
Abstract
According to pathogenic surveillance data during the first half of 2012, the H3N2 influenza virus was prevalent in Guangdong, China, but no pandemic H1N1 (pH1N1) virus was detected. This study aimed to measure the seroprevalence of pH1N1 and H3N2 infection following the influenza epidemic in 2012. We collected serum samples by stratified random sampling in a cross-sectional survey from August, 2012 to October, 2012. Antibody titers against H3N2, pH1N1, and influenza B antigens were measured by the hemagglutination inhibition (HI) assay, and age-specific seroprevalence and non-immunity were calculated. A total of 566 serum samples were collected from subjects who had not received an influenza vaccination. The seroprevalence of H3N2, pH1N1, and influenza B were 61.7%, 31.3%, and 40.4%, respectively, while non-immunity was calculated to be 9.2%, 40.6%, and 27.0%, respectively. The highest recorded seroprevalence was 86.0% for H3N2 in the 6–15 year age group, while the lowest was 14.6% for pH1N1 in the 60+ age group. Non-immunity fractions were 44.4% and 53.5% in the 0–6 and 60+ age groups, respectively. In conclusion, the seroprevalence of pH1N1 remained below 50% in all age groups following the 2012 influenza season. These data suggest that vaccination against pH1N1 antigens should be conducted, especially in the older age groups, before the next influenza season.
Introduction
S
After the pH1N1 wave in 2009–2010 in New Zealand, the overall community seroprevalence of pH1N1 was 26.7% and it varied across age groups (1). The highest seroprevalence (46.7%) was in children aged 5–19 years with a significant increase from the baseline (14%), while older adults (≥60 years) showed no significant differences in seroprevalence between the seroprevalence (24.8%) and baseline (22.6%). A cross-sectional study (17) conducted in Guangdong, China, reported a total seroprevalence of 22.8% (985/4319), with the highest seroprevalence found in the 11–20-year-old age group (32.8%), while the seroprevalence in those greater than 60 years of age was only 12.6%. The antibody titers against pH1N1 were the highest in the 7–17-year-old age group, followed by a gradual decrease in adults, then a significant increase in the elderly groups from urban areas.
Usually, influenza activity infections peak annually from March to July in Southern China (7). According to the Center for Public Health Surveillance and Information Service of China (3), the influenza case number was 2.35 times (74151/31551) during January–June in 2012 than that of last year. 87.3% (365/418) isolates were H3N2 subtype viruses, which were isolated from local epidemics and sporadic cases in Guangdong during March–June, 2012. No pH1N1 virus was detected by the Guangdong Influenza Surveillance Networks (only one in December of 2012), which suggests that the influenza H3N2 virus was the most prevalent strain (18) and that influenza B viruses were also often isolated. We conducted a cross-sectional study in order to track and determine the immune status of the population of Guangzhou, China, against influenza pH1N1, and to measure the seroprevalence of influenza H3N2 following the H3N2 epidemic in 2012.
Materials and Methods
Ethics statement
Subjects provided written consent. The concept and design of the study was approved by the Guangdong Provincial Center for Disease Control and Prevention Ethics Committee, as well as that in a previous study (17).
Serological sample and data
Serum samples were obtained from the subjects in Guangzhou, the capital of Guangdong Province, during August–October 2012. All sera were assembled into the following age groups: 0–5, 6–15, 16–25, 26–60, and >60 years of age, with at least sera 80 subjects per group. Multi-stage stratified random sampling was introduced in each age group (17). For each sample, the data of collection, age, gender, and vaccination status of the subject were recorded.
Antigen preparation
The strains isolated during the 2010–2012 epidemic/pandemic were selected as antigens against the serum antibodies. Referred to vaccine strains recommended from the World Health Organization (WHO) (4), the three strains used were A/Guangdong/1154/2012 (H3N2, A/Perth/16/2009-like), A/Guangdong/50/2011 (pH1N1, A/California/7/2009-like), and B/Guangdong/178/2010 (Bv, B/Brisbane/ 60/2008-like) with β-propiolactone (BPL) inactivation.
