
Abstract
The proinflammatory cytokines transforming growth factor beta 1 (TGF-β1) and interleukin (IL)-31 have been implicated in tissue injury. However, whether TGF-β1/IL-31 are stimulated and elevated in response to liver injury that leads to fibrogenesis in hepatitis B virus–related liver cirrhosis (HBV-LC) remains unclear. To investigate the association between TGF-β1/IL-31 and stages of chronic HBV infection, serum TGF-β1, IL-9, IL-10,IL-17, IL-22, IL-23, IL-31, IL-33, and IL-35 were determined among patients with chronic hepatitis B (CHB; n=19), HBV-LC (n=20), and a normal control population (NC; n=18). Disease severity in patients with HBV-LC was assessed using model for end-stage liver disease (MELD) scores. Serum TGF-β1 and IL-31 levels were strongly positively linked in all subjects, and both correlated positively with IL-22, IL-33, and IL-17. TGF-β1 and IL-31 levels in the blood were both significantly higher in CHB and HBV-LC patients than in NC subjects. Elevated serum TGF-β1 and IL-31 levels were positively associated with albumin, alpha-fetoprotein, creatinine, white blood cell count, and platelet levels. Serum TGF-β1 and IL-31 were markedly higher in HBV-LC patients who did not have esophageal varices, and IL-31 had the highest sensitivity and specificity (90.9% and 66.7%, respectively) for indicating the absence of this complication. In summary, TGF-β1 and IL-31 were linked to progression from CHB to LC, and correlated well with the severity of HBV-LC. These findings suggest possible roles of the TGF-β1/IL-31 pathway in the pathogenesis of liver fibrosis during chronic HBV infection.
Introduction
T
Transforming growth factor-β1 (TGF-β1) has multiple functions, including that of a powerful inhibitor of DNA synthesis and cellular proliferation (20). It also facilitates cell differentiation and promotes the production of extracellular matrix by hepatic stellate cells, upon hepatic injury and inflammation (14). There is increasing evidence that TGF-β1 is a powerful profibrogenic mediator that participates in the development of LC (16,22,26).
Cluster of differentiation 4 (CD4)+ T-cells, especially the T helper cell type 2 phenotype (19), produce interleukin-31 (IL-31), a described pro-inflammatory cytokine. IL-31 activates and functions through the oncostatin receptor and heterodimeric receptors of IL-31 (2,6). There is evidence that the IL-31/IL-31R signaling pathway is closely involved in the pathogenesis of atopic, allergic, and inflammatory diseases such as nonatopic eczema (15), allergic contact dermatitis (5, 10), spontaneous urticaria (13), asthma (28), nasal polyps (11), and familial primary cutaneous amyloidosis (18). LC is a consequence of chronic liver injury and ongoing inflammation that is marked by accumulating infiltrates, including CD4+ T-cells. These may produce high levels of IL-31 that facilitate hepatic inflammation and contribute to the fibrotic process. Thus, whether IL-31 is involved in the pathogenesis of HBV-LC warrants investigation.
TGF-β1 functions are mediated through interaction with Smad proteins. The participation of Smad2/3 is indispensable in the TGF-β1-induced inflammatory process. Evidence indicates that TGF-β1 induces Smad2 phosphorylation, then activates the binding of Smad3 to the IL-6 promoter region (including IL-31, a new member of the IL-6 family) (4), and finally stimulates the IL-31-JAK-STAT signal pathway (1,17). Therefore, IL-31 is considered a downstream component of the TGF-β1-Smad2/3 pathway, and IL-31 levels increase with increases in TGF-β1 (17). Recently, studies have shown that the TGF-β1-Smad2/3/IL-31 pathway participates in the progression of bleomycin-induced pulmonary fibrosis in mice (17,25). This suggests that the TGF-β1-Smad2/3/IL-31 pathway could be active in cells and cytokines inducing fibrosis, a crucial part of the pathogenesis of LC.
It was hypothesized that the TGF-β1-Smad2/3/IL-23 pathway is closely involved in fibrosis leading to HBV-LC. This is because TGF-β1-Smad2/3/IL-23 has been implicated not only in hepatic inflammation, but also in inducing hepatic stellate cells to produce extracellular matrix leading to fibrosis. Delineation of the participation of the TGF-β1-Smad2/3/IL-23 pathway in fibrogenesis could improve the understanding of hepatic fibrosis, and help determine if modulation of TGF-β1 levels could reverse the fibrotic process.
In the present study, to address the potential roles of the TGF-β1/IL-31 pathway in liver fibrosis in HBV-LC, it was determined whether putative cytokines were associated with disease severity and complications. Specifically, the serum levels of TGF-β1, IL-9, IL-10, IL-17, IL-22, IL-23, IL-31, IL-33, and IL-35 were determined in patients with HBV-LC and chronic hepatitis B (CHB), and normal healthy controls, and investigated the association between the TGF-β1/IL-23 pathway and other cytokines and clinical indices of liver cell injury.
