
Abstract
Vaccination against hepatitis A is an important intervention to prevent disease in HIV-patients. There are insufficient data on the association of the response to hepatitis A vaccine with immunological parameters, including subpopulations of T-cells. We studied HIV-infected adults with CD4 T-cells>200 cells/mm3 who received two doses of hepatitis A vaccine (Havrix or Vaqta). The counts of CD3, CD4, CD8, CD4+T-cells, NK, NK CD8+, NK CD8 – cells, and HIV RNA were measured at the time of first dose administration and one month after the end of the vaccination period. The geometric mean titer of antibodies to hepatitis A virus (anti-HAV) and factors affecting response were evaluated. 113 patients (50 antiretroviral treatment-naïve and 63 treatment-experienced) were enrolled in the study. There was no change in the immunological parameters and in the HIV-RNA post-vaccination, except for a decrease in CD8 and in double positive CD4+CD8+t-cell count. The immune response and geometric mean titer of anti-HAV were similar among treated and naïve patients (78% vs. 76% and 237 mIU/mL vs. 158 mIU/mL). Vaccine response was achieved in 71% of patients with CD4=200–499 cells/mm3 compared with 80% of participants with CD4 ≥500 cells/mm3 (p>0.05). Logistic regression revealed that immunological cells tested do not affect response differently in treatment-naïve vs. experienced patients. The only factor affecting response is the CD4 T-cell count at vaccination (OR 1.320; 95% CI 1.052–1.656; p=0.016). Patients with CD4 T-cell count ≥500 cells/mm3 were 4.3 times more likely to respond to the vaccine than patients with CD4 T-cell count 200–499 cells/mm3 (p=0.005). In conclusion, successful vaccination is associated with CD4 T-cells. The count of other immune cells or the administration of antiretroviral therapy does not predict response to hepatitis A vaccine in HIV patient with baseline CD4 T-cell>200 cells/mm3.
Introduction
Hepatitis A virus (HAV) in patients with HIV-infection causes prolonged illness and therefore there is a potential increase in the transmission of HAV (12). In addition, hepatitis A concurrent with preexisting chronic hepatitis B or C in HIV-patients increases morbidity and mortality due to serious complications including fulminant hepatitis (31).
Vaccination remains the most effective intervention to prevent or mitigate disease. Hepatitis A vaccine is particularly important for patients with HIV-infection and is recommended for high risk groups, including men having sex with men (MSM), injection drug users, and individuals with chronic liver disease (7). However, as reported with other vaccines, the efficacy and safety of the vaccine might be decreased in HIV-patients.
The immunity provided by the hepatitis A vaccine comes from the neutralizing antibodies (29). T-cells participate in the immune response to vaccination, as they are essential for the induction of antibody responses. Subpopulations of T-cells are also important immunological parameters. T-cell subgroups in HIV-infected patients change during disease progression and improve with successful antiretroviral treatment and suppression of viral replication. Studies performed on vaccination against hepatitis A in HIV patients have suggested a relationship between seroresponse and baseline CD4 T cell count. Patients with advanced immunosuppression, low CD4-T cell count, and detectable HIV RNA, have especially poor and short-lasting antibody response to vaccination.
A study on more immune cell populations could provide interesting data both on the effect of the hepatitis A virus vaccine on HIV patients, as well as on the factors affecting immune response.
Methods
The study was reviewed and approved by the Ethics Committee of the “A. Sygros Hospital” in Athens, Greece. Before enrollment, all patients signed and gave an informed consent form. All subjects were HIV-infected MSM attending the AIDS clinic. The vaccine was administered as part of their clinical care, following screening for antibodies against hepatitis A. Participants received two doses of the vaccine (either Havrix [1440 El. U per dose, GlaxoSmithKline] or Vaqta [50 U per dose, Merck & Co]) with an interval of 6–12 months. These two vaccines are considered equivalent and can be used interchangeably.
All vaccinated patients had CD4 T-lymphocytes>200 cells/mm3 when they received the first dose of the vaccine (time of vaccination). Enrolled patients were either under Highly Active Antiretroviral Therapy (HAART-treated) with undetectable viral load at the time of vaccination or had never received antiretroviral therapy (HAART-naïve).Inclusion criteria included: no change or fail in antiretroviral therapy during study period.
