravillous cytotrophoblast, and which has gained much attention due to its multiple functions on the immune system (2,20). Early studies found HLA-G had also a restricted distribution on some normal tissue cells, such as thymic epithelial cells, endothelium, activated monocytes, and erythropoietic lineage cells from the bone marrow (5). However, HLA-G has also been unexpectedly found in various types of human malignancies, including breast cancer (12), renal cell carcinoma (4), ovary cancer (14), gastrointestinal cancer (8), and colorectal cancer (26). HLA-G expression in virus-infected or malignant cells has also been associated with tumor progression and metastasis (5,19).
The aberrant expression of HLA-G in many human cancers exemplifies similar strategies used by the fetal–maternal interface, virus, and cancer to evade immune response. As other cancer types, esophageal carcinoma cells take advantage of a similar molecular strategy to escape from immune recognition in response to the expression of HLA-G antigens.
We performed a case-control study to investigate whether HLA-G is associated with HPV infection and the occurrence and progression of Kazakh esophageal squamous cell carcinoma (ESCC) in Xinjiang, China, and whether the expression of HLA-G in Kazakh ESCC can be used as a reliable clinical marker in the prediction of clinical outcomes of the disease.
Materials and Methods
Study population
Sixty Kazakans specimens were collected between 2004 and 2010. The patients, aged 34–76 years old (36 men and 24 women), were diagnosed with esophageal squamous cell carcinoma (ESCC) and did not received preoperative radiotherapy or chemotherapy. At the same time, 40 specimens were collected from Kazakans cancer adjacent normal esophageal biopsy tissues as controls. The control group were aged 32–73 years old (24 men and 16 women). All specimens were recruited from Department of Yili Friendship Hospital, Xinjiang, China, where the biopsy paraffin-embedded tissues were prepared. Each participant provided written informed consent; the study was approved by the participating hospital.
Conventional hematoxylin and eosin (HE) staining was used for all specimens. Two pathology experts confirmed all the cases by light microscopic observation and analysis of the histopathological changes of the HE-stained slides according to esophageal pathological diagnosis criteria as referenced in "World Health Organization (WHO) Classification Tumors of the Digestive System" (22). Based on the WHO classification criteria, 24 patients were classified as well-differentiated squamous cell carcinoma, and 36 as moderately and poorly differentiated squamous cell carcinoma. In the control group, all specimens were confirmed adjacent normal esophageal mucosa to the cancer.
Immunohistochemical analysis
After the paraffin-embedded tissue blocks were cut into 4-μm thick sections and mounted on polylysine-coated slides, they were dewaxed in xylene and rehydrated through a graded series of ethanol. After deparaffinization, endogenous peroxidase activity was blocked by a 3% peroxide-methanol at room temperature for 10 min. Antigen retrieval was performed at 100°C (in an autoclave) for 7 min in a 10 nmol/L sodium citrate buffer (pH 6.0). Afterwards, sections were incubated with goat serum to block nonspecific adsorption at room temperature for 10 min. Sections were then incubated with the primary anti–HLA-G monoclonal antibody (1:100) (CapitalBio, China) overnight at 4°C. Then a thorough washing in PBS was performed. Subsequently, binding sites of the primary antibody were visualized by using a DAKO EnVision kit (DAKO, Glostrup, Denmark) in accordance with the manufacturer's instructions. Finally, sections were faintly counterstained with hematoxylin and mounted with glycerol gelatin. Per reactions were set each positive control (HLA-G+ control sample) and negative control (PBS).
Evaluation of staining
All sections were analyzed under a light microscope by two experienced pathologists. Results were scored as positive or negative by the percentage and intensity of positive cells. The percentage of positive was scored as 0 for no staining, 1 for less than 25% staining cells, 2 for 25%–50%, and 3 for more than 50% staining intensity of staining was scored as 0, 1, 2, or 3 according to absent, weak, clear, or strong expression. The staining results were divided into three categories based on the sum both scores: 0 was negative (-), 1–2 was weak positive (1+), 3–4 was moderate positive (2+), and 5–6 was strong positive (3+).