Methods
Subjects
Nineteen CHB and 20 HBV-LC patients were enrolled in this study (Table 1). The criteria for diagnoses of CHB and HBV-LC have been described previously (8,12,21,29). Excluded were patients with hepatitis A, C, or D, human immunodeficiency virus (HIV), or alcohol- or drug-induced hepatitis or autoimmune liver diseases. Blood samples were collected from enrolled patients in the morning after admission, who were hospitalized or followed up from July 2012 to November 2013 in the Department of Infectious Diseases, First Hospital of Quanzhou Affiliated to Fujian Medical University (Quanzhou, China). Eighteen healthy individuals who showed no history of chronic liver diseases or ongoing inflammation were designated as normal controls (NC), and blood samples were collected.
Numerical data are shown as the median (10th–90th percentile) and analyzed by the Kruskal–Wallis H test and Mann–Whitney nonparametric U-test. Statistically significant values are shown in bold.
NC, normal controls; CHB, chronic hepatitis B; HBV-LC, hepatitis B virus–related liver cirrhosis; MELD, model for end-stage liver disease; HBeAg, hepatitis B e-antigen; ALT, alanine aminotransferase; AST, aspartate transaminase.
The 20 HBV-LC patients were assessed for symptoms of hepatic decompensation (hypersplenism, esophageal varices, ascites, and infections such as spontaneous bacterial peritonitis, pneumonia, or septicemia) at the time of enrollment. Two clinical manifestations of LC—ascites and encephalopathy—and three lab tests—serum total bilirubin, creatinine levels, and prothrombin time—were used to determine the Child–Pugh score. The MELD score was calculated as 9.57× ln(serum creatinine)+3.78×ln(serum total bilirubin)+11.2×ln(international normalized ratio)+6.43. The Ethics Committee of the First Hospital of Quanzhou (No. 20130308) approved the study protocol, and each patient provided written informed consent.
Enzyme-linked immunosorbent assay
The plasma levels of TGF-β1, IL-9, IL-10, IL-17, IL-22, IL-23, IL-31, IL-33, and IL-35 were each determined by enzyme-linked immunosorbent assay (ELISA) in accordance with the manufacturer's instructions (Market, San Jose, CA). The optical density values were measured at 450 nm with a microplate reader (ELx800; BioTek Instruments, Winooski, VT), and converted into pg/mL using the standard curve generated by internal standards included in the same plates.
Biochemical, serological, and virological tests
An automated coagulation analyzer (IL TOP700; Werfen Group, San Jose, CA) was used to measure prothrombin time and the international normalized ratio. Serum albumin, alanine aminotransferase (ALT), total bilirubin, creatinine, and other biochemical indices were determined by automatic biochemical analyzer (Beckman LX-20; Beckman, Brea, CA). The HBV surface antigen (HBsAg), anti-HB surface antibodies, hepatitis B e-antigen (HBeAg), anti-HBe, total IgM anti-HB core antigen, anti-hepatitis C virus, anti-hepatitis D virus, HIV, and alpha-fetoprotein were all measured by Architect QT assay (Architect i2000 SR Immunoassay Analyzer; Abbott Diagnostics, Irving, TX). Serum HBV DNA was determined using a commercial real-time polymerase chain reaction kit in a PE 9700 Thermal Cycler (Perkin Elmer, Boston, MA) in accordance with the manufacturer's instructions. The detection limit of HBV DNA was 1×103 copies/mL.
Statistical analyses
All data were analyzed using SPSS v13.0 (SPSS, Inc., Chicago, IL). Continuous variables are expressed as the median (10th–90th percentile). The Kruskal–Wallis H test, Mann–Whitney nonparametric U-test, and chi-square tests were used to analyze significant differences. Diagnostic accuracies for complications were estimated by receiver operating characteristic curve (ROC). Spearman's rank correlation was performed between variables. A two-sided p-value of <0.05 was considered significant.
Results
Clinical data from the three groups
Eighteen of the 20 HBV-LC patients showed signs of hepatic decompensation (hypersplenism, esophageal varices, ascites, and infection) on the day of enrollment in the study. Specifically, 14 (70%) patients had hypersplenism, 9 (45%) had esophageal varices, 10 (50%) had ascites, and 6 (30%) had infections. Moreover, 7 (35%) patients were already complicated by hepatocellular carcinoma (HCC).
The HBV-LC patients were older than the NC group and CHB patients (p<0.001; Table 1). The patient gender ratios of the HBV-LC and CHB groups were similar. The mean HBV DNA, ALT, aspartate transaminase (AST), albumin, lymphocytes, hemoglobin, and platelet levels were clearly lower in the HBV-LC group compared with the CHB group (p<0.05). The international normalized ratio, granulocyte ratio, and MELD scores were higher in the HBV-LC group than in the CHB group (p<0.05). The proportion of those testing positive for HBeAg, and the levels of total bilirubin, direct bilirubin, globulin, alpha-fetoprotein, and creatinine were similar between the two patient groups.
