
Abstract
The most useful treatment for HCV infection worldwide is peg-interferon plus ribavirin, although the response varies from person to person. Hence, host genetics are significantly involved in the treatment response to HCV infection. The 2′-5′ oligoadenylate synthetase (OAS) is one of the most important components of the immune system having significant antiviral functions. The aim of this study was to investigate the role of single nucleotide polymorphism (SNP) at the exon 7 splice acceptor site (SAS) of OAS1 to interferon-based therapy of HCV infection. OAS1 genotyping was performed in 140 HCV patients by restriction fragment length polymorphism polymerase chain reaction method (RFLP-PCR). These patients were enrolled for the study in 2010–2013. OAS1 SNP was also established in 120 healthy controls. Correlation of HCV genotypes, OAS1 SNP, and other factors with response to interferon therapy were statistically analyzed by SPSS 13 software. There were no significant differences in the distribution of OAS1 genotypes between healthy and patients subjects. The distribution of AG and AA genotypes of OAS1 genotypes between sustained virological responders (SVRs) and the non-responders (NRs) group were also comparable. However, Pearson chi square analysis indicated that the patients possessing a GG genotype of the OAS1 gene at exon 7 SAS demonstrated significantly positive association with treatment response to HCV infection (p=0.039). This study determined that SNP at exon 7 SAS of OAS1 was significantly associated with response to interferon-based therapy of HCV infection in our population.
Introduction
H
The current standard treatment for chronic HCV genotype 3 (HCVG3) infections is pegylated alpha interferon (IFN) with weight-based ribavirin, which is given for 24–48 weeks (37). Increasing data support evidence that serological and clinical factors may predict a long-term response to interferon-based therapy of HCV infection. These features involve both viral and host factors (10,18,23,28,40,41,45). Among the viral factors, genotypes and HCV RNA levels are significantly associated with the treatment response, while among the host factors, disease duration, patient age, stage of liver fibrosis, and other genetic factors can adversely influence the treatment response (8,11,40). The host genetic factors have an imperative role in the building of a unique immune response by controlling differences among individuals in the stimulation of cytokines or other intracellular antiviral proteins (3,13). One of the most important reasons for these differences among individuals in cytokines production is attributed to single nucleotide polymorphisms (SNPs) in the human genome. SNPs also have a significant role in the development of chronic HCV infection and response to combinational therapy of HCV infection (35,39).
Recently, genome wide association studies (GWAS) of more than 1600 patients revealed a strong association of IL28B polymorphism at rs12979860 with pegylated interferon and ribavirin treatment. It was shown that patients with a CC genotype at this particular position have a 2.5 times or even better response to interferon-based therapy. This association was also confirmed in other ethnic groups worldwide. Additionally, the C allele was also more prevalent in healthy subjects as compared to chronically infected subjects in multi-ethnic populations, pointing its potential role in natural clearance of HCV infection (38).
IFN therapy stimulates several intracellular antiviral proteins. The OAS1 is one of the most important intracellular antiviral proteins that are stimulated by IFN therapy (21,23). The OAS1 is an IFN-stimulated enzyme that converts ATP into 2′–5′ linked oligomers of adenosine in the presence of double-stranded (ds) RNA (31). Latent ribonuclease L (RNaseL) is activated by 2′–5′ linked oligoadenylate to degrade viral RNA and inhibit protein synthesis. Thus, 2′–5′ OAS protein has discriminating activity against several viruses.
The 2′–5′ OAS gene family is comprised of OAS1, OAS2, and OAS3 as important members. The OAS1 gene is placed on human chromosome 12q24.2 encoding four isoforms p42, p44, p46, and p48 (17). Many recent studies have demonstrated a significant role of 2′-5′ OAS-RNaseL system for clearing viral infections (22,24,30). In HCV infection, the core protein has been shown to activate the 40/46-kDa OAS1 gene promoter specifically in various human hepatocyte-derived cell lines. The promoter induction of OAS1 gene was further enhanced in the cells treated with interferon alpha (27). Thus, any SNP with an effect on OAS1 activity may also have a role in determination of resistance/susceptibility to HCV infection and also interferon-based therapy of HCV infection.