Hemagglutination inhibition (HI) assay
HI assays were performed with inactivated virus according to the World Health Organization Manual on Animal Influenza Diagnosis and Surveillance (15).
Statistical analysis
Data were analyzed using SPSS v16.0 (SPSS Inc., Chicago, IL); all sera were divided into five age groups or eight age groups dependent on the seroprevalence tendency based on age. Seroprevalence was primarily defined as the serum titers ≥40 by HI assay; HI titers <10 was were serologically considered as having non-immunity against the specific influenza subtype/type (13,17). Geometric mean titer (GMT) was calculated for each age group, with a titer less than 1:10 assigned a value of 5. In analyses where some individuals contributed more than one observation, robust standard errors were used to construct 95% confidence intervals (CIs). Categorical variables were analyzed using the Chi-square test or Fisher exact test. The independent sample t test was used to compare GMTs of HI antibodies. Statistical testing was performed with the level of significance set at p<0.05.
Results
Antibody responses by gender and age groups
A total of 566 serum samples had been collected from subjects (male:female=1.28:1) without vaccination against influenza. The seroprevalence of H3N2 was 61.7% (349/566), whereas the seroprevalence of pH1N1 and influenza B were 31.3% (177/566) and 40.4% (229/566), respectively. There were no statistically significant differences in seroprevalence of subtypes/types between genders (Table 1).
Pearson Chi-Square (two- sided).
According to collective sera, the highest seroprevalence was observed in subjects in the 6–15 age group for H3N2, and the lowest in 60+ age group was for pH1N1. The age groups that showed seroprevalences <50% included the 60+ age group for the H3N2 subtype, all age groups for the pH1N1 subtype (except the 6–15 age group) and all age groups for influenza B (except the 16–25 age group). There were statistically significant differences between the seroprevalences among the five age groups across three subtypes/types (Table 1).
Antibody responses by age group
Influenza antibody responses were summarized by age groups in detail (Table 2).
The lowest antibody response rate was 38.9% against H3N2 in the two older age groups (26–60 and 60+), which was lower than 50% of the observed seroprevalence values. For antibody responses to pH1N1, seroprevalences lower than 50% included all eight age groups, with the lowest fraction being 10.1% (ages 61–70), whereas antibody responses against influenza B showed seroprevalence values less than 50% in seven age groups except that of one (ages 21–30, 53.5%).
The GMTs were calculated to be 19.4% (95% CI, 15.1–24.9%) – 68.1% (95% CI, 54.1–85.7%) for H3N2, 9.0% (95% CI, 7.5–10.7%) – 25.9% (95% CI, 20.0–33.6%) for pH1N1, and 14.5% (95% CI, 11.2– 18.7%) – 29.2% (95% CI, 23.4 –34.3%) for influenza B. The GMT in the 0–10 age group was 3.51 times that in the age 71+ age group. The differences in seroprevalence were statistically significant between eight age groups in three subtypes/types (Table 2).
The seroprevalence in of H3N2 gradually declined as age increased (Fig. 1). The seroprevalence of pH1N1 increased in the 11–20 age group, then gradually declined as age increased. The seroprevalence of influenza B type increased in the 21–30 age group, then gradually declined, but fluctuated as age increased.