Elevated levels of the TGF-β1/IL-31 pathway detected in HBV-LC patients
The serum cytokine levels were compared among the three groups (Fig. 1). The IL-31 levels of the HBV-LC group (19.4[4.3–124.2] pg/mL) were higher than those of the CHB group (7.5[1.6–50.5] pg/mL; p<0.05) and the NC group (3.9[0.3–20.0] pg/mL; p<0.001).
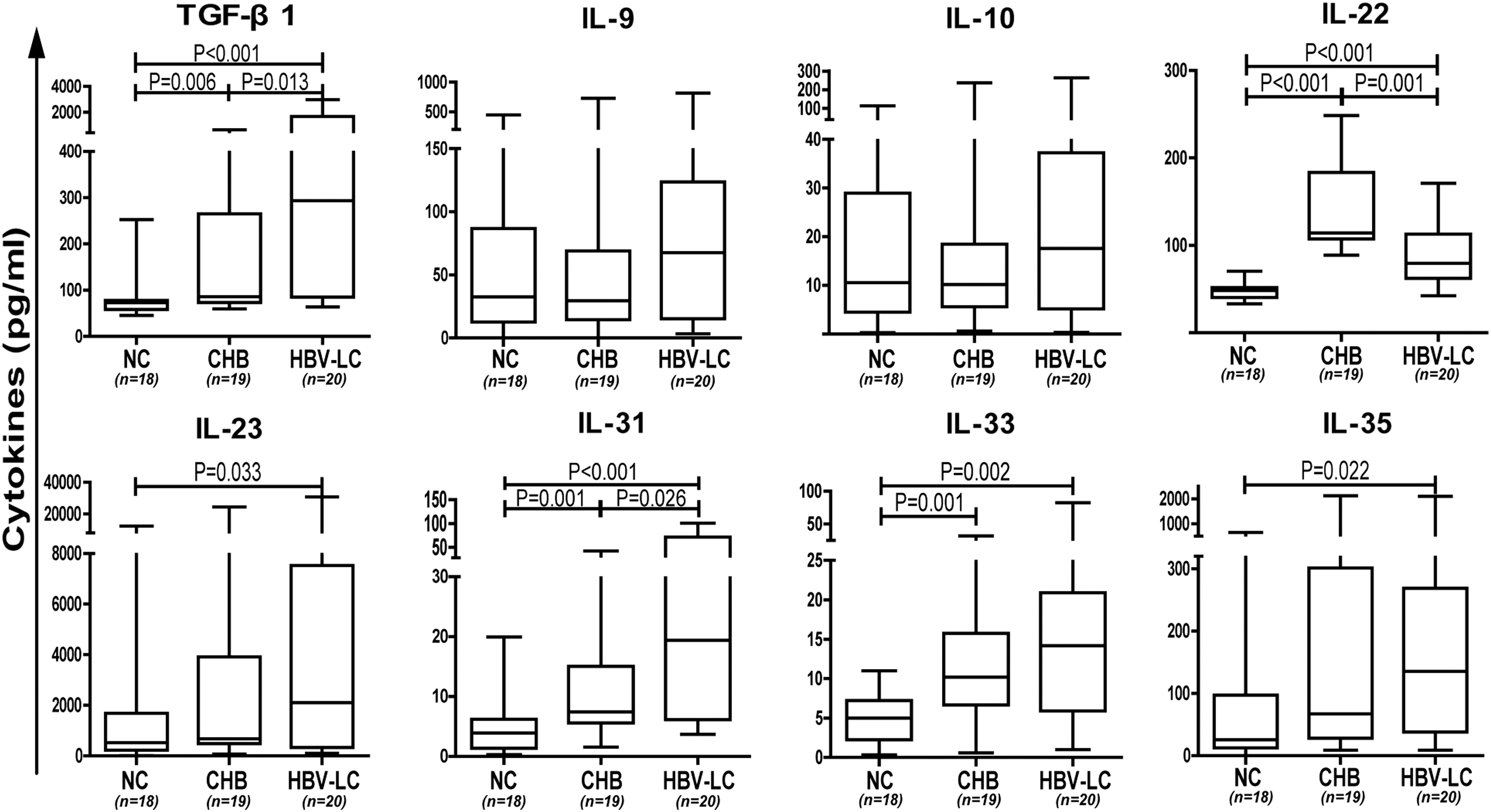
Serum levels of cytokines in three groups. Levels of transforming growth factor beta 1 (TGF-β1), interleukin (IL)-22, IL-23, IL-31, IL-33, and IL-35 were significantly higher in the hepatitis B virus–related liver cirrhosis (HBV-LC) group. Levels of IL-9 and IL-10 were similar in all three groups. Data are expressed as the median (range) and were analyzed by Mann–Whitney U-test. CHB, chronic hepatitis B; NC, normal control.