Although the OAS1 gene has a very important contribution in antiviral interactions, there are many variations in its sequence. Approximately 36 SNPs have been noted in this gene. The strongest SNP that is associated with OAS1 activity is found at exon 7 SAS. This SNP (rs 10774671) is also suggested to influence susceptibility to type 1 diabetes (5). The normal splicing at exon 7 of OAS1 gene is achieved by the presence of AG sequence at this position. The G allele at this position retains the splice site and confers higher enzymatic activity (p46), whereas the presence of A allele at this position (AA at acceptor site) ablates the splice site and confers lower enzymatic activity (p48 and p52) to the OAS1 gene (4,20). Thus, the genetic variation at exon 7 SAS of OAS1 makes it an excellent candidate gene that can significantly predict the response to IFN-based therapy in HCV or HBV patients (20,36).
During the last decade, there is a continuous struggle for discovering new treatment options of HCV infection, since interferon therapy is long, expensive, and associated with severe side effects. Different approaches for searching new treatment options of HCV infection involve small organic compounds, siRNA, shRNA, peptide methods, and targeting various host factors that have important role in HCV life cycle. Recently, two NS3 protease inhibitors, Telaprevir and Boceprevir, have been added to peg-interferon plus ribavirin treatment of HCV genotype 1 (19). Many direct acting agents such as TMC-435, BI 201335, ABT-333, and Debio 025 are in stage III of clinical development (16). How these small genetic variations would affect therapy will require further research.
Materials and Methods
Subjects
The blood samples of chronic HCV patients were collected from the Gambat Institute of Medical Sciences (Province; Sindh) and Saidu Group of Teaching Hospital (Province; Khyber Pakhtun Khwa). Initially, 186 chronic HCV patients were enrolled in the study. Patients received IFN+ribavirin treatment for 6 months, except HCV genotype 1 and 4 patients who received the combinational therapy for 6 more months. Subjects who discontinued treatment due to any reason were excluded from the study. Finally, 140 chronic HCV infected patients remained. One hundred and twenty healthy controls (negative for HCV Ab and RNA as well as hepatitis B surface antigen) were also involved in the study. The institutional Ethics Committee gave permission for the study. The consent of both the patients and healthy subjects were taken for the genetic testing of OAS1 gene prior to enrollment in the study. The patients were monitored for 6 months after the end of therapy and were grouped into SVR and IFN non-responder (NR-IFN) on the basis of treatment response. All patients who tested negative for HCV RNA (using both nested RT-PCR and real-time PCR) after 6 months of treatment completion were grouped into SVR, while those patients who did not show SVR were grouped in NR.
Determination of OAS1 gene polymorphism
The blood samples of all healthy controls and HCV-infected subjects going through IFN-based therapy were collected in EDTA tubes. DNA extraction was performed by using a Genomic DNA mini kit (Invitrogen; Cat no. 1820-02) according to manufacturer's instruction, followed by its quantification with Nanodrop (Eppendorf Biophotometer, Germany). RFLP-PCR was used for genotyping of OAS1 gene. The technique is widely used for mutation detection worldwide (2,43). We used reported primers to amplify 203 bp PCR fragments of OAS1 gene. Primer sequences used were as follows: rs10774671; forward, 5′-TGCAATGCAGGAAGACTCC-3′ and reverse, 5′-TGCAGGTCCAGTCCTCTTCT-3′ (9). This product also covers our desired SNP. PCR amplification was carried out in 25 μL mixture containing 100–500 ng DNA, 2.5 mM MgCl2 (Fermentas), 10 pM of each primer, 2x PCR buffer (Fermentas), 200 mM dNTP's (Fermentas), and 2 units of Taq DNA polymerase (Fermentas). Cycling condition involved long denaturation at 95°C for 5 min, followed by 35 cycles, each at 94°C for 30 sec; annealing at 62°C for 30 sec; and extension at 72°C for 1 min. Cycling condition was followed by a final extension step at 72°C for 10 min.