The number of CD3, CD4, CD8, CD4+CD8+T-cells, NK, NK CD8+and NK CD8–cells was measured at the time of vaccination and 1 month following the administration of the second dose of the vaccine (complete vaccination), using flow cytometry.
The HIV viral load and antibody titer against hepatitis A virus (anti-HAV) were also determined. HIV-RNA was measured using NASBA Ultra sensitive which has a cut-off limit of 40 cop/mL. A commercial enzyme-linked fluorescent assay method (VIDAS Anti-HAV Total, Biomerieux, France) was used to measure anti-HAV titers. Seroconversion was set to occur when the HAV antibody titer was ≥20 mIU/mL. Additional data included: demographic characteristics, duration of antiretroviral treatment, time since HIV diagnosis, history of AIDS-related conditions, hepatitis B or C co-infection, nadir CD4 T-cell count, and viral load.
The Kolmogorov-Smirnov test was used to establish data normality at the statistical analyses. The analysis was based on parametric tests for data that were normally distributed, while nonparametric tests were used for abnormal data (Wilcoxon's test).
Univariate and multivariate logistic regression was used to explore the factors affecting response. Parameters that were evaluated included: CD4, CD3, CD8, CD4+CD8+T-cells, NK-cells, nadir CD4, and HIV-RNA. In this analysis, nondetectable viral load was equivalent to administration of HAART as all HAART-treated patient had HIV RNA<50 cop/mL.
Results
113 patients of Greek descent were enrolled in the study. At the time of vaccination (administration of first dose), 63 patients were receiving HAART, while 50 were HAART-naïve. The median time of taking antiretroviral therapy until the administration of the first dose of the vaccine was 8 years ((interquartile range IQR 4.0–11.5 years). Baseline demographic and immunologic characteristics are summarized in Table 1.
Categorical variables are shown as numbers (percentages) and continuous as medians (interquartile ranges).
At or prior the first dose of hepatitis A vaccine administration;
HAART=Highly Active Antiretroviral Therapy.
No significant changes in the CD3, CD4 T-cell count, NK-cell count and their subgroups, NK CD8- and NK CD8+cell counts were observed following vaccination. The CD3 T-cell count was 1977 cells/mm3 at the time of vaccination versus 1930.0 cells/mm3 1 month after the second dose, the CD4 T-cells count was 570.0 cells/mm3 versus 559.0 cells/mm3, the NK-cells count was 235 cells/mm3 versus 174.0 cells/mm3, the NK CD8+cells count was 132.0 cells/mm3 versus 116.5 cells/mm3, and the NK CD8-cells count was 61.0 cells/mm3 versus 53.0 cells/mm3.
There was a significant difference in the counts of CD8 T-cells and CD4+CD8+T-cells at the time of vaccination compared to the respective post-vaccination counts. The CD8 T-lymphocyte count at the time of vaccination was 1106.0 cells/mm3 (IQR 705.5–1431.0 cells/mm3) versus 942.5 cells/mm3 (IQR, 605.0–1274.0 cells/mm3) one month after the completion of vaccination (p=0.016). The CD4+CD8+T cell count was 3.0 cells/mm3 (IQR 1.0–6.0 cells/mm3) versus 2.0 cells/mm3 (IQR 1.0–3.5cells/mm3), p<0.0001.
After the end of vaccination, HAART-treated patients experienced a statistically significant decrease in CD8 T-cells and CD4+CD8+T- cells. On the contrary, no change was observed in the CD8 T-cell count and the CD4+CD8+T-cell count, in HAART-naïve patients. Other parameters did not change significantly in either of the groups (Table 2).
Variables are shown as medians [interquartile ranges].
HAART=Highly Active Antiretroviral Therapy; b At or prior the first dose of vaccine administration; cOne month after the second dose of the vaccine.
No particular change was observed in the HIV viral load. Patients on antiretroviral treatment remained with undetectable viral load (HIV RNA <50 cop/mL), while those who did not receive treatment had little variation: 7100 cop/mL (IQR 1200–31000 cop/mL) at vaccination versus 8350 cop/mL (IQR 1000–28500 cop/mL) one month after the second dose (log10 cop/mL: 3.8 versus 3.9).