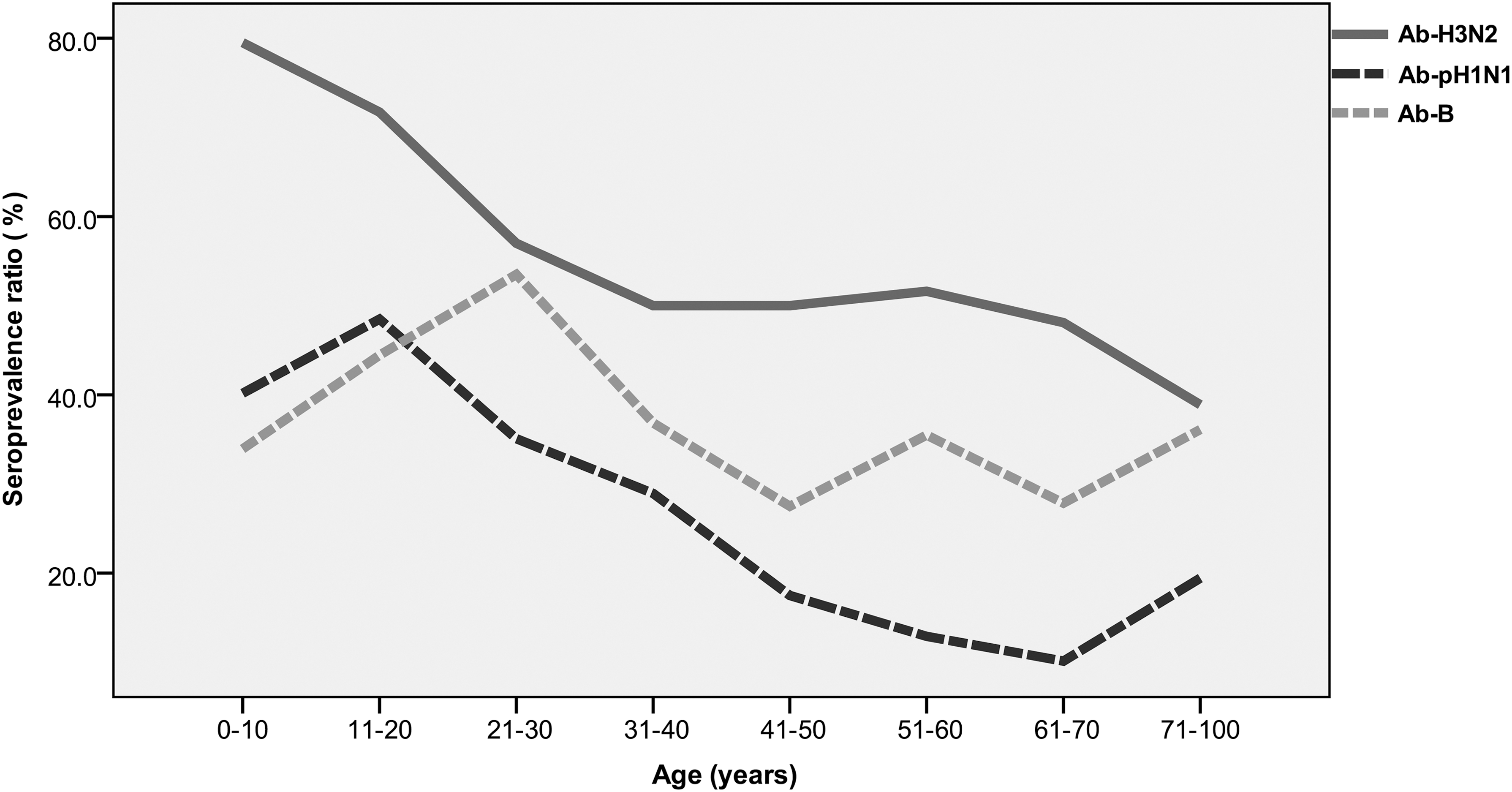
Seroprevalence of three influenza viruses in 2012.
Non–immunity by age groups
The fraction of subjects that were not immunized to the three subtypes/types of influenza were 9.2% (52/566), 40.6% (230/566), and 27.0% (153/566) for H3N2, pH1N1, and influenza B, respectively (Fig. 2). The preschooler 0–6 age group (44.4%) and older age ≥60 age group (53.5%) had higher non-immunity rates in for pH1N1 among the five age groups. In summary, human immunity against H3N2 infection maintained a higher, and that against pH1N1 infection only had a lower level.