Similarly, the TGF-β1 levels of the HBV-LC group (293.6[63.7–2974.7] pg/mL) were higher than those of the CHB group (85.8[59.5–637.9] pg/mL; p<0.05) and the NC group (72.6[45.5–252.6] pg/mL; p<0.001).The differences in the TGF-β1 and IL-31 levels between the CHB and NC groups were also significant (p=0.006 and 0.001, respectively).
The IL-22 levels of the CHB group were significantly higher than those of the HBV-LC or NC groups (p<0.001). The IL-22 levels of the HBV-LC group were significantly higher than those of the NC group (p=0.001).
The levels of IL-33 of both the CHB and HBV-LC patients were significantly higher than those of the NC group (p<0.01), but between the CHB and HBV-LC groups, the IL-33 levels were similar.
The levels of IL-35 and IL-23 were significantly higher in the HBV-LC group compared with the NC group (p<0.05).
The IL-9 and IL-10 levels were similar among the three groups (p>0.05). Consistent with a previous finding (29), the serum IL-17 levels of the HBV-LC patients were significantly higher than those of the CHB and NC groups. It was also found that the IL-17 levels of the CHB group (46.3[18.4–63.8] pg/mL) were higher than those of the NC group (19.5[9.9–35.0] pg/mL; p<0.001) in the present study.
Association between liver disease severity and elevated TGF-β1/IL-31 pathway
Deteriorating hepatic synthesis capability and liver function decompensation are usually indicated by reduced albumin, white blood cell count, hemoglobin, and platelets, and elevated globulin, international normalized ratio, creatinine, and alpha-fetoprotein. Clinical indices of liver cell injury include ALT, AST, total bilirubin, and direct bilirubin.
