
Abstract
In humans, hepatitis B virus (HBV) is the most prevalent and the main infectious agent that leads to liver disease. Previous investigations identified that long-term HBV-infected patients are unable to eradicate HBV completely from hepatocytes. The main mechanisms responsible for long-term forms of the infections are yet to be clarified. However, researchers believe that the differences in genetic and immunological parameters in the patients in comparison to subjects who successfully clear HBV infections may be the causes for long-term infection. Previous studies demonstrated that chemokines play important roles in the regulation of immune cell migration and activation, which is crucial for a comprehensive immune response against HBV. RANTES, MIP-1α, and MIP-1β are important CC chemokines which act through CC chemokines receptor 5 (CCR5). This receptor is expressed on several effector immune cells including NK cells, T lymphocytes, and macrophages, and plays a crucial role in the regulation of activation and migration of the immune cells during immune responses against viruses, including HBV. Therefore, alterations in its expression or functions could be associated with attenuated immune responses against HBV. In addition, previous studies identified that a 32 base pair deletion (Δ32) in exon 1, as well as three polymorphisms in the promoter region of the CCR5 gene results in downregulation of the molecule. Previous studies revealed that CCR5 expression was altered in hepatitis B but the role of the CCR5 Δ32 mutation and CCR5 promoter polymorphisms in this disease is controversial. This review addresses the recent information regarding the status of CCR5 expression on immune cells and the association of CCR5 promoter polymorphisms with HBV-infected patients.
Introduction
I
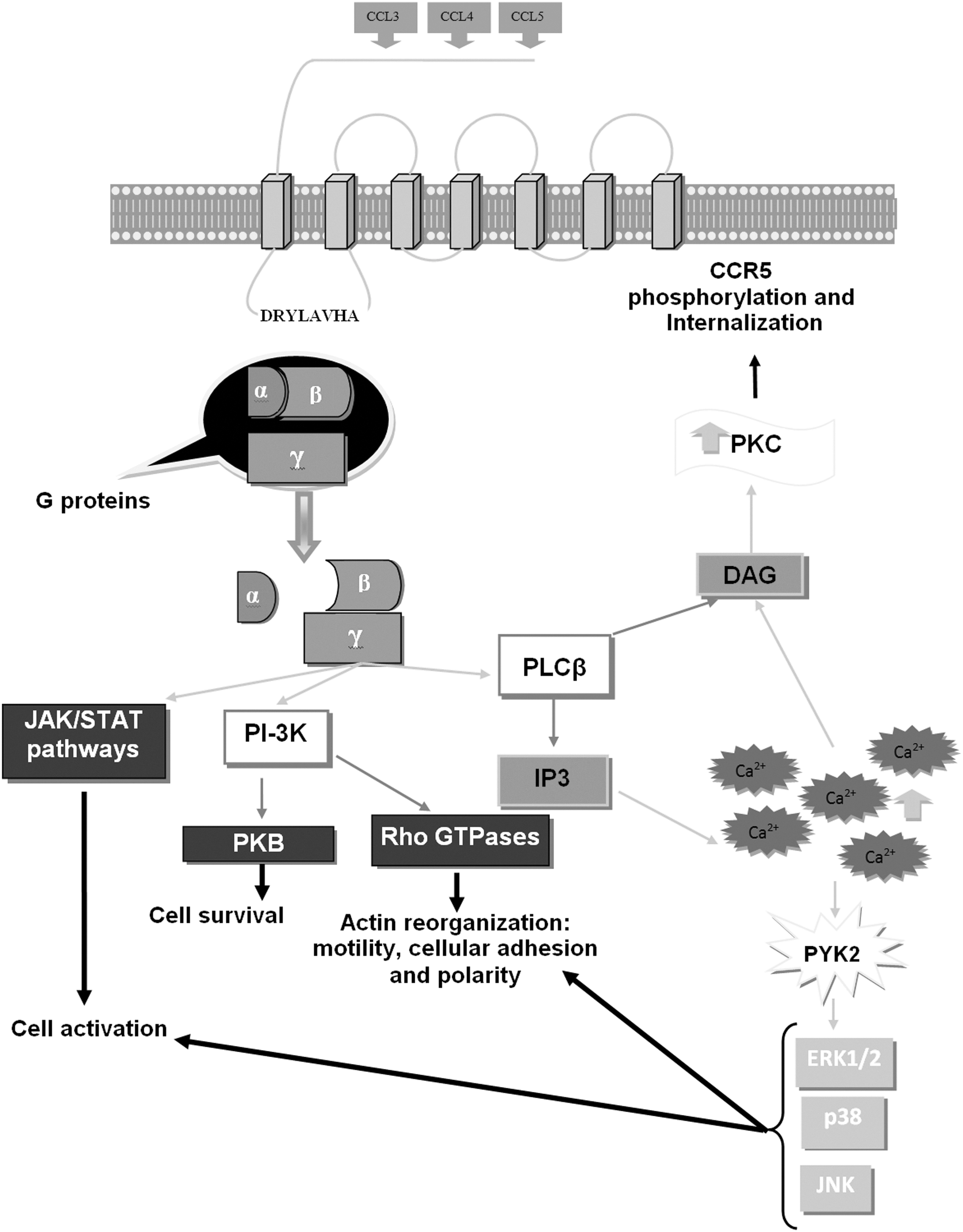
The CCR5 receptor structure and its signaling pathways. CCR5 is shown as a 7 transmembrane domain receptor that interacts with CCL3, 4, and 5 on the extracellular domain and lead to the activation of intracellular pathways. The conserved DRYLAVHA amino acids sequences within the first intracellular loop play crucial roles in activation of G proteins (α, β, and γ). Subsequently, the CCR5/ligand interaction leads to G protein dissociation and consequently the induction of intracellular pathways including phospholipase Cβ (PLCβ), JAK/STATs, phosphoinositide 3-kinase (PI-3K), triphosphoinositol (IP3), diacylglycerol (DAG), elevation of intracellular calcium ions (Ca2+), protein kinase C (PKC), proline-rich tyrosine kinase 2 (PYK2), extracellular signal-regulated kinase (ERK1/2), p38, c-Jun N-terminal kinase (JNK), protein kinase B (PKB), and Rho GTPase. Adapted from Sorce et al., (39).