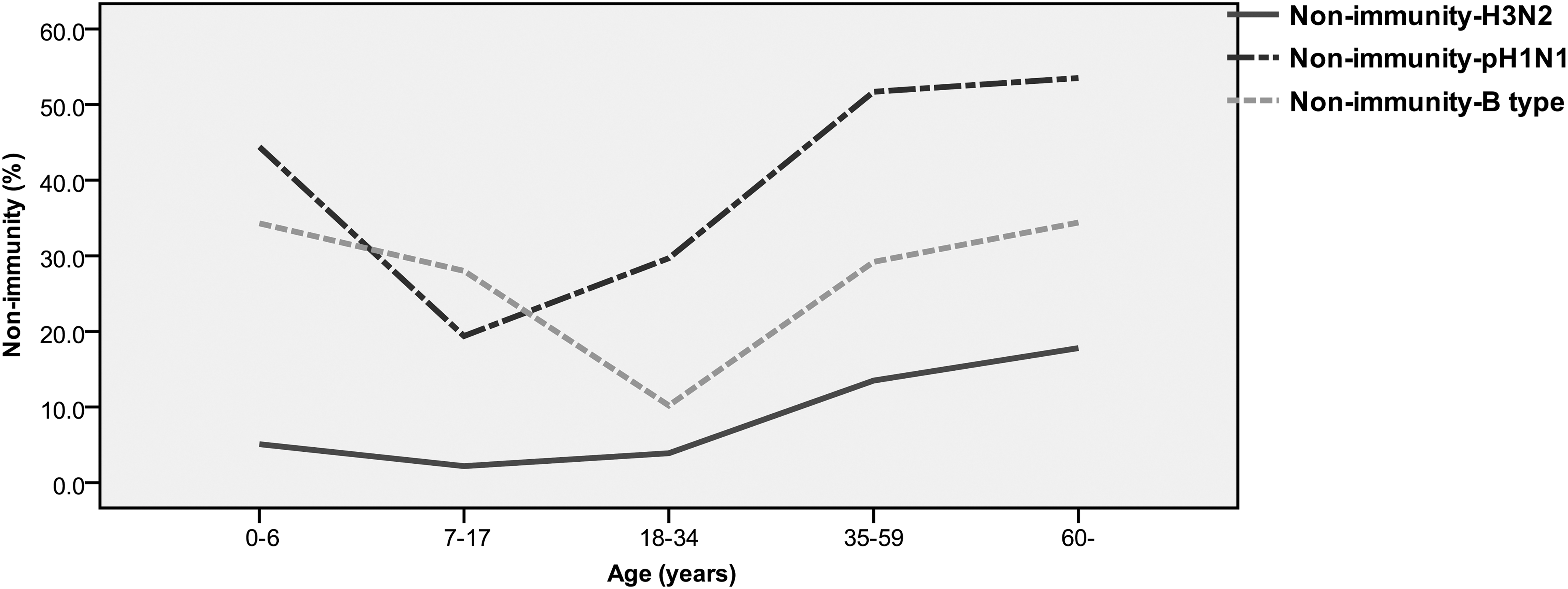
Age-dependent prevalence of non-immunity to three influenza viruses.
Multiple antibodies in each subject
The percentages that the sample antibodies were positive response (≥1:40) against two and all of three H3N2, pH1N1, and influenza B antigens were 8.3% (47/566) in antibodies only against H3N2 and pH1N1, 13.3% (75/566) in antibodies only against H3N2, and influence B, 5.8% (33/566) in antibodies only against pH1N1 and influenza B, and 15.2% (86/566) in antibodies against all of three H3N2, pH1N1, and influenza B antigens (Table 3). With this correspondence, the percentage that the antibodies were negative response (<1:40) against H3N2, pH1N1, and influenza B antigens were up to 23.0% (130/566), where the highest negative ratio was 36.9% (58/157) in the 60-year-old group.
Negative ratio was defined as the serum titers <40 by HI assay.
