
Abstract
Sudan virus (SUDV) is a member of the Filoviridae family that has been associated with sporadic outbreaks of human disease in sub-Saharan Africa. The filoviruses are notable for the high frequencies with which they cause both hemorrhagic manifestations and death in infected individuals. Recently, we reported an extensive biomarker analysis of patient specimens from the Gulu SUDV outbreak. In that study, we found evidence of endothelial dysfunction and alterations of factors important to the coagulation pathways. The complex intersection between the endothelium, coagulation, and immunity is further explored in this study where we examine several additional biomarkers using the same patient specimens. We report that von Willebrand factor (vWF), a protein that promotes platelet adhesion to the injured endothelium, is elevated in SUDV-infected individuals compared to normally reported values in healthy individuals. Furthermore, vWF is associated with a fatal outcome in SUDV-infected pediatric patients. In addition, we find that vWF is elevated in individuals who have hemorrhagic manifestations of disease, suggesting excessive thrombosis in these patients.
S
Our previous data suggested a protective role for activated platelets during SUDV infection, since the vast majority of sCD40L is derived from activated platelets. Platelets function on the endothelial surface not only to initiate thrombus formation but also as mediators of innate and adaptive immune responses (16). Therefore, we sought to examine additional biomarkers of platelet–endothelial interactions using this same set of patient samples.
Four biomarkers were chosen for additional analysis: P-selectin, L-selectin, a disintegrin and metalloproteinase with thrombospondin motifs-13 (ADAMTS13), and von Willebrand factor (vWF). P-selectin is an adhesion molecule that is produced by activated platelets and endothelial cells that facilitates interactions with leukocytes (3). L-selectin is an adhesion molecule that is produced by leukocytes that allows them to tether to activated endothelial cells (12). ADAMTS13 is an enzyme that is produced by endothelial cells that is responsible for the cleavage of vWF; this enzyme is reduced or deficient in patients with thrombotic thrombocytopenic purpura (17). vWF is a protein that is made by both platelets and the endothelium that mediates platelet adhesion to the injured endothelium and localized platelet aggregation; levels of this protein are low in patients with von Willebrand disease, which manifests as a bleeding disorder (7).
Multiplex assays were obtained from Millipore (Billerica, MA) and performed on patient serum samples according to the manufacturer's instructions. The patient population included 86 patients aged 6–60 years, of whom 37 patients were aged 6–21 years, and 49 were aged 22–60 years. Thirty-five percent were male. Thirty-six per cent had hemorrhagic manifestations (defined as any form of bleeding to include hematemesis, melena, hematochezia, or mucosal bleeding), and 48% of patients had a fatal outcome (9). The additional data obtained from these new analyses were input into the same database that was created for the initial analysis (detailed in (9)), and an analysis of variance was conduced to determine the significance of each analyte for the variables examined (age, sex, hemorrhagic manifestations, day post-symptom onset, HIV status, viremia, and survival outcome).
P-selectin and ADAMTS13 were not significant for any variable (data not shown). L-selectin was only significant for age in that pediatric patients had higher levels than adults, and this has been previously reported (11). However, vWF demonstrated statistical significance for clinical outcomes during SUDV infection. Normal serum levels of vWF are approx. 10 μg/mL (7). All SUDV-infected patients had higher than normal levels of vWF. Pediatric patients who had fatal outcomes had higher levels of vWF than those who had nonfatal outcomes, while adults had similar levels of this factor regardless of outcome (Fig. 1A). Interestingly, during the later times of infection, 11–15 days post-symptom onset, levels of vWF were very low in fatal pediatric patients. This likely represents consumption of the protein over time during prolonged inflammation and has also been reported in children with severe dengue (2). Infected individuals who had hemorrhagic manifestations of disease had higher levels of vWF than patients who did not have hemorrhagic manifestations, and this was not age dependent (Fig. 1B).
