
Abstract
CD163, a hemoglobin scavenger receptor for haptoglobin-hemoglobin complexes, is expressed by monocytes/macrophages and is often shed as soluble CD163 (sCD163) in response to inflammatory stimuli. This scavenger receptor is reported to dampen the inflammatory response, and high plasma levels of sCD163, which are thought to reflect the total level of CD163 expression, may predict the severity of disease. To understand the role of sCD163 in the pathogenesis of hemorrhagic fever with renal syndrome (HFRS) better, the concentrations of sCD163 in plasma from 66 patients were quantified, and the relationships between sCD163 level and disease course, severity, and clinical parameters were analyzed. The level of plasma sCD163 in HFRS patients was elevated from fever onset and during the course of the disease, and it peaked in the oliguria stage at 874.5 (549.9–1138.0) ng/mL compared with controls at 192.8 (54.9–282.1) ng/mL. The correlations between plasma sCD163 and renal dysfunction suggest that sCD163 may play an important role in the development of acute renal failure in patients infected with Hantaan virus.
Introduction
H
At present, the pathogenesis of HFRS is still unclear. It is believed that the induction of an uncontrolled immune response to the hantavirus infection, rather than the viral infection itself, is the major cause of the microvascular leakage and development of HFRS. Because the kidneys are the major organ that are pathologically damaged during HFRS with the most prominent finding of acute tubulointerstitial nephritis with infiltration of inflammatory cells, AKI has been thought to be involved in the high mortality rate of HFRS (8,16).
CD163, which belongs to the scavenger receptor cysteine-rich (SRCR) superfamily, is a 130 kDa endocytic receptor for haptoglobin-hemoglobin (Hp-Hb) complexes that is exclusively expressed in the monocyte–macrophage lineage (9). In addition to being present on the macrophage surface, continuous shedding of the extracellular domain of CD163, catalyzed by the metalloproteinase ADAM17, leads to substantial amounts of soluble CD163 (sCD163) in plasma (3). Inflammatory stimuli lead to increased shedding of CD163. It is believed that the plasma concentration of sCD163 may reflect its general expression level (1). Many clinical studies have further revealed that in several infectious diseases such as human immunodeficiency virus (HIV) (2), chronic hepatitis B/C (7), and scrub typhus (13), levels of sCD163 elevated in patient serum/plasma are associated with disease severity. Additionally, elevated sCD163 is associated with organ dysfunction. The rise of sCD163 is notably more pronounced in patients who develop liver dysfunction or new kidney injury than in those who do not (5). AKI is one of the most prominent and characteristic manifestations of the HFRS disease, especially in the severe form HFRS (15). Therefore, monitoring the levels of plasma sCD163 in HFRS patients may aid in predicting the development of AKI in patients infected with HTNV and help delineate the pathogenesis of the disease.
In this study, the levels of sCD163 were measured in plasma from HFRS patients and compared throughout the course of the illness. Furthermore, the relationships between the levels of sCD163 and the clinical parameters were systemically analyzed. The findings indicate that sCD163 might act as a marker for the development of AKI in patients infected with HTNV, and provide evidence to suggest that the scavenger receptor might have a potential role in the pathogenesis of HFRS.
Materials and Methods
Sample preparation
A total of 66 hospitalized adult patients diagnosed with HFRS were enrolled in this study between 2012 and 2013 at the Department of Infectious Diseases at the Tangdu Hospital of The Fourth Military Medical University (Xi'an, China). A clinical diagnosis of HFRS was serologically confirmed by the detection of immunoglobulin M (IgM) or IgG antibodies specific to HTNV. Plasma samples were collected intravenously from 66 HFRS patients (51 male; age range 18–69 years) while in hospital. All samples were frozen at –80°C until use. The clinical parameters were collected using routine hospital laboratory techniques. The study was approved by the Institutional Review Board of the university, and all individuals provided written informed consent.