Discussion
Influenza viruses cause recurrent illnesses, annual epidemics, and extended pandemics that spread quickly and affect entire populations (10). According to virological surveillance in the United States (5), the proportion of influenza H3N2, pH1N1, and influenza B viruses isolated during October 2, 201100May 19, 2012 were 60.8% (11002/18100), 21.9% (3966/18100), and 17.3% (3132/18100), respectively. In Guangdong, China, during the first half of 2012, 87.3% (365/418) of surveyed viruses were of H3N2 subtype viruses and the rest were influenza B type viruses (Victoria lineage) (3). Furthermore, the higher seroprevalences among the youngest age groups might be associated with H3N2 infection from the H3N2 epidemic in Guangdong (6,18).
Influenza pH1N1 epidemics in Guangdong prevailed during 2009–2011 and surprisingly, no epidemics/cases emerged during the first half of 2012. Several studies on pH1N1 serology have been conducted in the past 3 years (1,11,17); however, the seroprevalence for the year 2012 is underreported. The seroprevalence among different age groups ranged from 12.6% to 29.3%, as reported by the 2010 Guangdong serosurvey (17). In contrast to previous results, the findings presented here can be summarized as follows: i) the GMTs for pH1N1 in this study remained low, for example, seroprevalences in the age 41+ age group was only was 10.1% to 19.4% in pH1N1; ii) the GMTs for pH1N1 in the age above 6+ age groups were higher (14.6–51.6%) than the former among the 6–15, 16–25, 26–59, and 60+ age groups. The seroprevalence of influenza B was similar to that of pH1N1, where the seroprevalences in the 41–50 and 61–70 age groups was as low 27.5% to 27.8%.
As the serum was pre-treated by RDE (15), the low HI titer could be explained by the associateion with specific antigens from previous influenza infections or vaccinations. Usually, seroprevalence (serum titers ≥40) is used to evaluate the effective immunity against influenza, but even one individual with low HI titers (including between 10 and 20 titers) had a less severe disease progression (16). In this study, we have defined HI titers <10 as having no immunity against influenza infection. Both young and old age groups with the low seroprevalence/non-immunity against pH1N1 virus were susceptible to pH1N1 infection. The high seroprevalence of pH1N1 in the 11–20 age group and the lack of immunity against pH1N1 in the 7–17 age group are contrasted in Figures 1 and 2. The differences between seroprevalence and non–immunity depends on the number of moderate titers (between 10 and 20 titers).
Seroprevalence of Abs decreases according to the increase of the age, and the highest rate of non-immunity seems to exist for pH1N1 in the elderly. Considering that pH1N1 did not widely circulate in the previous year, it could be interpreted due to the low relatedness of recent flu circulating strains that elderly people likely came in contact with pH1N1 1 year ago. The peak HI titer observed in the oldest age seems to be related to a previous immunity to pH1N1-like H protein, although no inoculation of pH1N1 vaccine was recorded.
The aged individuals with lower antibody responses against influenza viruses due to their humoral immunity responses were only against conserved epitopes from influenza viruses or vaccines. Although the fatality rate for pH1N1 was lower than that of human H5N1, many severe/fatal pH1N1 cases emerged in America, Asia, Europe, and Africa during from 2009 to 2012 (14). The risk factors for pH1N1 infection were similar to those for seasonal influenza, especially in younger age groups (14). The results of this study suggest that influenza vaccination in older age groups (seroprevalence with of 10.1–19.4% and a non-immunity rate of 53.5% and negative ratio of 36.9%) might be necessary to prevent the influenza infection. The presence of pre-existing antibody at a titer ≥40 prior to vaccination affected the antibody response to influenza vaccination (8). Achieving high vaccination rates in the senior population is recommended as a goal, considering the benefits of influenza vaccination in the elderly (2). Furthermore, an increase in vaccination might reduce morbidity and prevent further complications from influenza, while providing more effective herd immunity, and rationalizing costs to the public health system (12).
Footnotes
Acknowledgments
This work was financially supported by the National Transfer Payment funding for the 2012 influenza survey and the National Natural Science Foundation of China (Grants no. 30972757). We thank Dr. Jie Wu and Lirong Zou for their assistance.
Author Disclosure Statement
No competing financial interests exist.