One month following the second dose of the HAV vaccine, seroprotective anti-HAV antibody titers were measured in 78% (95% CI, 66%–87%) of the patients receiving HAART (49/63). Out of the 50 antiretroviral treatment-naïve patients, 38 responded to the vaccine (response rate: 76% [95% CI, 63%–86%]), p=0.826.
The geometric mean titer of anti-HAV antibodies was higher in patients under HAART than in those who were not receiving treatment (237 mIU/mL [95% CI, 201–321 mIU/mL] versus 158 mIU/mL [95% CI, 130–221 mIU/mL]). However, the difference was not statistically significant (p=0.068).
Response rate and GMT were also examined, stratified by the baseline CD4 T cells count. Participants with CD4 T-cell count between 200 and 499 cells/mm3 (n=42) at the time of vaccination had 71% (95% CI, 55%–83%) seroconversion rate versus 80% (95% CI, 70%–88%) of those with CD4 T-cell count ≥500 cells/mm3, (p=0.253).
In addition, patients with CD4 T-cell counts above 500 cells/mm3 at vaccination, had more robust GMTs than subjects with CD4=200–499 cells/mm3 (266 mIU/mL [ 95% CI, 198–358 mIU/mL] versus 150 mIU/mL [95% CI 113–200 mIU/mL]) However, neither the difference in response nor the GMT difference was statistically significant (p>0.05).
Fractional polynomial analysis revealed that immunologic parameters, except CD4 T-cell, have nonlinear relationships to response (Fig. 1a). Although in this analysis, the relation of the CD4 T-cell count with the probability of response was not statistically significant (p=0.101), determining the linear association there was a statistically significant relationship (p=0.041). CD3, CD8, CD4+CD8+, NK, and nadir CD4 T-cell count do not correlate with the probability of response. Nadir CD4 T-cells were examined as an example of an immunological parameter. Nadir CD4 T-cell count was measured using two independent variables in the model (nadir CD4 count and nadir CD4 count square root). Inverse U-shaped correlation was observed in the chart between the probability of response to the vaccine and nadir CD4 count. Considering the HIV viral load, there was no significant variation in the relationship between response and nadir CD4 count (p=0.842) (Fig. 1b). This outcome is also characterized the HAART administration because, in the present study, undetectable viral load was inextricably linked to the taking of antiretroviral treatment.
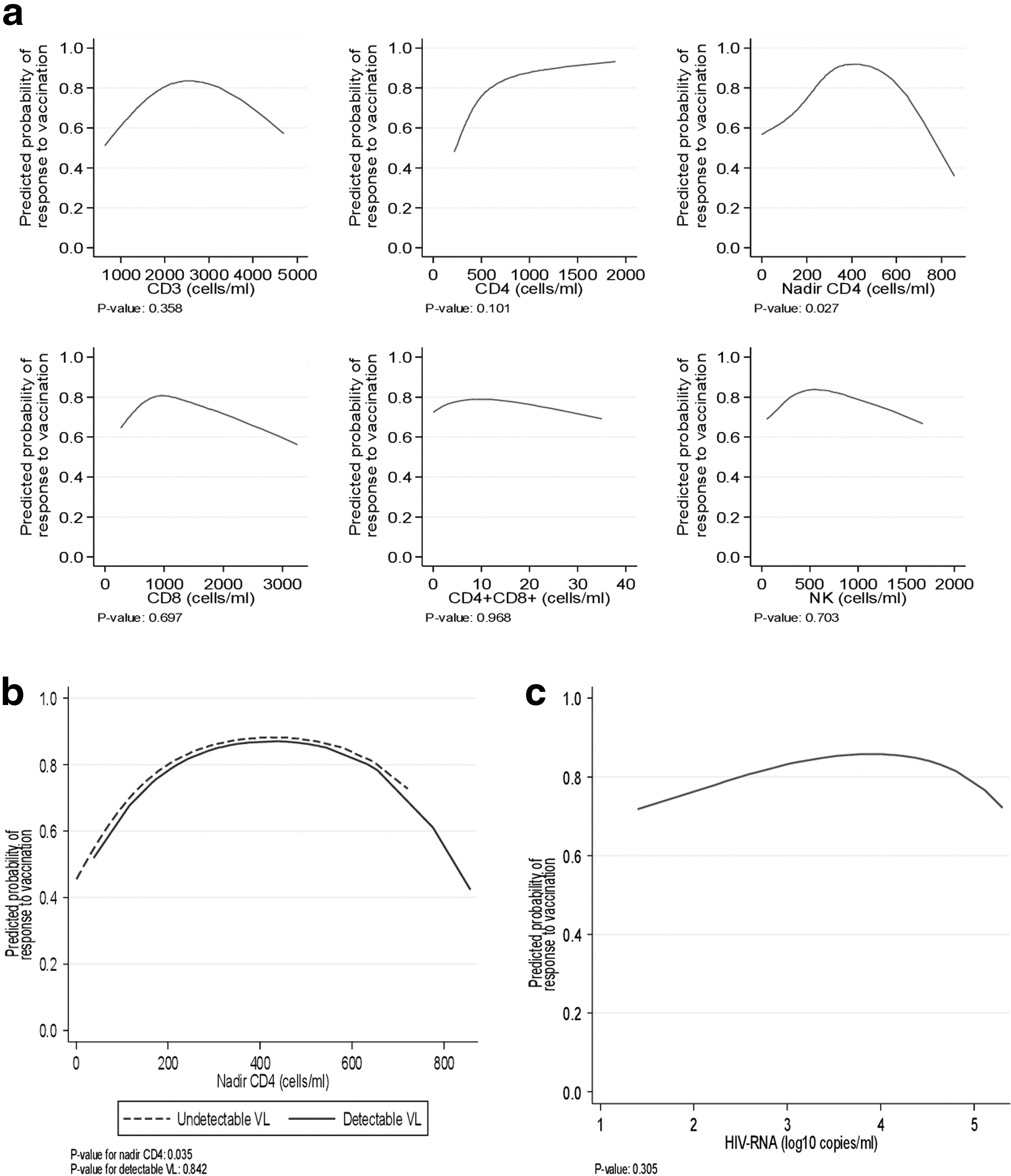
Response to vaccination. Association between predicted probability of response to the hepatitis A vaccine and immunologic parameters