CCR5 and Viral Infection
Previous investigations demonstrated that CCR5 plays important roles in viral infections. For instance, it has been documented that CCR5 is a co-receptor for human immunodeficiency virus (HIV) and facilitates HIV entrance into CD4-positive T lymphocytes (27). Additionally, studies confirmed that absence or downregulation of CCR5 led to reduction in the disease progression (19). The CCR5 Δ32 mutation also has a negative correlation with acquired immunodeficiency syndrome (AIDS) development (36). Therefore, it appears that CCR5 plays key roles in the development of AIDS in HIV-infected patients. In contrast to HIV infection, CCR5 has protective roles against other viruses including influenza (17,23), cytomegalovirus (46), herpes simplex virus type (HSV) (11), and hepatitis C virus (HCV) (15). Therefore, it can be concluded that CCR5 regulates the induction of immune responses against viral infections. Thus the recent data regarding the correlation between CCR5 expression, as well as its genetic variation in hepatitis B, are discussed in this review article.
CCR5 Expression on Immune Cells of HBV-Infected Patients
It has been well documented that parameters that de-regulate appropriate immune responses can be associated with the outcome of viral infections, especially hepatitis B (5). Previous studies identified that CCR5 ligands (CCL3, 4, and 5) are produced by immune and non-immune cells in response to HBV antigens (34,49). Additionally, it has been shown that CD4-positive T cells have increased expression of CCR5 in acute hepatitis B when compared to the chronic form (45). Therefore, it seems that the expression of CCR5, which is the main receptor for CCL3, CCL4, and CCL5, is altered during hepatitis B infection and may affect its clearance by a patient. As previously mentioned, NK and NKT cells represent the main immune cells against HBV (22), hence, the status of CCR5 expression on these cells influences immune responses during hepatitis B infection. Previous studies demonstrated that NKT cells expressed higher CCR5 receptor than conventional T cells (22), so it appears that alterations of CCR5 expression can affect these cells more than T lymphocytes. Our previous study showed that CCR5 expression was decreased on the NK cells of occult hepatitis B-infected (OBI) patients (7).
Furthermore, our unpublished data revealed that NK cells of chronic HBV-infected (CHI) patients express lower CCR5 than healthy controls that had cleared an HBV infection. To the best of our knowledge, our previous studies were the first studies that evaluated CCR5 expression on the NK cells of HBV-infected patients. Based on these studies, it seems that decreased CCR5 expression on NK cells is associated with the long-term types of HBV infection (chronic and occult form). Interestingly, it has also been documented that HBcAg-specific CD8 T cells have high levels of CCR5 expression (37), hence it seems that CD8 T cells may perform their functions in a CCR5-dependent manner. Recent information regarding the role of CCR5 in the activation of T cytotoxic cells against HBV is controversial. Accordingly, our previous study demonstrated CCR5 is downregulated on the cytotoxic T cells of OBI patients (8). Our study on CHI patients also revealed that cytotoxic T cells have lower expression of CCR5 when compared to healthy controls (2). In contrast with these studies, Lee et al., reported that the expression of CCR5 on the CD8+ T cells of CHI patients was not changed when compared with those of healthy controls (28). These studies suggest that CCR5 is a key regulator of immune responses to HBV and its expression in immune cells appears to be deficient in HBV-infected patients. However, the findings are not definitive, and expression studies need to be completed on the various immune cells, as well as in conjunction with studies in several ethnic groups.
CCR5 Polymorphisms in Hepatitis B
Due to the important roles played by CCR5 in hepatitis B, several researchers have evaluated the relation between variations in the CCR5 gene and hepatitis B that are discussed here. Previous studies have focused on the variations identified in the promoter region (-59029, -59353, and -2459) of the CCR5 gene and also on the CCR5 Δ32 mutation. For example, Ahn et al. reported that the polymorphisms at -59029 were significantly associated with CHI (3). Chang and colleagues also revealed that the polymorphisms at -59029 of the CCR5 gene were associated with hepatitis B (12). They have also demonstrated that the -59029A allele was significantly associated with the increased risks of CHI (12). Another study from China demonstrated that the CCR5 -59029 polymorphism is significantly associated with susceptibility to HBV infection (35). Thus, based on these results, it can be concluded that the CCR5 -59029 polymorphism can be considered as a risk factor for prolonged forms of hepatitis B.