DNA preparation
Methods to minimize the possibility of tissues contamination for patient cases and controls group were as follows: Briefly, each formalin-fixed and paraffin-embedded sample was cut into 7 μm thick sections, 10–15 slides were dropped into a new high pressure EP-tube, the blade was disinfected with 75% medicinal alcohol before the sample cut. With every 5 samples, we used no tissues paraffin-embedded sample to cut for no contamination control. Then genomic DNA was isolated from the paraffin-embedded tissues by the phenol–chloroform method (21), and dissolved in sterile double-distilled water 12 ∼ 24 h, and refrigerated at −80° to preserve it.
HPV16 typing
Before HPV16 detection, we used β-globin signals to confirm sample DNA quality and chose strong β-globin samples to genotype. HPV-DNA was detected by primer polymerase chain reaction (PCR). Each reaction includes a positive and a negative control. The positive control was CaSki cell DNA (generously provided by Professor Yang Ke, Beijing Institute for Cancer Prevention Laboratory). Primers for HPV16 E6: FOR 5′-GACCCAGAAAGTTACCACAG-3′, RER 5′-CACAACGGTTTGTT GTATTG-3′ (primers synthesis from Shanghai Health Industrial). PCR reactions were as follows: predegeneration 94° 3 min; degeneration 94° 45 sec, annealing 55° 45 sec, an extension of 72° 45 sec, a total of 35 cycles.
Statistical analysis
The software SPSS version 13.0 was employed for all statistical analyses. Correlations between the degree of staining and the subgroups according to the clinicopathologic classifications and HPV16 infection were calculated by using the Pearson χ2 test. Odds ratios (OR), confidence intervals (CI), and p values were calculated by the Epi-Info program. P values less than 0.05 were considered significant.
Results
The ß-globin PCR results show that all specimens had sufficient quality for HPV16 analysis. 35.0% were HPV16 positive, significantly higher than 15.0% of the control group (OR=3.051; 95%CI: 1.103–8.438; p <0.05) .