In the univariate analysis, no statistically significant relationship was observed among HIV-RNA and the probability of response (Fig. 1c)
Multiple logistic regression also revealed that the only factor affecting response is the CD4 T-cell count at vaccination. Taking into consideration the viral load, as CD4 count increases by 100 cells/mL, the probability of responding to the vaccine rises by 32% (OR 1.320; 95% CI 1.052–1.656; p=0.016).
No statistically significant interaction was observed between the CD4 count and the viral load in terms of the response to the vaccine (p=0.530).
Using CD4 T-cell count stratification, it was estimated that patients with CD4 T-cell count ≥500 cells/mm3 were 4.3 times more likely to respond to the vaccine than patients with CD4 T-cell count=200–499 cells/mm3, p=0.005).
At the same time, the effect of CD3, CD4, CD8, CD4+CD8+, NK, and nadir CD4 T-cell counts on the response to vaccination, was assessed in terms of the taking of antiretroviral treatment. The p value generated by the Wald test for the respective interaction coefficients was 0.439. Therefore, immunological factors do not affect response differently in HAART-treated versus treatment-naïve patients.
Discussion
A variety of cells are involved in immune response to vaccination. In HIV-infected patients, where many immune cell subpopulations are affected, response to vaccination is expected to be diminished.
In this study, reduced response to the hepatitis A virus vaccine was observed in both treatment-naïve patients as well as in patients receiving HAART, while the single factor affecting response was CD4 T-cells. The other T-cell subpopulations tested had no correlation with response to vaccination.
The hepatitis A vaccine induces an immune response that depends on T cells (T-dependent response). The vaccine components stimulate naïve CD4 T- cells and lead to the manifestation of T-helper 1 (Th1) response. The Th1 response induces both the production of antibodies and the cytotoxic response of CD8 T cells (24).
Furthermore, vaccine antigens stimulate natural immunity. The innate immune system seems to regulate the magnitude and the quality of antibody responses. Emerging evidence points to a key role not only of antigen-presenting cells but also of NK cells (9). NK cells produced following influenza virus vaccination increased gamma interferon (INF-γ), but the distribution of their subgroups remained stable (18).