In the combined HBV-LC and CHB patient groups (n=39), the levels of TGF-β1 and IL-31 negatively correlated with albumin and lymphocytes (Table 2). Moreover, the TGF-β1 and IL-31 levels of the patients positively correlated with globulin, white blood cell count, granulocyte ratio, platelets, and creatinine levels (Table 2). IL-31 levels positively correlated with international normalized ratio and total bilirubin. However, there was no correlation between TGF-β1 and IL-31 and ALT, AST, direct bilirubin, hemoglobin, or HBV DNA levels.
Statistically significant values are shown in bold.
TGF-β1, transforming growth factor beta 1; IL-31, interleukin-31.
In an earlier study, it was found that the activated TGF-β1/IL-31 levels correlated with the extent of liver injury and disease severity in HBV-related acute chronic liver failure (unpublished data). To explore if there was an association between the TGF-β1/IL-31 pathway and the severity of LC, the association between TGF-β1 and IL-23 levels and MELD score and Child–Pugh stages were analyzed in HBV-LC patients (n=20). As shown in Figure 2C and D, there were significant positive correlations between the MELD score and the serum levels of TGF-β1 (r=0.591, p=0.008) and IL-31 (r=0.570, p=0.011) in patients with HBV-LC. However, patients with higher Child–Pugh stage did not have detectably higher TGF-β1 and IL-23 levels (Fig. 2A and B).
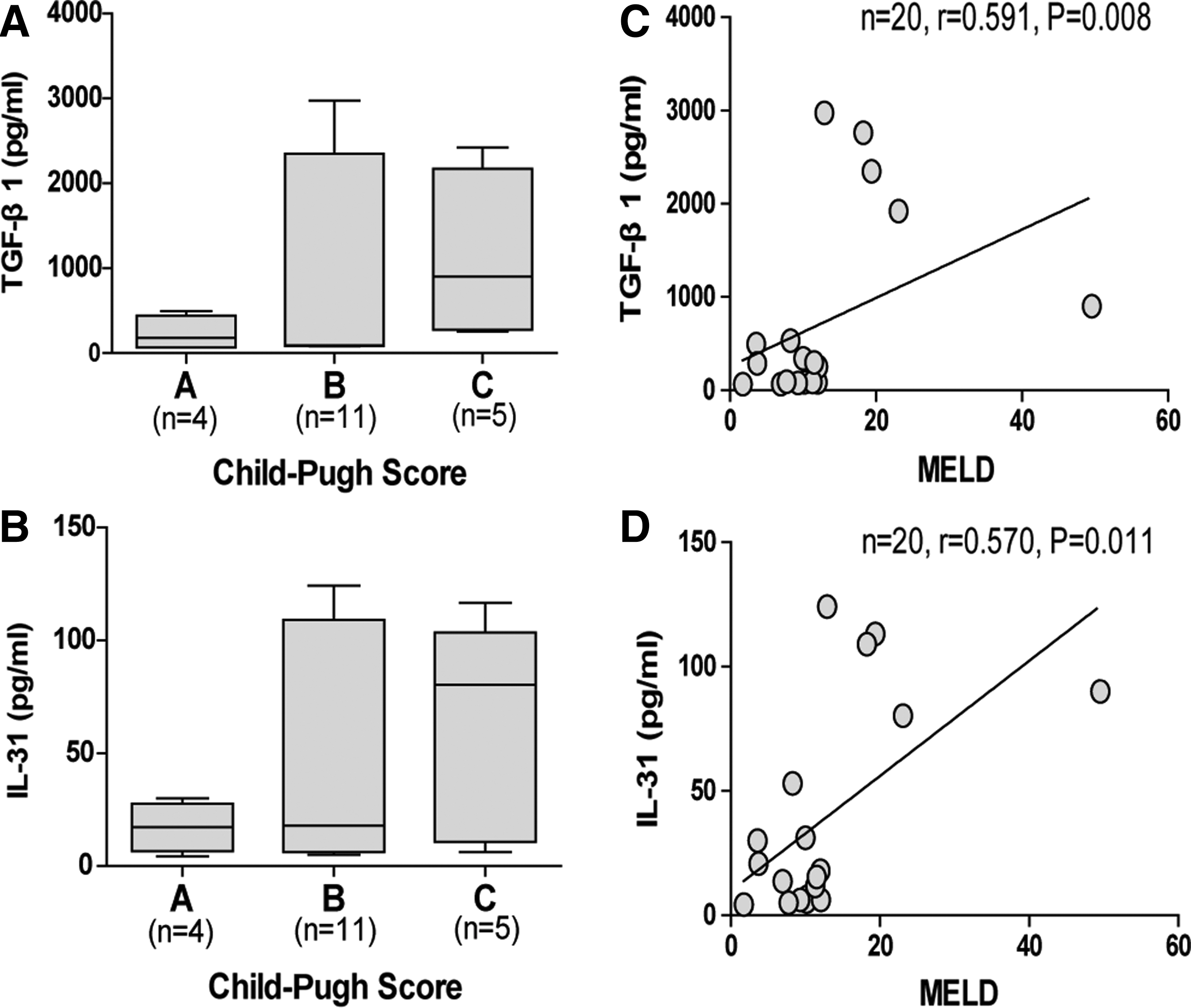
Increased levels of TGF-β1 and IL-31 positively correlated with disease severity. TGF-β1 and IL-31 levels in patients with different Child–Pugh stage (
Serum TGF-β1/IL-31 levels were altered in HBV-LC patients with liver decompensation
Complications of LC such as hypersplenism, esophageal varices, ascites, and infection indicate decompensated liver functions. The serum levels of TGF-β1 and IL-31 in patients with varices (89.7 [63.6–1920.3] pg/mL and 9.0 [4.3–80.3] pg/mL, respectively) were significantly higher than in patients without varices (716.2 [92.9–2974.7] pg/mL; 71.6 [7.5–124.2] pg/mL; p=0.016 and 0.007; Fig. 3E). However, the TGF-β1 and IL-31 levels in patients who had ascites, infection, or hypersplenism did not differ from those without these complications (p=0.822 and 0.545 for ascites; p=0.458 and 0.248 for infection; p=0.409 and 0.868 for hypersplenism; Fig. 3A, B, and D).