Additionally, it appears that the polymorphisms at -59353 of the CCR5 gene also can be considered as a risk factor for prolonged hepatitis B. For instance, Ahn and colleagues revealed that there is a significant association between the polymorphisms at -59353 with CHI (3). Currently there is no additional information regarding the relation between this polymorphism and hepatitis B, and more studies are required to develop our knowledge regarding this polymorphism.
In contrast with the -59029 and -59353 polymorphisms, studies on the -2459 polymorphism reveal conflicting results. For example, Cheong et al. showed that the CCR5 -2459 polymorphism was significantly associated with CHI in 957 Korean patients (13), while Jae and colleagues reported that the polymorphism at -2459 of CCR5 was not associated with HBV persistence in another Korean population (21). Another study identified that CCR5 -2459 mutation was not associated with post-transplant re-infection with HBV in a Chinese population (29). Therefore, it appears that the polymorphism at the -2459 position of the CCR5 gene is not associated with CHI in some populations, and more studies on this polymorphism are required to improve our knowledge regarding the relation between CCR5 -2459 polymorphism and prolonged term hepatitis B.
Interestingly, the studies on the CCR5 Δ32 mutation showed more discrepancies. Ahn et al. demonstrated that the CCR5 Δ32 mutation were significantly associated with CHI (3), while other researchers reported that the CCR5 Δ32 mutation was not associated with hepatitis B (12). Our previous findings also revealed that the CCR5 Δ32 mutation was associated with neither OBI (8) nor CHI (24) patients. Ganczak and colleagues also reported that the CCR5 Δ32 mutation was not prevalent in CHI patients (18). Li and colleagues identified that the CCR5 Δ32 mutation was also not associated with post-transplantation re-infection with HBV (29). Tan et al. (42) and Liu et al. (30) also reported that CCR5 Δ32 mutation was not found in any evaluated Chinese HBV-infected patients. These results are in contrast with Suneetha et al., who demonstrated an association between the CCR5 Δ32 mutation and hepatitis B (41). Accordingly, the authors revealed that the frequency of heterozygosity of the CCR5 Δ32 mutation was more prevalent in CHI patients than controls (41). Thio and colleagues also reported that the CCR5 Δ32 mutation reduced the risk of progression to a persistent form of HBV infection (43). Another study identified that the CCR5 Δ32 mutation increases the likelihood of HBV eradication from the infected liver (44). The discrepancy in the studies may reflect the differences in the evaluated populations in terms of genetic background, as well as epigenetic factors. According to the studies surveyed here, it seems that the polymorphisms within the promoter at -59029 and -59353 are significantly associated with outcome of hepatitis B, but the association between both the CCR5 -2459 polymorphism and the CCR5 Δ32 mutation with hepatitis B remains controversial.
Conclusion
Based on the available data, it appears that CCR5 plays an important role in responding to hepatitis B, because its expression is disrupted on the NK cells, as well as cytotoxic T cells of long-term HBV infected patients. Additionally, due to the fact that the number of CCR5-positive NK cells and the intensity of CCR5 on NK cells of prolonged HBV-infected patients are decreased during hepatitis B (7), it is possible that the CCR5 -59029 and -59353 polymorphisms may play important roles in regulation of CCR5 expression.
Furthermore, the association between both the CCR5 -59029 and -59353 polymorphisms with prolonged hepatitis B infection is supported by its strong linkage disequilibrium (12). Both of these polymorphisms are associated with hepatitis B simultaneously. Once again, based on the available data, it appears that CCR5 is genetically associated with prolonged hepatitis B infection.
The discrepancies between the reported studies regarding the relationship between the CCR5 Δ32 mutation and the CCR5 -2459 polymorphism with hepatitis B may be due to differences in the studied populations that originated from varying ethnic groups with different genetic backgrounds. Previous studies revealed that a consequence of CCR5 downregulation is the increased expression levels of CCL3, 4, and 5 (32). Due to the fact that CCL3, 4, and 5 can use other receptors, such as CCR1 and CCR3, it is plausible that upregulation of these chemokines may lead to immune cell activation and migration of these cells to the HBV-infected liver, which subsequently improves viral clearance. Therefore, it appears that investigating the expression of CCL3, 4, and 5, as well as CCR1 and CCR3, could be considered for future studies in hepatitis B. Finally, based on the fact that chemokines and their receptors are components of a complex regulatory network, it will be important to study the expression levels of chemokine receptors and their ligands, as well as the presence of polymorphisms within the regulatory regions of these genes.
Footnotes
Acknowledgments
This project was supported by a grant from the Rafsanjan University of Medical Sciences.
Author Disclosure Statement
No competing financial interests exist.