HIV infection leads to decreased CD4, increased CD8 T-cell count and intense, uncontrolled immune activation resulting in the failure of the immune mechanism (27). Untreated patients exhibit continuous activation and destruction of CD4 T-cells in response to the presence of the virus. At the same time, there is an intense proliferation of CD8 T cells, mainly driven by the levels of HIV RNA. HAART- treated patients develop immune restoration for CD4 T cells, while CD8 T cells decrease but they do not return to normal levels. The decrease of CD8 T-cells is the result of the lowering of immune stimulation following the control of the viral load. Thus, it is compatible with the administration of antiretroviral treatment. The decline of CD8 T-cells during HAART is expected. Elevated CD8 cell counts are thought to be associated with an increased risk of virological treatment failure in HAART-treated patients (14).
Also in patients with HIV-infection, the presence of CD4+CD8+T cells has been recorded. These cells are probably derived from activated CD8 T cells expressing the CD4 molecule (1,4). The dual population of T-cells [CD4+CD8+] has been characterized as memory cells with antiviral activity (20). The CD4+CD8+T-cells appear to be multifunctional cells expressing some CD4 and CD8 T cell markers (10). They are part of the T-cell response to the virus, especially during acute HIV-infection and intense viral replication (6). HAART and suppression of immune activation leads to reduction of large activated T-cells like the double positive, CD4+CD8+T-cells (11). Therefore the decline in the CD8 and in the CD4+CD8+T-cell count does not seem to be associated with the vaccination or have any clinical significance.
In addition, HIV-RNA remained stable post vaccination, indicating that the vaccine does not trigger a major increase of the viral load and it, therefore, does not impair the HIV infection status.
Data from studies that evaluated the potential effect of hepatitis A vaccine in HIV-patients is limited and contradictory. No change in CD4 T-cells or in HIV RNA has been reported, after the administration of the hepatitis A vaccine in adult HIV-patients (17,32). Gouvea et al. (8) have reported a decrease of the CD4 T-lymphocyte count in HIV-infected children, post-vaccination. Other vaccines have also caused a transient drop in CD4 T-cell counts combined with an increase of the viral load in HIV-infected children (19). The study of Pasricha et al. showed that hepatitis B vaccination in HIV-patients significantly increases CD3, CD4, and CD8 T-cell counts, and slightly increases the levels of cytokines associated with the activity of NK-cells (23).
Regarding the response to vaccination, immunosuppressed patients included in this study had an expected low immune response. Although the hepatitis A virus vaccine is highly immunogenic in healthy adults (98%–100%), data from HIV-patients show poor antibody response. The results of relevant studies in HIV-patients vary broadly (response rate 50%–93%) (26). In more recent relevant studies, immune response ranges between 70% and 74%, while in studies using a lower limit to detect anti-HAV antibodies these rates rise to 89% (2,13,17). Impaired response of HIV-patients is also reported with other vaccines, including those against influenza, tetanus pneumococcal infection, and hepatitis B (3,15,28).
In this study, it is of interest that the response rate to the vaccine was similar between treated and untreated patients. Similarly, there was no significant difference in the intensity of the response, as expressed by the anti-HAV geometric mean antibody titer, between the two groups, although there was a clear trend towards higher antibody titers in the HAART-treated group.
Neither HAART nor undetectable viral load seemed to affect response to vaccination. Meanwhile the effect of immunological factors was independent from the use of antiretroviral therapy. Nevertheless, it has been reported that the administration of HAART in children increases the probability of response to the hepatitis A virus vaccine (33). The reconstitution of the immune system seems to be the main responsible mechanism.
In the case of the vaccine against pneumococcal infection, HAART has been directly associated with the long-term durability of antibody response (28). In the relevant article, HAART-naïve patients experienced a steeper decline in protective antibodies. This decline was attributed to the increased loss of memory B-cells in untreated patients, compared to patients under treatment.
Overton et al. (22) concluded that the main factor associated with response to hepatitis A virus vaccination is HIV RNA<1000 cop/mL. Other investigators associate low viral load with the long term maintenance of immune response (2). Similarly, Nielson et al. (21) attribute the successful vaccination of patients with CD4 T-cell count<200 cells/mm3 to the low HIV RNA.