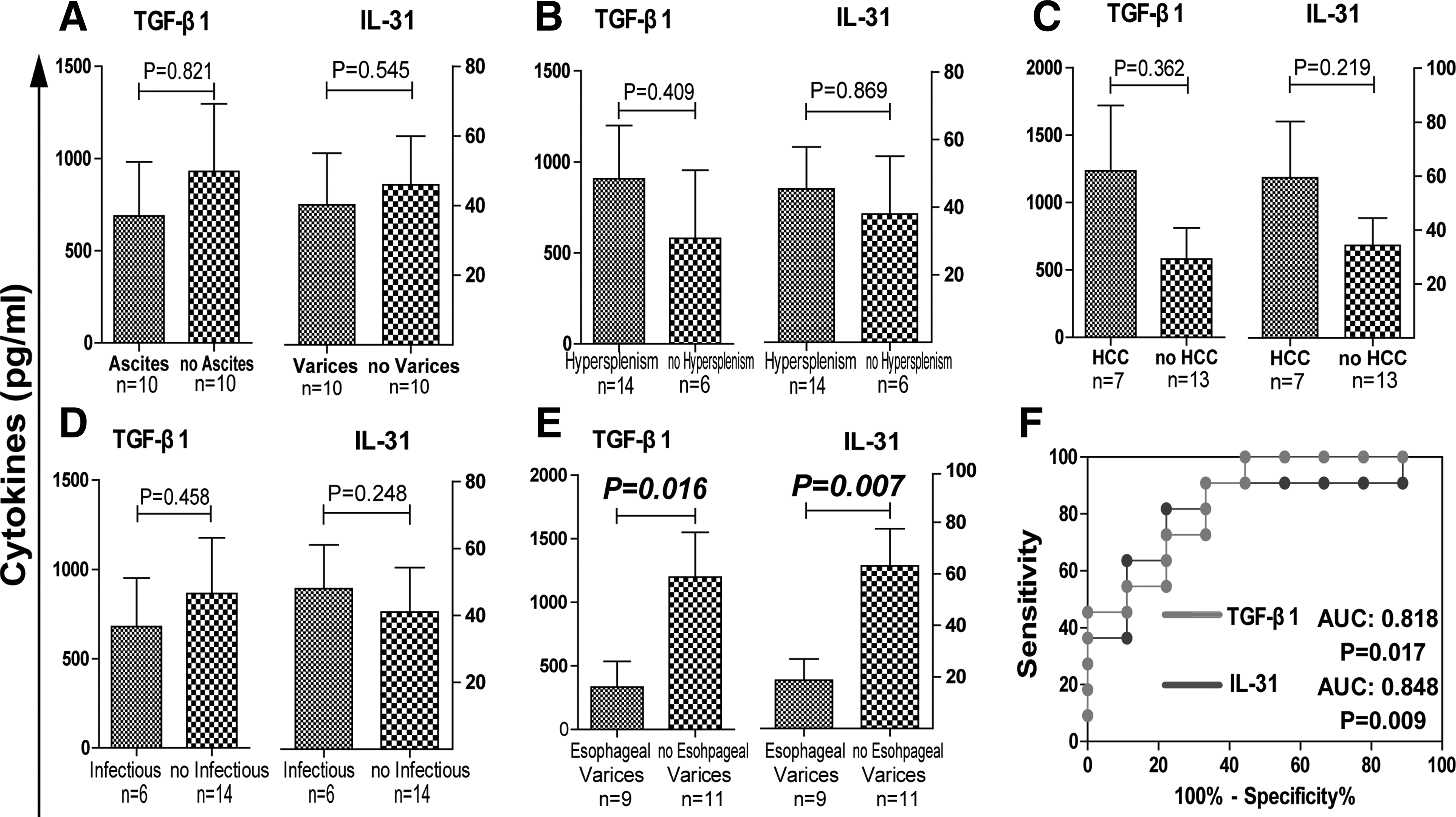
Serum levels of TGF-β1 and IL-31 between patients with and without complications. TGF-β1 and IL-31 levels in patients who suffered from ascites (
The TGF-β1 and IL-31 levels in patients with HCC (195.6[63.7–1920.3] and 16.7[4.3–90.1], respectively) were comparable to patients without HCC (1298.9[86.7–2974.7] and 62.5[6.3–124.2]; p=0.362 and 0.219; Fig. 3C).
To explore the ability of TGF-β1 and IL-31 to differentiate patients with esophageal varices from ones without this complication, a ROC analysis was performed. The areas under the curves of TGF-β1 and IL-31 were 0.818 and 0.848, respectively. IL-31 had the higher sensitivity (90.9%) and specificity (66.7%) in correlating the absence of esophageal varices in HBV-LC patients, with a cutoff value of 12.8 (Fig. 3F). This suggests that regular monitoring of IL-31 levels may predict the likelihood of varices, a dangerous complication with high mortality rates in cirrhotic patients.
Links between the TGF-β1/IL-31 pathway and other cytokines
The serum TGF-β1 levels strongly correlated with the IL-31 levels (r=0.953, p<0.001; Fig. 4A). In all subjects (n=57), both the TGF-β1 and IL-31 levels correlated with IL-22 (r=0.442 and 0.537, p<0.01; Fig. 4B and C) and IL-33 (r=0.482 and 0.459, p<0.001; Fig. 4D and E). However, they did not correlate with IL-9 (r=0.157 and 0.122, p>0.05), IL-10 (r=0.130 and 0.099, p>0.05), IL-23 (r=0.220 and 0.186, p>0.05), or IL-35 (r=0.231 and 0.213, p>0.05). Moreover, in the NC and CHB groups (n=37), the TGF-β1 and IL-31 levels correlated with IL-17 (r=0.349 and 0.350; p<0.05; Fig. 4F and G).