The restriction enzyme, AluI (Fermentas), was used for the digestion of amplified product. 8 μL of the PCR product was digested by 5 units of AluI enzyme in a total volume of 20 μL. The incubation period was for 4 h at 37°C. 10 μL of the digested product was run on a 3% agarose gel stained with ethidium bromide. The electrophoresed product was observed under UV light of Wealtec gell doc system. HCV genotyping was performed according to Ohno (29). The protocol is already optimized protocol in our laboratory (32).
Statistical analysis
Hardy-Weinberg equilibrium was applied to determine the distribution of OAS1 genotypes in both patients and healthy controls. Statistical analysis between the SVR and NR groups were determined by SPSS 13. Pearson Chi square test was applied on treatment responders and non-responders to determine association between treatment response and OAS1 genotypes. A two-tailed p value≤0.05 was considered to be statistically significant.
Results
Patients and healthy subjects
All the patients and controls were descendents of Pakistani origin. Groups of SVR and NR chronic HCV patient groups were compared to reveal any of the clinical, pathological, biochemical, or virological parameters associated with specific patterns of treatment response. Data were analyzed as mean±SD. The univariate analysis of clinical and virological factors was compared between SVR and NR; no significant differences were revealed between the two groups (Table 1).
Analysis of OAS1 polymorphism by RFLP-PCR
The presence of the AA genotype at the exon 7 SAS was specified by complete digestion of the 203 bp PCR product into two fragments: 150 bp and 53 bp by AluI enzyme (AGCT). The GG genotype at the exon 7 SAS was specified by absence of AluI site where A to G polymorphism created an indigestible sequence (GGCT) with a retained intact of 203 bp PCR fragment. The heterozygous (AG) condition at the exon 7 SAS of OAS 1 gene was represented by three fragments of 203 bp, 150 bp and 53 bp on agarose gel electrophoresis (Fig. 1).