In order to achieve better response, contemporary clinical practice recommends to vaccinate patients with CD4 T-cell counts >200 cells/mm3, unless there are specific reasons. All subjects in this study had baseline CD4 T-cell counts > 200 cells/mm3. So, the absence of the effect of HAART or viral load on response might be due to the fact that study participants were not severely immunosuppressed.
In addition, the almost identical response of treatment—experienced and treatment—naïve patients may be attributed to the similar baseline CD4 T-cell count in both groups. Logistic regression analysis results further confirm this observation, with CD4 T-cells being the single factor associated with response. The probability of responding to the vaccine rises as CD4 count increases. The association of CD4 T-cells with seroresponse is also confirmed by the evaluation of response by stratification of baseline CD4 T-cell count. Patients with a CD4 T-cell count ≥ 500 cells/mm3 had a higher antibody titer, and it was 4 times more likely to respond to the vaccine. Nevertheless, the response rate of these patients (80%) is inferior to the known response of healthy vaccinated individuals (98%–100%).
The results of many relevant studies are similar to ours. Weissman et al. (34), examining patients mostly on HAART, concluded that CD4 count at vaccination is an independent predictor of response to hepatitis A vaccine. The Rimland et al. multifactorial analysis (25) showed that satisfactory immune response was only associated with high CD4 T-cell count and not with viral load or nadir CD4 T-cell count. The same investigators found that patients with CD4 T-cell count<200 cells/mm3 were 16 times more likely to be nonresponders. Similarly, the Hepavac study showed that anti-HAV protective antibodies were observed in 67% of the patients with CD4 T-cell count of=200–350 cells/mm3 and in 83.7% of the patients with CD4 T-cell count of=350–500 cells/mm3 (16).
A similar trend has been reported for hepatitis B virus and influenza virus vaccines (30). During the latest influenza pandemic (H1N1), where, due to the serious morbidity, the vaccine was also given to patients with advanced immunosuppression, reduced immunogenicity was confirmed in vaccinated individuals with CD4 T-cell count<200 cells/mm3 (3). In general, no immune response to vaccination is expected in patients with CD4 count <100 cells/mm3, while patients with CD4 T-cell counts<200 cells/mm3 have a minimum response.
Furthermore, few studies report that nadir CD4 count is a factor associated with response (16). The evaluation of nadir CD4 T-cell count is based on the theory of “immunological scar” even after years of successful treatment. However, in this study, as well as in most of the literature, no correlation between response and nadir CD4 count was established. It seems that the current HIV status is more significant for obtaining immune response.
A limitation of the study is the lack of a control group with healthy adults since the study was performed exclusively in an AIDS Unit. Another limitation lies in the long time interval between the values compared (the initial dose of the vaccine and one month after the completion of vaccination). Any transient changes that may have taken place after the first dose were not identified. We did not examine the immunological parameters following the first dose because we intended to perform an overall evaluation of the vaccination, as given in clinical practice.
Furthermore, we have not evaluated cell functionality, which might efficiently demonstrate the relationship of the hepatitis A vaccine with the immunological system of HIV-patients. Nevertheless, the determination of the T-cell subgroups is used to roughly assess the condition of the defense mechanism, and the clinical evaluation of HIV-patients is based on CD4 and CD8 T-cell counts. Therefore, we think that this study provides useful data reporting quantitative measurement of various immune cells.
In conclusion, although a variety of immune cells plays a role in the antibody response, only CD4 T-cell count is associated with response to the vaccine. Since the hepatitis A virus vaccine does not seem to impair immune system in HIV patients, successful vaccination must form, without any reservation, part of the HIV-patients care. The findings of immune response in patients with CD4 counts >200 cells/mm3 independently of the taking of HAART highlight the need for a new approach to vaccination. As patients with higher CD4 T-cell count are more likely to response to the vaccine, administration of hepatitis A vaccine after HAART initiation and not at the time of initial diagnosis may be the more effective intervention. This study, along with others, could offer data for a new guideline regarding the schedule and timing of HIV-patients immunization.
Footnotes
Author Disclosure Statement
No competing financial interests exist.