HFRS disease severity was classified on the basis of clinical and laboratory parameters used in the diagnostic criteria for HFRS in China as (a) mild: mild renal failure without an obvious oliguric stage; (b) moderate: obvious symptoms of uremia, effusion (bulbar conjunctiva), hemorrhage (skin and mucous membrane), and renal failure with a typical oliguric stage; (c) severe: severe uremia, effusion (bulbar conjunctiva and either peritoneum or pleura), hemorrhage (skin and mucous membrane), and renal failure with oliguria (urine output, 50–500 mL/day) for ≤5 days or anuria (urine output, <50 mL/day) for ≤2 days; and (d) critical: for those with more than one of the following symptoms during severe disease: refractory shock, visceral hemorrhage, heart failure, pulmonary edema, brain edema, severe secondary infection, and severe renal failure with either oliguria (urine output, 50–500 mL/day) for >5 days, anuria (urine output, <50 mL/day) for >2 days, or a blood urea nitrogen level of >42.84 mmol/L (16). Severe AKI was defined as either receipt of dialysis or serum creatinine ≥354 μmol/L (15).
For the present study, 15 healthy adult volunteers without a history of HFRS-like disease were selected as control donors.
Enzyme-linked immunosorbent assay
The levels of sCD163 and C-reactive protein (CRP) in plasma were determined with enzyme-linked immunosorbent assay (ELISA) kits (eBioscience or Biovendor, respectively) according to the protocol. Plasma samples of 100 μL were used for each test. The optical densities were determined at 450 nm. The concentrations of sCD163 and CRP in the tested samples were estimated from a standard curve as calculated with serially diluted reconstituted sCD163 or CRP standards.
Statistical analysis
Statistical analysis was performed using SPSS for Windows v13.0 (SPSS, Inc.) and GraphPad Prism v5.0 (GraphPad Software, Inc.). Continuous variables were analyzed by the Kolmogorov–Smirnov test for normality of distribution, and Levene's test for the homogeneity of variance. For the non-normally distributed variables, the nonparametric Mann–Whitney U-test was used. Nonparametric Spearman correlation analysis was used to evaluate the associations between sCD163 levels and the clinical parameters. Receiver operating characteristic (ROC) curves were constructed to assess the sensitivity and specificity of the sCD163 level in predicting the development of AKI. The area under the ROC curves (AUC) and corresponding 95% confidence intervals (CI) were calculated. All p-values are two-sided, and p-values of <0.05 were considered significant.
Results
sCD163 levels were first determined by ELISA. A panel of 135 plasma samples from 66 HFRS patients and 15 healthy donors was examined. The information for these samples is summarized in Table 1. The median level of sCD163 with its corresponding interquartile range in the plasma samples from all HFRS patients was elevated to 663.5 (420.0–1004.0) ng/mL, which was 3.4-fold higher than that in the plasma samples from healthy controls, which was 192.8 (54.9–282.1) ng/mL (p<0.001; Fig. 1A). Considering severity levels, the median levels of plasma sCD163 with their corresponding interquartile ranges were 712.2 (225.3–1094.0) ng/mL in the mild group, 582.4 (322.7–923.2) ng/mL in the moderate group, 696.0 (485.0–923.2) ng/mL in the severe group, and 874.5 (529.6–1329.0) ng/mL in the critical group. The levels in all four groups were elevated compared with healthy controls (p<0.05) and reached their peak in the critical group, but without a difference between the groups (p>0.05; Fig. 1B). Then, the plasma sCD163 level was studied in HFRS patients at each stage of the disease, irrespective of the severity. The median levels of plasma sCD163 with their corresponding interquartile ranges were 663.5 (330.8–1077.0) ng/mL in the febrile/hypotensive stage, 874.5 (549.9–1138.0) ng/mL in the oliguric stage, 631.0 (355.1–951.6) ng/mL in the diuretic stage, and 687.9 (493.1–1309.0) ng/mL in the convalescent stage (Fig. 1C). In general, the sCD163 levels in the four groups were all elevated compared with those in the healthy controls. The dynamic changes in the different stages showed that the median levels of plasma sCD163 in HFRS patients reached their peak in the oliguric stage (Fig. 1C).