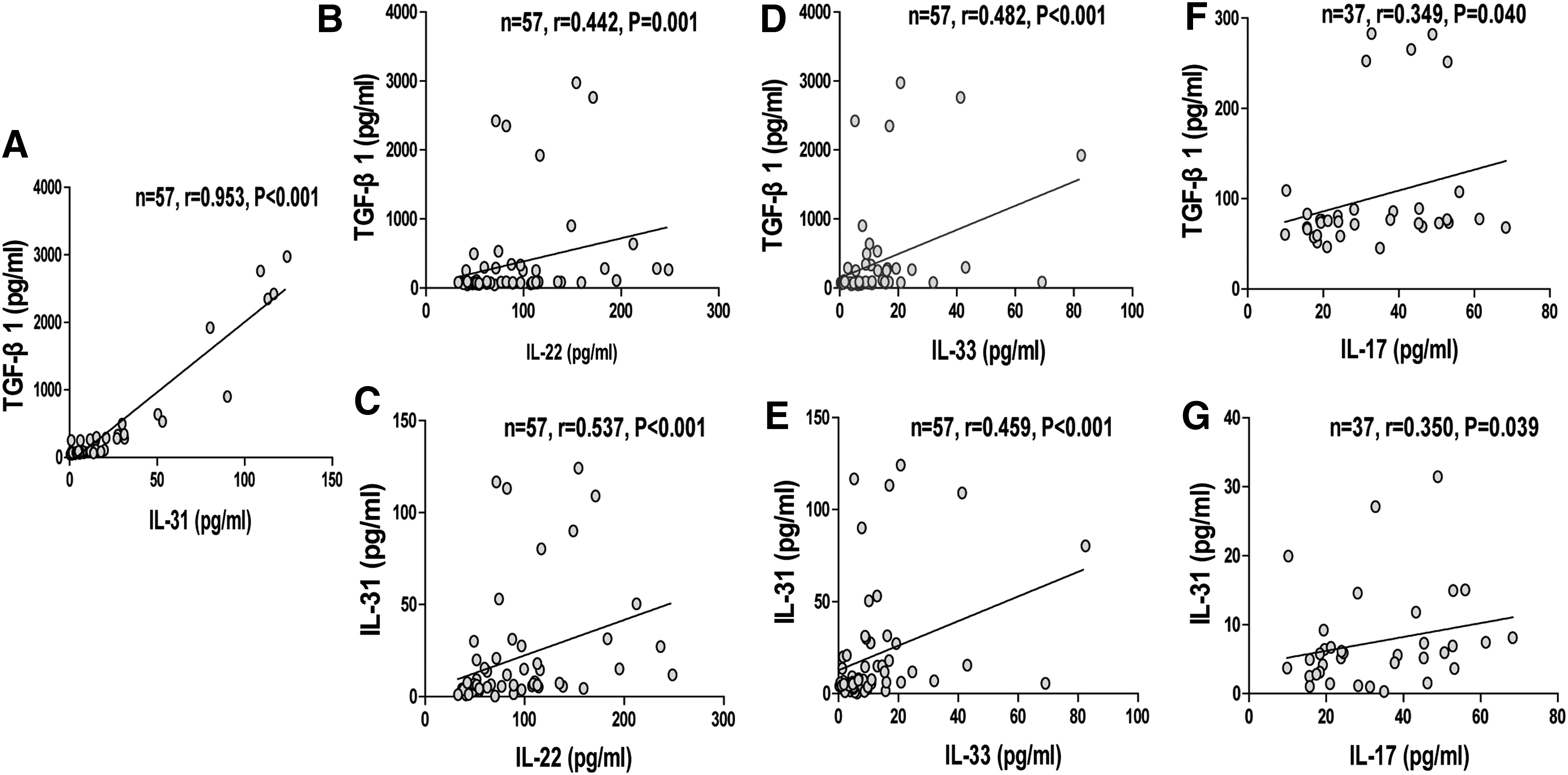
Associations between the TGF-β1/IL-31 pathway and other cytokines. Spearman's rank correlation was performed between variables. (
Discussion
Chronic liver injury and ongoing inflammation of the liver are the fundamental triggers that induce production of excessive extracellular matrix, forming fibrotic tissue toward the repair of damaged parenchyma. Elements that participate in the necroinflammatory process should be investigated for their role in contributing to fibrogenesis. TGF-β1 has been shown to have multiple biologic functions, depending on the target cells it binds. It can act on CD4+ T-cells to stimulate the production of IL-31, which is proinflammatory (25), and it can also activate hepatic stellate cells to produce extracellular matrix. There is evidence that the activated TGF-β1/IL-31 pathway is involved in the progression of bleomycin-induced pulmonary fibrosis in mice (17,25), suggesting the possibility of TGF-β1/IL-31 involvement in human LC.
The purpose of the present study was to determine whether TGF-β1/IL-31 levels were indeed altered in LC. For the first time, it was found that the TGF-β1/IL-31 pathway is closely associated with the progression of CHB to LC, and correlated with disease severity and the complications of HBV-LC. In addition, elevated TGF-β1 and IL-31 levels were sufficiently sensitive and specific for correlating the absence of esophageal varices within HBV-LC patients.
Details of the pathogenesis of liver fibrosis in HBV-LC remain unclear. An important feature of fibrosis is concomitant chronic liver damage and inflammation. While fibrosis functions to repair damaged liver cells, it can also lead to excessive production of extracellular matrix. Thus, the immunity-based theory may explain pathogenic fibrosis and hepatic malfunction. Previous studies have shown that Kupffer cells (34), monocytes, natural killer cells (33), dendritic cells (31), hepatic stellate cells, Th1 cells (34), Th17 cells (29,30), regulatory T-cells (24), and other immunologically relevant cells are involved in pathological liver fibrosis in HBV-LC. Increases in regulatory T-cells, monocytes, and other cells in the liver lead to higher levels of TGF-β1. Elevated TGF-β1 levels can induce Smad2 phosphorylation, activate the binding of Smad3 to IL-31 promoters, and finally stimulate the production of IL-31 (17), which promotes inflammatory responses (19). Therefore, it was hypothesized that both TGF-β1 and IL-31 participate in necroinflammation, which could further augment this pathologic process by activating factors that act to maintain the necroinflammation. This is consistent with the significantly increased TGF-β1 and IL-31 levels found in the present study in the serum of HBV-LC patients, and by the strong correlation between them.