Immunohistochemistry showed diffuse staining of the membranes and cytoplasm of tumor cells (see Fig. 1). HLA-G protein was observed in 45 (75.0%) of 60 malignant tissues, 28 (65.1%) expressed moderate or strong (2+/3+), 17 (28.3%) expressed weak (1+) in ESCC, and only 15 cases of ESCC (34.9%) were negative for HLA-G. HLA-G protein was observed in 7 (17.5%) of 40 normal esophageal tissues adjacent to the cancer, and all 7 cases expressed weak (1+). The expression of HLA-G protein in ESCC was higher than that of normal tissues (p<0.05), see Table 1.
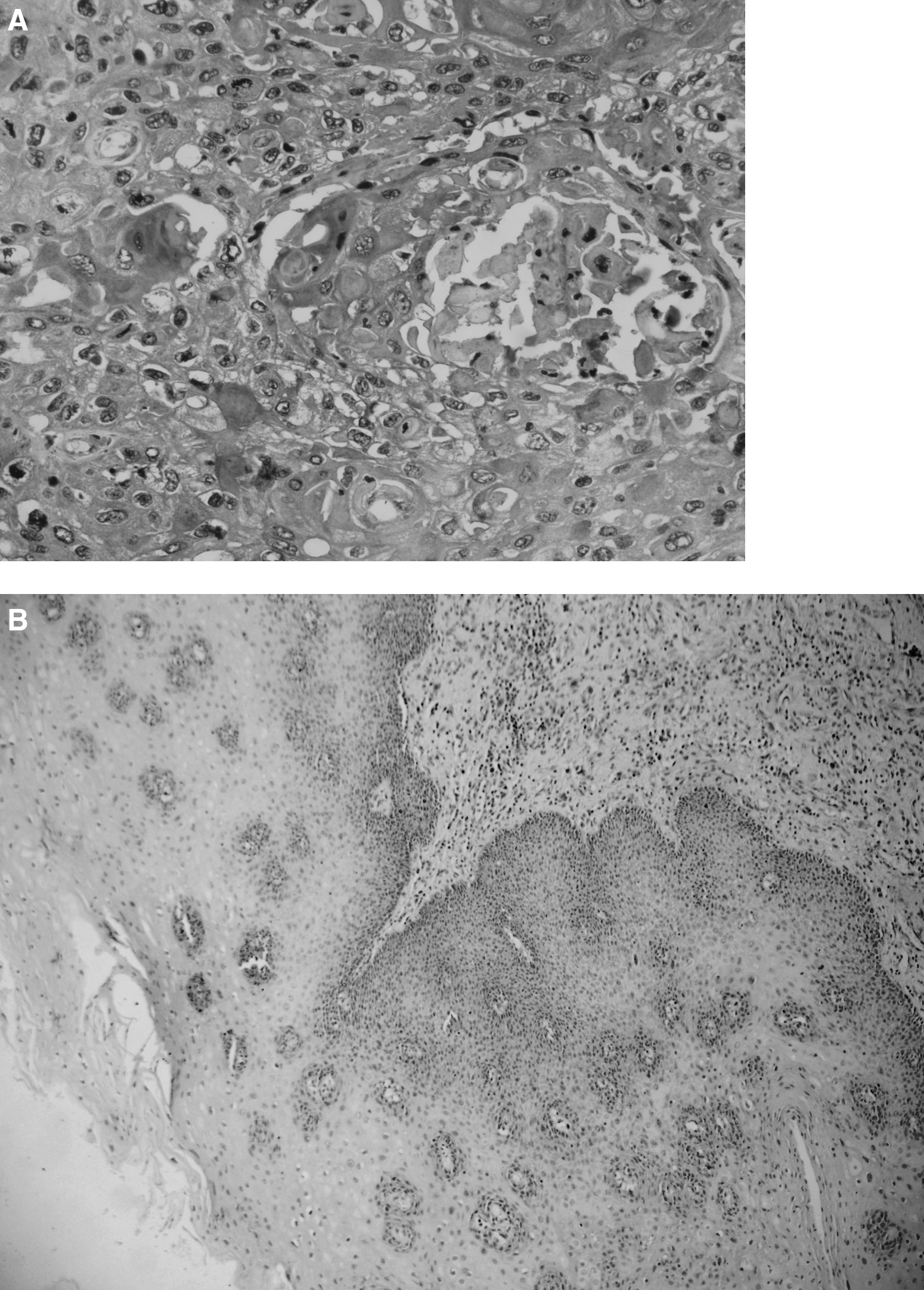
Immunohistochemical staining of esophageal squamous cell carcinoma.
ESCC, esophageal squamous cell carcinoma; HLA-G, human leukocyte antigen-G; HPV, human papillomavirus.
The weak (1+) positive expression of HLA-G in ESCC was higher than that of normal tissues (p=0.002). 2The moderate or strong (2+/3+) positive expression of HLA-G in ESCC was higher than that of normal tissues (P=0.000).
Expression of HLA-G among HPV16-positive and HPV16 negative ESCC is show in Table 2. Of the 21 patients with HPV16-positive ESCC, 4 showed weak expression of HLA-G, 11 demonstrated moderate or strong expression of HLA-G. Of the 39 patients with HPV16-negative ESCC, 11 had weak expression of HLA-G, 17 showed moderate or strong expression of HLA-G. We found the moderate or strong (2+/3+) expression of HLA-G was higher in HPV16-positive than HPV16-negative ESCC, the weak (1+) expression of HLA-G was higher in HPV16-positive than HPV16-negative ESCC, but the differences were not statistically significant (p>0.05 for all).
ESCC, esophageal squamous cell carcinoma; HLA-G, human leukocyte antigen-G; HPV, human papillomavirus.
The weak (1+) expression of HLA-G in HPV16-positive ESCC was higher than HPV16-negative ESCC group; 2the moderate or strong (2+/3+) expression of HLA-G in HPV16-positive ESCC was higher than HPV16-negative ESCC group. But those are not statistically significant.