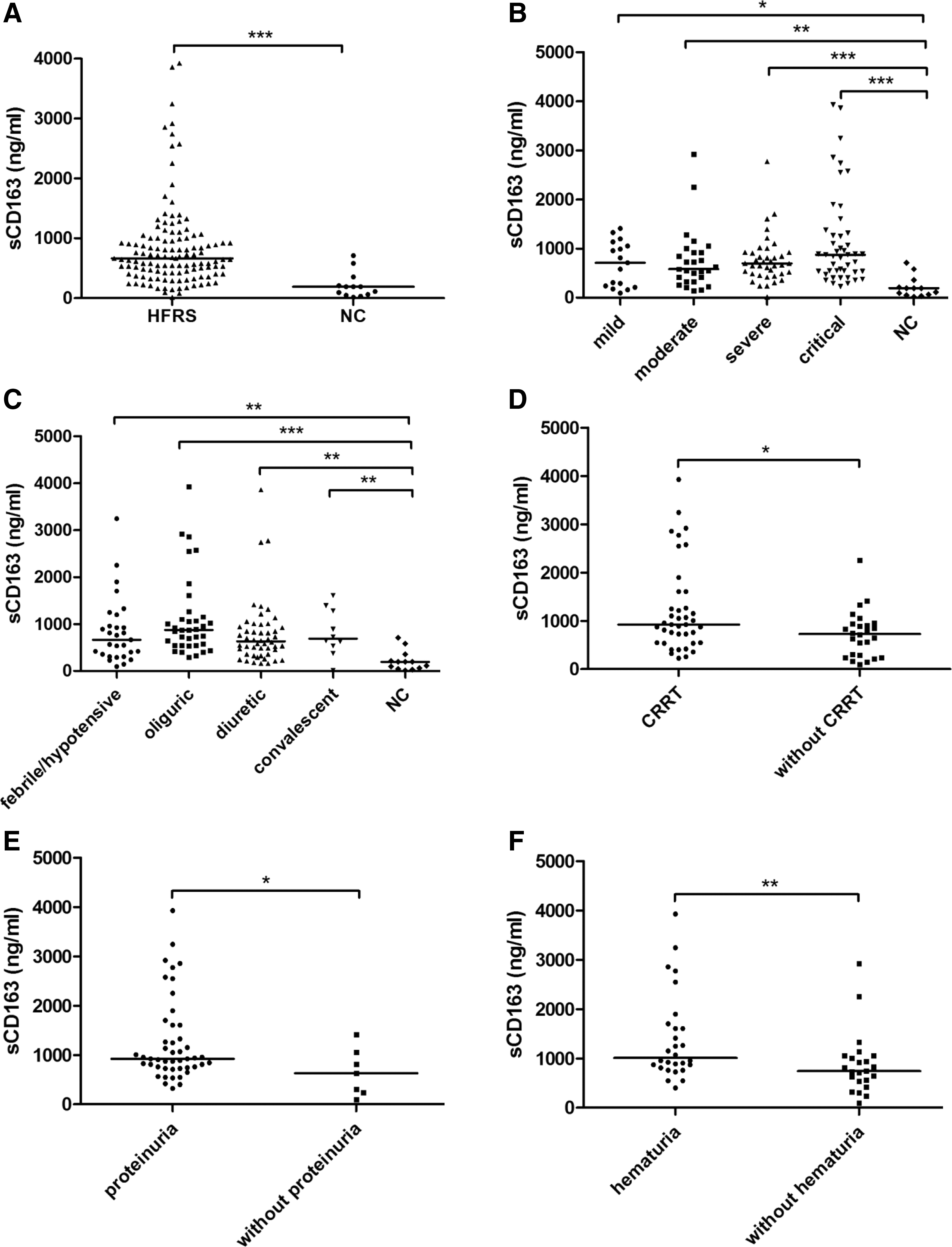
Comparison of plasma sCD163 in different hemorrhagic fever with renal syndrome (HFRS) groups. (
HFRS, hemorrhagic fever with renal syndrome.