It was also found that the serum levels of IL-22, IL-23, IL-33, and IL-35 were significantly higher in HBV-LC patients compared with the NC group, and serum levels of TGF-β1 and IL-31 correlated positively with IL-17, IL-22, and IL-33, all of which function as pro-inflammatory cytokines in HBV infection (23,30,32). These findings suggest that additional or downstream inflammatory cytokines can be activated or promoted by the TGF-β1/IL-31 pathway, leading to chronic liver injury and inflammation in HBV-LC. Therefore, the roles of the TGF-β1/IL-31 pathway in liver fibrosis include direct inflammation and modulating the expression of other inflammatory cytokines through innate and adaptive immune cells.
It seems that TGF-β1/IL-31 in hepatic fibrosis may function to sustain the pathologic process, since increased TGF-β1 and IL-31 levels, and that of other inflammatory cytokines, can augment and extend hepatic inflammation. This in turn can stimulate and attract additional inflammatory cells, releasing more cytokines. Such a cyclic process may extend the disease process in the liver, eventually cause the formation and accumulation of massive extracellular matrix, and result in distortion of the hepatic architecture.
TGF-β1 also delays regeneration of parenchymal hepatocytes, favors the differentiation of hepatic stellate cells in to cells that produce extracellular matrix, and promotes perisinusoidal fibrosis and hepatocyte apoptosis (27). The results of the present study thus suggest that modulation of the TGF-β1/IL-31 pathway may interrupt the pathologic process of HBV-LC, and benefit immunotherapy.
In this study, it was found that TGF-β1 and IL-31 negatively correlated with albumin. Albumin levels are an indication of the number of healthy hepatocytes, which synthesize and secret albumin. Albumin levels decrease when the function of a cirrhotic liver deteriorates. The inverse correlation between elevated TGF-β1 and IL-31 levels and reduced albumin in the cirrhotic liver suggests a significant decrease in the number of functional hepatocytes, while the number of nonparenchymal cells, including those that produce TGF-β1 and IL-31, has been sustained. Inevitably, the LC becomes more severe. This explains why elevated TGF-β1 and IL-31 levels were found to be positively associated with MELD scores. The findings are consistent with reports that cytokines can aggravate disease progression (9,30,32,34).
Esophageal varices, one of three complications of portal hypertension, is the leading cause of upper gastrointestinal bleeding. Inexplicable correlations were found between altered TGF-β1/IL-31 levels and the presence of esophageal varices. Only a specific range of TGF-β1 and IL-31 levels suggested a high-risk for esophageal varices forming, while a higher or a lower level of TGF-β1 and IL-31 was an indication of no esophageal varices. IL-31 in particular showed the highest sensitivity and specificity (90.9% and 66.7%, respectively) for correlating the nonoccurrence of esophageal varices in HBV-LC patients, with a cutoff value of 12.77. Such predictive utility shown by TGF-β1 and IL-31 levels should be verified by a larger number of cases in future studies.
There are some limitations in this study. First, it was not possible to obtain liver biopsies from HBV-LC patients because of the absence of indications for liver biopsy. It is not known if elevated TGF-β1 and IL-31 levels in the serum resulted directly from increased production by liver cells. Second, the proportion of CD4+T-cells that express TGF-β1 and IL-31 in the blood was not determined because of the limited blood volume. In future research, the expression of TGF-β1 and IL-31 in liver biopsies will be determined, along with the prevalence of TGF-β1 and IL-31-secreting CD4+T-cells in peripheral blood.
In conclusion, this study showed that serum TGF-β1 levels strongly correlated with IL-31, TGF-β1 and IL-31 were elevated significantly in HBV-LC patients, and correlated with severity of LC and MELD scores. In addition, TGF-β1, and especially IL-31, showed both the highest area under the curve value, and the highest sensitivity and specificity for correlating the absence of esophageal varices within HBV-LC patients.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No. 81400625), the Natural Science Foundation of Fujian province (No. 2014J01392), the Fujian Medical University Research and Development Project (No. FZS13029Y), and the Fujian Provincial Health Bureau Youth Research Project (No. 2013-1-45). The authors are grateful for the assistance of all the medical staff for collecting clinical specimens in the Department of Infectious Diseases, First Hospital of Quanzhou Affiliated to Fujian Medical University.
Author Disclosure Statement
No competing financial interests exist.