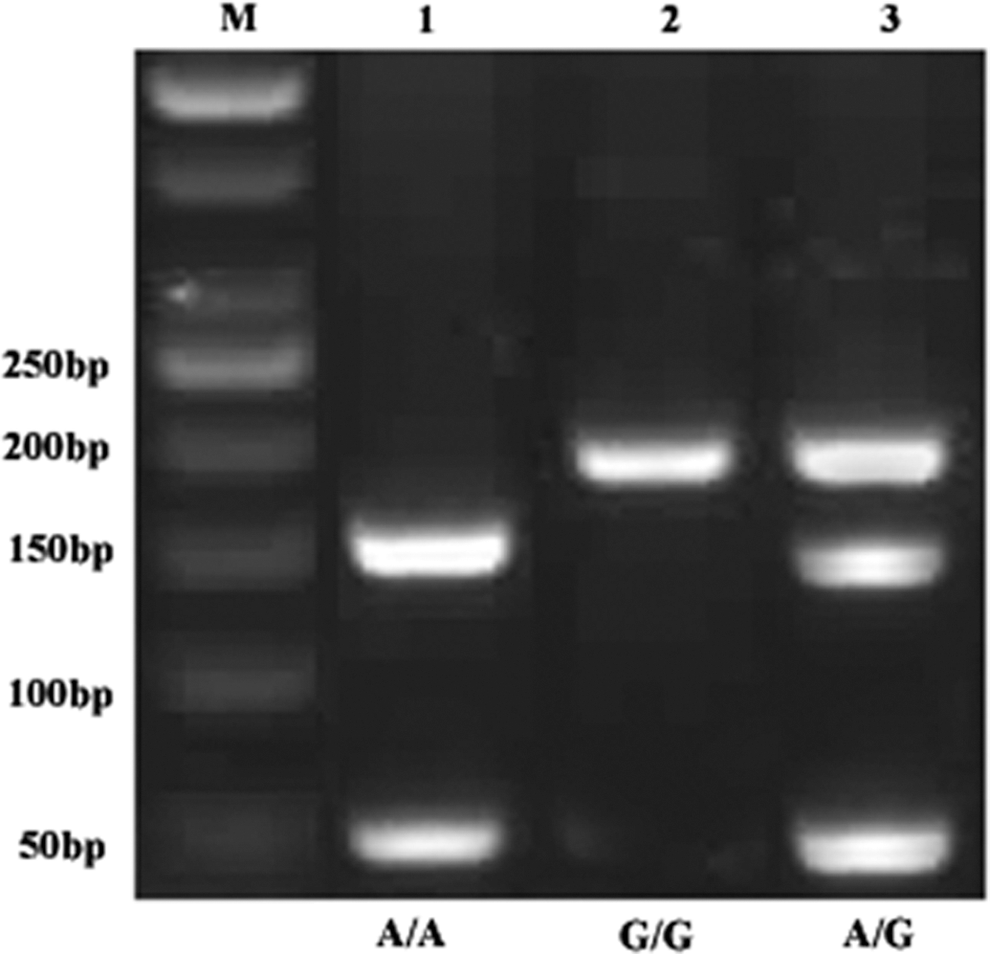
Electrophoresis pattern of three different individuals by RFLP-PCR analysis. Lane M, 50 bp marker; Lane 1, homozygous A genotype; Lane 2, homozygous G genotype; Lane 3, heterozygous A/G genotype of OAS1 gene.
Frequency of OAS1 genotypes in healthy and patient groups
One hundred and twenty healthy subjects from both sexes were also enrolled in this study to determine whether the tested SNP represents an important genetic component of the Pakistani population. The frequency of OAS1 gene polymorphism at exon 7 SAS was tested in both healthy and patient groups to unravel any association of this particular SNP with chronic HCV infection. The distribution frequency of OAS1 genotypes among the healthy subjects were; 62%, 33%, and 5% for genotypes GG, GA, and AA, respectively, while the frequency distribution of OAS1 genotypes among the patient subjects were; 69%, 25%, and 6% for OAS1 genotypes GG, GA, and AA. The results showed that G allele (70%) tends to be more frequent than A allele (30%) in both control and infected individuals. There were no significant differences in OAS1 genotypes distribution between healthy and patient groups. This indicates that there is no association of any OAS1 genotype with the natural clearance of HCV infection (Fig. 2).
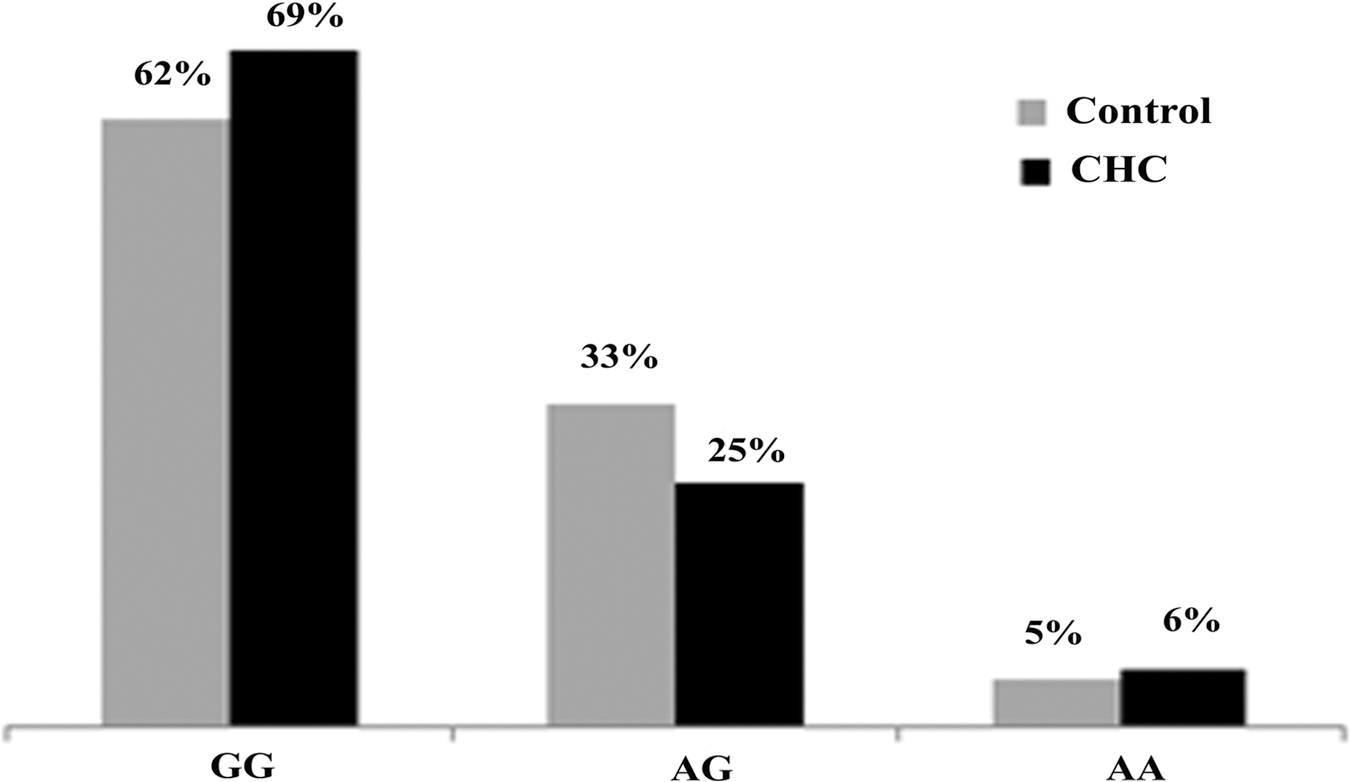
Comparison of OAS1 polymorphism distribution between healthy controls and chronic hepatitis C patients.
Frequency of OAS1 genotypes in SVR and NR groups
The patient group was further divided into SVR and NR groups in order to find any correlation of this particular SNP with interferon-based therapy of HCV infection in our population. The distribution frequency of OAS1 genotypes between the two groups were compared and analyzed by Pearson Chi square