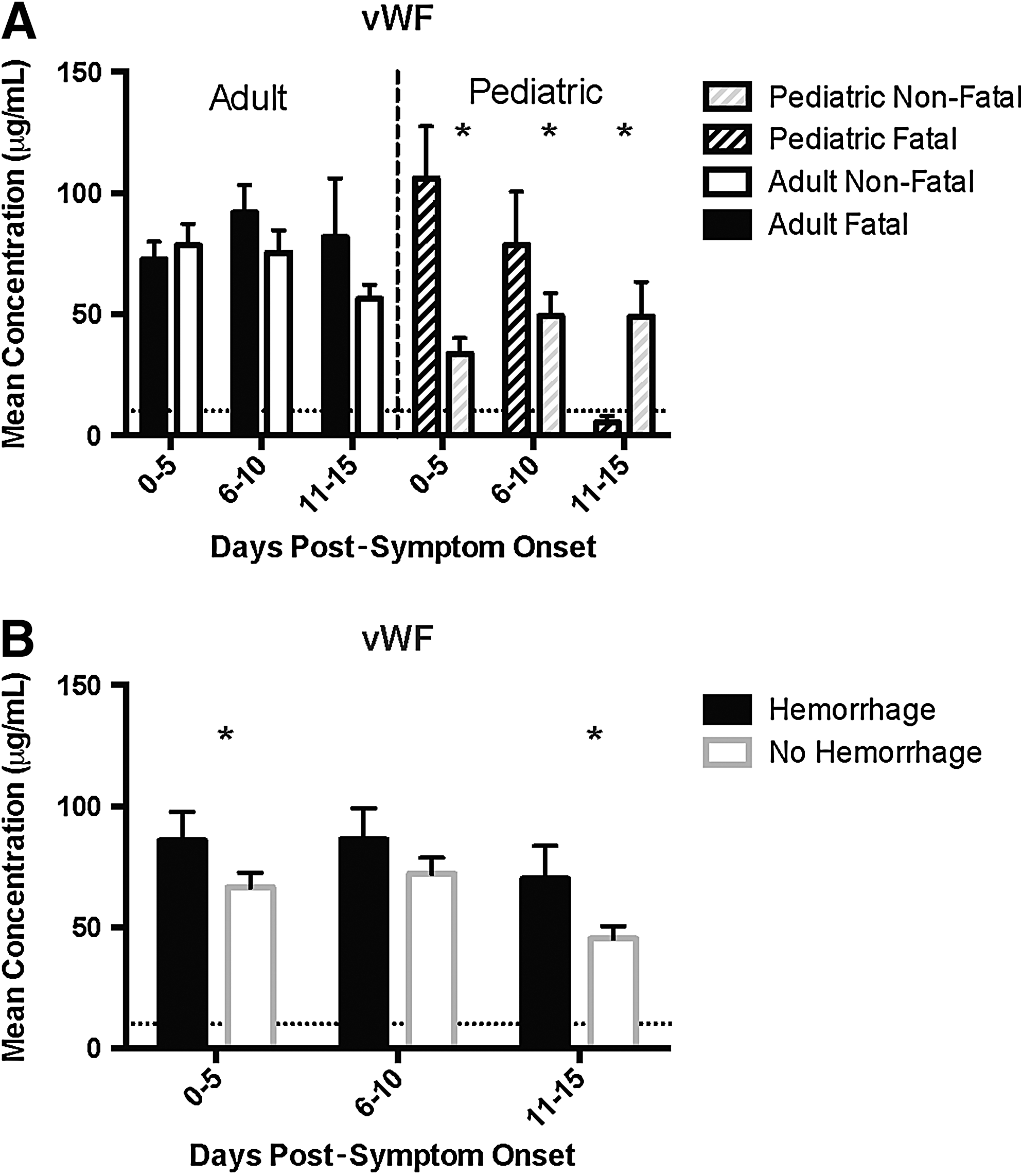
von Willebrand factor (vWF) levels are associated with adverse outcomes in Sudan virus–infected patients. (
Platelets play a critical role in hemostasis; they bind to damaged endothelial surfaces and, once activated, release the contents of secretory vesicles, promoting coagulation and leukocyte binding. vWF is released from activated platelets and from the Weibel-Palade bodies of activated endothelial cells. vWF provides a bridge via which platelets interact with the exposed subendothelial surface of a damaged endothelium, and it also complexes with and stabilizes coagulation factor VIII. Elevated levels of vWF have been shown to correlate with disease severity for several other infectious diseases: malaria, dengue virus, Puumala hantavirus, and in patients with sepsis (2,5,10,15). In our study, elevated levels of vWF were seen in all infected individuals, but only pediatric patients demonstrated an association between elevated levels and fatal outcome. The vast majority of vWF is derived from activated endothelial cells, and we have detected increased levels of two other markers of endothelial activation—sVCAM and sICAM—in these same pediatric patients. These data support our hypothesis that excessive endothelial activation/reactivity contributes to pediatric mortality and suggests the potential for specific therapies in management of pediatric SUDV disease.
While an activated endothelium is one explanation for the association between fatal outcome and elevated vWF in pediatric patients, an alternative explanation is that increased levels of vWF could be associated with intravascular thrombosis either locally or systemically and this would be expected to be deleterious to cardiovascular function. This would also be consistent with the notion that severely ill filovirus-infected patients can develop disseminated intravascular coagulopathy (DIC). The presence of DIC has not yet been strictly proven in the context of any filovirus outbreak because the scoring system recommended by the International Society for Thrombosis and Haemostasis for the diagnosis of DIC requires measurement of platelets, fibrinogen, PT, and fibrin degradation products simultaneously, and these measurements are not routinely performed in the outbreak setting (6). However, there have been individual circumstances in which access to tertiary care was available where a filovirus-infected individual clearly demonstrated DIC (13). Our finding that SUDV-infected patients who experienced hemorrhagic manifestations had higher levels of vWF than those who did not have hemorrhagic manifestations is consistent with the reported associations between DIC and elevated levels of vWF in several different diseases (4).
One limitation to our study is that we were only able to measure total vWF antigen levels. Furthermore, we were not able to distinguish between high molecular weight multimers or the propeptide, nor were we able to estimate vWF activity using a conformation specific assay. This limitation was secondary to the fact that we only had very limited microliter quantities of patient serum available for study. Despite this, we detected statistically significant differences in vWF levels as a function of adverse patient outcomes. Interestingly, there exists a soluble chimeric GPIbα (the receptor on platelets for vWF) conjugated with the Fc fragment of human IgG (GPG-290) that can inhibit the interaction between vWF and platelets, and administration of this to mice prevents the formation of thrombi (1). Whether this has the potential to be of therapeutic use in patients who are infected with SUDV remains to be determined, but warrants study in the available animal models.
Footnotes
Acknowledgments
A.K.M is supported by the PIDS/St. Jude Fellowship Award and the Atlanta Pediatric Scholars Award (NIH K12 HD072245). This work was performed while she held an NIH Loan Repayment Award.
Author Disclosure Statement
No competing financial interests exist.