Of the 66 HFRS patients, 40 (60.6%) received one or more sessions of continuous renal replacement therapy (CRRT) treatment. The sCD163 level was higher in the CRRT treatment group than in patients without CRRT treatment (Fig. 1D). Among the 66 HFRS patients, 47 patients suffering from proteinuria and 28 with hematuria in different ranges had much higher sCD163 levels in their plasma (Fig. 1E and F).
Further, the relationships were analyzed between plasma sCD163 levels and the clinical parameters detected during hospitalization. It was found that the peak level of sCD163 during the entire clinical course of each patient was positively correlated with their corresponding peak blood urea nitrogen (BUN; r=0.361, p=0.003; Fig. 2A), peak serum creatinine (Crea; r=0.284, p=0.012; Fig. 2B), CRP (r=0.223, p=0.007; Fig. 2D), and the length of hospital stay (r=0.295, p=0.009; Fig. 2E), whereas it was inversely associated with the nadir platelet count (PLT; n=−0.130, p=0.026; Fig. 2C). Additionally, a ROC curve for the peak levels of sCD163 was made to predict the development of AKI, and the AUC was 0.66 (95%CI 0.51–0.81; Fig. 2F).
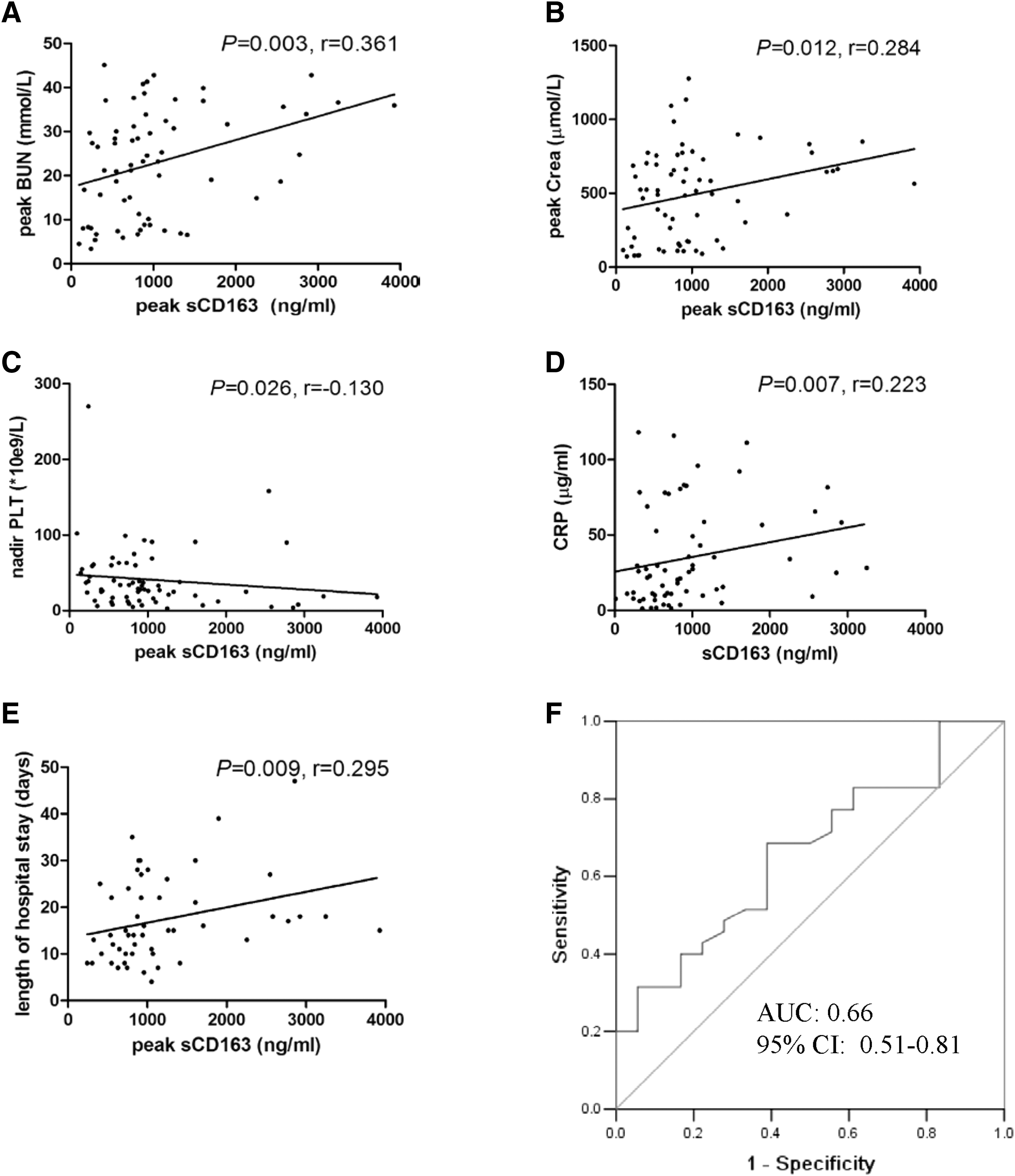
Correlations of sCD163 with clinical parameters. Shown are the levels of (
Discussion
In this study, plasma samples from a cohort of HFRS patients were used, and it was found that the level of plasma sCD163 was substantially increased in HFRS patients after HTNV infection, especially in the critical group. The dynamic analysis suggested that the elevation began from the onset of fever and reached its peak level at the oliguric stage of the disease (Fig. 1). The associations between sCD163 level and clinical parameters reflecting renal dysfunction suggest that sCD163 could be a novel biomarker of acute renal failure in HFRS (Fig. 2A–E). The ROC curve (Fig. 2F) also confirmed the accuracy of using the peak plasma level of sCD163 as a predictive biomarker for the development of AKI in HFRS patients.
sCD163 is reported to be a promising activation marker for monocytes/macrophages (11). It is believed that CD163-positive monocytes/macrophages may play a role in the resolution of inflammation because CD163 can fuel an anti-inflammatory response by directly leading to the secretion of anti-inflammatory cytokines or by delivering hemoglobin to macrophages (10). Additionally, it has been proposed that sCD163 contributes to innate immune defenses by sequestering hemoglobin iron that would otherwise be available to pathogens (17). However, given the lack of a proper animal model of HFRS at present, their anti-inflammation roles cannot be demonstrated in vivo during HTNV infection.