analysis. It was found that the frequency of GG genotype was significantly higher in SVR group than NR group (73% vs. 53%; p=0.039). The frequency of other two genotypes of OAS1 gene (i.e., AG and AA) at this particular position were comparable in both SVR and NR groups, representing a nonsignificant association of these genotypes with interferon-based therapy of HCV infection. The high prevalence of GG in SVR group suggests that individuals possessing this genotype at exon 7 SAS of OAS1 gene are better responders to interferon-based therapy of HCV infection (Fig. 3).
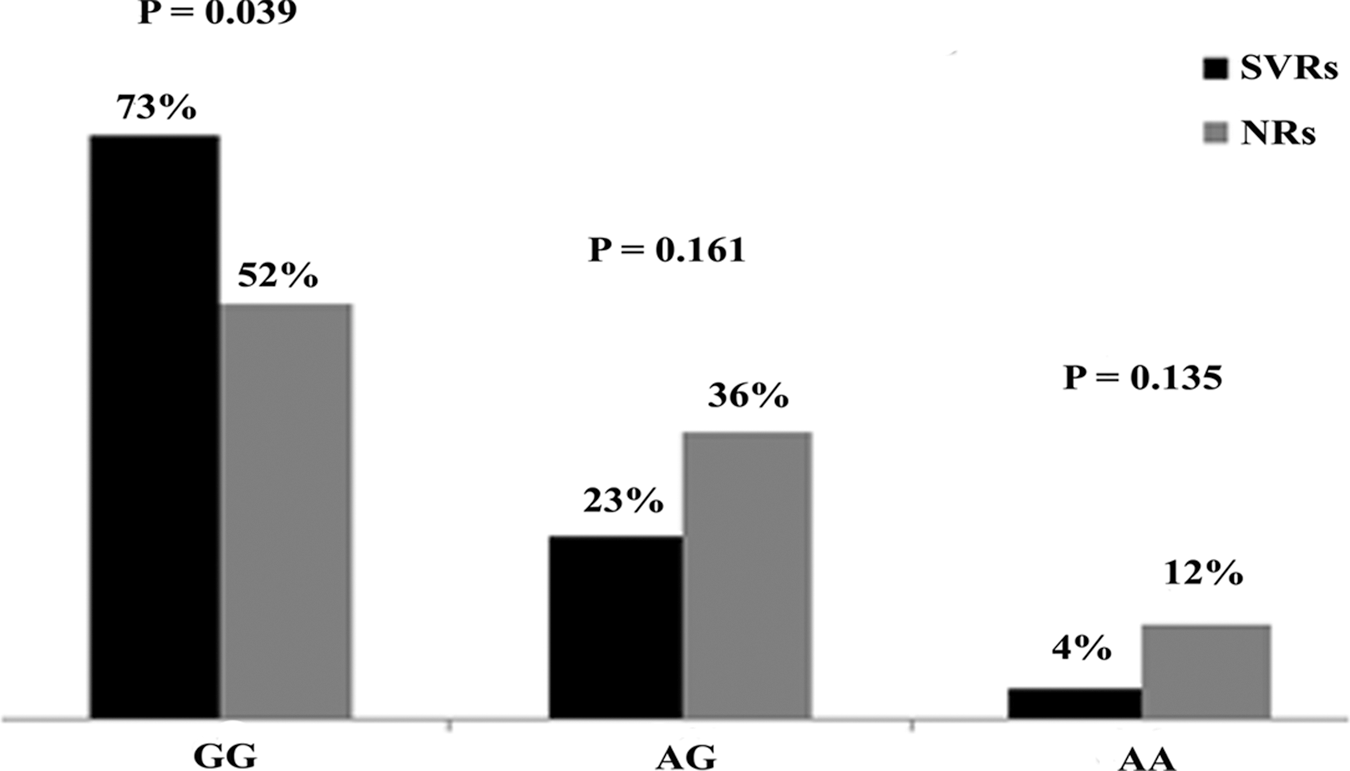
Comparison of OAS1 polymorphism distribution between SVRs and NRs. The p values were calculated by Pearson Chi square test.
HCV genotypes vs. OAS1 genotypes
The most common HCV genotype was 3. Previous studies have also shown that HCV genotype 3 is the most prevalent genotype in Pakistan (32). For genotype 3 (both 3a and 3b) most of the patients possessing OAS1 GG genotype achieved SVR (i.e., 39 out of 41 patients). Patients with HCV genotype 3 and OAS1 AG genotype also succeeded in achieving SVR (39 out of 46) (Table 2).
Discussion
HCV infection is a major global health problem. An estimated 10 million people (6%) in Pakistan are infected with HCV (42). Only 20%–30% of patients are expected to be free of the virus within 6 months of infection. 70%–80% of acute HCV infections become chronic. During the last 2 decades, extensive research work has been done to unravel the association of pathogen and host's genetics on pathogenesis of common diseases. For this purpose, SNPs in the human genome are specifically targeted to find their associations with susceptibility, resistance, or treatment response to various diseases (12,26). Both host and viral factors play an important role in outcome of HCV infection and its response to interferon-based therapy. HCV possesses extensive sequence diversity in its