To assess the role of HLA-G expression in ESCC, we calculated the correlations between HLA-G expression and the clinicopathological parameters, including age, gender, tumor location, histological grade, depth of invasion, nodal status, and the clinical stages. We found overexpression of HLA-G was significantly correlated with aggressive clinicopathologic characteristics, including depth of invasion and clinical stages (p<0.05). However, no significant correlation was found between HLA-G expression and other parameters (p>0.05), Table 3.
p<0.05.
Discussion
In our study, the HPV16 virus infection rate in patients of ethnic Kazak esophageal cancer was significantly higher than Kazakh cancer adjacent normal esophageal tissues. It therefore has been proposed that HPV16 infection may play a role in esophageal carcinogenesis. A similar observation was also revealed in previous studies (7,10). It was considered by some investigators that HLA-G was closely related with HPV infection in early studies (6).
HLA-G has an important role in immune response and immune regulation to HPV infection and tumor. Early studies showed that HLA-G inhibited NK cell and T cell-mediated cytolysis by suppressing CD4+ T-cell (1,13). HLA-G was also found to induce the development of tolerogenic dendritic cells that promote the differentiation of both anergic and regulatory (suppressor) CD4+ and CD8+ T cells (18). In addition, HLA-G can also induced Th2 cytokine (IL-4, IL-5, IL-10) polarization, prompted auxiliary T cells cytokine (Th1, Th2) balance toward Th2, and reduced the immune response of Th1 cells (15,17). Finally, HPV and cancer cells could escape from the host's immune monitoring and killing.
This study found HLA-G protein was expressed by 43 (71.7%) of 60 in Kazakh ESCC, of which 28 (65.1%) expressed moderate or strong (2+/3+), 15(34.9%) expressed weak(1+) in ESCC, and only 17 cases of ESCC (28.3%) were negative. The expression of HLA-G protein in ESCC was higher than that of normal tissues (4%) (P<0.05). The results are similar to those in patients with hepatocellular carcinoma and ovarian cancer (14,25). Expression of HLA-G may afford a potent mechanism of immunologic tolerance by tumor cells. In addition to its potential expression, it may be used as a marker to distinguishing ESCC and normal tissues. When comparing the expression of HLA-G among HPV16-positive and HPV16-negative ESCC, we found the moderate or strong expression of HLA-G was higher in HPV16-positive than HPV16-negative ESCC, but the differences was not statistically significant. These results suggest that HLA-G expression in Kazakh esophageal lesions is associated with cancer progression but not with HPV16 infection. Some studies showed that HLA-G expression in HPV16- and HPV18-positive tumor were higher than that of negative ones, especially in cervical cancer (6). To explain these differences in the reports, the mechanism of HPV infection and integration into the host genome in different types of cancer might be cited as potential causes of inconsistency.
Whether HLA-G expression has close relationship with development of Kazakh ESCC progression, we found overexpression of HLA-G was significantly correlated with aggressive clinicopathologic characteristics, including depth of invasion and clinical stages (P<0.05), especially in moderate and strong expression of HLA-G. The results are partly similar with reports by Yie in gastric cancer and colorectal cancer (8,26).Our findings indicated that overexpression of HLA-G might be a useful marker to identify patients with more aggressive Kazakh ESCC. It is also suggested that overexpression of HLA-G may provide an opportunity for ESCC cells to escape immunological surveillance, and promote the development of ESCC progression.
A limitation of this work is our relatively small number of samples. A larger cohort of samples might substantiate these data. Another limitation is the lack of cancer patient overall survival rate, which may better help us to assess the interaction between HLA-G expression and prognosis in Kazakh ESCC.
Footnotes
Acknowledgments
This work was supported by Ministry of Science and Technology of China (Nos. 2012AA02A503, 2009BAI82B03 and 2010DFB34100), and The National Natural Science Foundation, No.81160301.
Author Disclosure Statement
The authors have no financial conflict of interest.