The expression of CD163 has been reported to be regulated by a variety of factors. The glucocorticoids and anti-inflammatory mediators such as IL-10 promote CD163 expression. Inversely, pro-inflammatory mediators such as LPS, IFN-γ, and TNF-α suppress CD163 expression (4). It has been indicated that the plasma concentration of sCD163 may reflect its general expression level (1). It was hypothesized that HTNV infection triggers innate immune responses, including Toll-like receptor (TLR) 4 pathways (18), and then induces the shedding of CD163. The constantly increasing level of sCD163 during the entire course of HFRS may be regulated by the anti-inflammatory cytokines produced during HTNV infection and may act as a feedback mechanism to the HTNV infection.
HFRS is an infectious disease mediated by immune and inflammatory responses. Little is known about the development of AKI in patients infected with HTNV. Previous studies have suggested that inflammatory mediators secreted by monocytes/macrophages are thought to contribute to the “cytokine storm” during HTNV infection and may be involved in the development of AKI in HFRS patients (14). It was found that plasma levels of sCD163 peaked at the oliguria stage, which indicates that the activation of monocytes/macrophages during oliguria may be involved in AKI. The correlations between plasma sCD163 and the clinical parameters reflecting the severity of AKI underscore the importance of innate immunity during HTNV infection. Although there is still a lack of knowledge about how sCD163 sheds from the monocytes during HTNV infection and how scavenger receptors such as sCD163 play a role in the pathogenesis of HFRS, this study still provides evidence to exploit sCD163 as a potential diagnostic tool in the early stage of AKI during HTNV infection, and provides a basis on which to understand the roles played by monocytes and macrophages in the pathogenesis of HFRS.
Footnotes
Acknowledgments
This study was supported by The National Natural Science Foundation of China (no. 30930087) and the National Basic Research Program of China (no. 2012CB518905).
Author Disclosure Statement
No competing financial interests exist.