genome because of its error-prone RNA-dependent RNA polymerase resulting in different subtypes and genotypes (34). OAS1 gene is an important component of the signaling pathway of interferon. Its homolog in mice has demonstrated susceptibility against flaviviruses (25). Our results suggest that there is a significant association of OAS1 gene polymorphism at exon 7 SAS with interferon-based therapy of HCV infections, confirming the previous reports of El-Awady et al. (9). Patients with GG genotype at this position achieved more SVR (p=0.039) on interferon-based therapy as compared to the patients possessing either GA or AA genotypes. Our results suggest that G allele conferred better functional capability to OAS1 enzyme towards the viral clearance. These results established the earlier reports that G allele at exon 7 SAS of OAS1 gene is associated with higher enzyme activity (P46). On the other hand, A allele at this site (AA genotype) resulted in enzyme with higher weight but lower activity (P48). Furthermore, it was shown that patients possessing AA genotype are poorer responders to interferon-based therapy in an Egyptian population. The response rate to interferon-based therapy of HCV infection for OAS1 gene polymorphism at exon 7 SAS was gradually increased from AA to AG and then to GG genotype (2). A recent report from China has shown that three SNPs of OAS1 gene (rs2660 G/A, rs10774671 G/A, and rs3741981 G/A) are in linkage disequilibrium. The A allele at these three loci was significantly more common in chronic HCV patients as compared to healthy controls (p=0.001). Moreover, it was found that A allele at these loci also increased the risk of chronic HCV infection (46). The minor allele frequency (MAF) (i.e., G allele) in our population was 0.496. Data from Ensembl genome browser show that MAF in Africa, America, and Han Chinese in Bejing, China is 0.587, 0.301, and 0.309, respectively.
There is substantial number of studies showing that human genetic differences have an important role in disease progression and treatment response. Recently, it has been discovered that SNPs of the interferon lambda group are strongly associated with interferon plus ribavirin therapy of HCV infection (12). Further investigation of IL28B rs12979860 has demonstrated that this variant is actually located within IFNL4. There are two alternative forms of IFNL4: IFNL4 deltaG that produces protein while the other alternative form is without deletion and produces no protein. IFNL4 deltaG was found to be more prevalent in African American and European American populations. The presence of IFNL4 deltaG protein was responsible for poorer response and viral clearance in this population. It was concluded that in African Americans and European Americans, IFNL4 deltaG is better predictor of pegylated interferon plus ribvirin treatment of HCV infection than IL28B genotype. However, currently new direct acting agents against HCV infection are being developed and the role of IFNL4 deltaG in the era of DAA is still to be determined (14).
The present study confirmed that mutation at exon 7 SAS of OAS1 gene is significantly associated with interferon-based therapy of chronic HCV infection. However, the main limitation of our study was a small sample size. Although the sample size of HCV genotype 3 was larger, the sample size of other genotype was not large enough to apply statistics on each genotype separately. Moreover, we did not study other SNPs of OAS1 gene that are in linkage disequilibrium with this particular SNP. The haplotype study of OAS1 gene may further highlight the importance of OAS1 gene in interferon-based therapy of HCV infection. However, our pilot study highlighted the importance of this SNP for interferon-based therapy of HCV infection in our population. Currently, there are discoveries of new therapeutic options for HCV infection; the importance of these SNPs in association with these new therapeutic options will also be studied.
Conclusion
The current SOC for HCV infection is interferon plus ribavirin but it is expensive and associated with serious side effects. It is very necessary to have some predicative markers for the treatment response. We evaluated the distribution of OAS1 genotypes and their response to interferon plus ribavirin treatment in chronically infected HCV patients of the Pakistani population. There were no significant differences in distribution of OAS1 polymorphism between patients and healthy subjects. However, the frequency of OAS1 GG genotypes was higher in the SVR group than NR group, suggesting the protective role of this genotype in response to interferon-based therapy of HCV infection. In conclusion, OAS1 polymorphism at exon 7 SAS is an independent determinant that can predict outcome of interferon plus ribavirin therapy in case of HCV infection in our population.
Footnotes
Acknowledgments
SM and MI conceived the study, and did the analysis. MI and NMK performed all experiments. MI searched the literature and drafted the manuscript. NMK, MT, MK, and FJ helped MI in sample collection and data analysis. SM critically reviewed the manuscript. SM supervised and designed the study, gave final approval and helped MI in performing the research. All authors have read and approved the final version of the manuscript.
Funding: Financial support in part by National University of Sciences and Technology (NUST), H-12, Islamabad, Pakistan, and Higher Education Commission of Pakistan is highly acknowledged.
Author Disclosure Statement
The authors declare that they have no competing interests.