
Abstract
The aim of this study was to assess the impact of genetic variants of oligoadenylate synthetase 1 (OAS1) single-nucleotide polymorphism (SNP) rs10774671 at the exon 7 splice acceptor site on liver fibrosis progression and hepatitis C virus (HCV) outcome in Egyptian HCV genotype 4 patients. In this study, 195 subjects were enrolled; 60 controls and 135 chronic HCV genotype 4 patients with different fibrosis grades. All subjects were genotyped for OAS1 SNP rs10774671 polymorphism by polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) analysis. There was an increasing trend of liver fibrosis progression as 52.9% GG, 73.6% GA, and 83.3% AA genotypes were detected in late fibrosis patients (p = 0.025). The AA genotype was higher in the late fibrosis group than in the early fibrosis group (83.3% vs. 16.7%) (p = 0.001). The A allele was significantly affecting the liver fibrosis progression rate, more than the G allele (p = 0.001). The multivariate analysis showed that the OAS1 GA and AA genotypes were independent factors associated with liver progression (p = 0.009, odds ratio [OR] 3.467, 95% confidence interval [CI] 1.273–7.584). In addition, the A allele was associated with liver fibrosis progression (p = 0.014, OR 2.525, 95% CI 1.157–4.545). The polymorphism at OAS1 exon 7 rs3741981 might be a potential genetic marker and can be useful in the assessment of liver fibrosis progression and disease outcome in HCV-infected patients.
Introduction
H
Several studies showed that men tend to progress to fibrosis and cirrhosis faster than women. HCV patients over 40 years old progress to cirrhosis at a faster rate than younger patients. In HCV patients coinfected with HIV or hepatitis B virus (HBV) or having any comorbid conditions, high liver damage and progression rates were reported (1,6,35).
The immune responses to HCV are mainly responsible for viral clearance and disease pathogenesis during infection. Host genetic differences such as single-nucleotide polymorphisms (SNPs) in cytokines or interferon (IFN)-induced genes have a relevant influence on HCV susceptibility, disease progression, and treatment response (2,16,17,31). Many SNPs in cytokine genes, such as transforming growth factor (TGF)-β, IFN-γ, tumor necrosis factor (TNF)-α, the interleukin (IL)-1 receptor antagonist, IL-10, and IL-30, have been associated with several inflammatory conditions, hepatic fibrosis, and HCC (28,31,36,37). In addition, polymorphism in type III IFN class IL-29 (IFN-λ1), IL-28A, (IFN-λ2), and IL 28B (IFN-λ3) was associated with HCV liver progression and treatment response rates (8,11,32).
Genetic polymorphisms of IFN-induced genes were shown to influence the outcome of HCV infection (2,7,21). The 2′-5′-oligoadenylate synthetase 1 (OAS1) gene is one of the most important innate immunity genes, which defends against HCV infection and controls the disease progression. The 2′,5′-OAS enzyme uses adenosine triphosphate to synthesize 2′,5′-oligoadenylates. This leads to the activation of latent ribonuclease, which degrades the viral RNA and inhibits the virus replication. In humans, there is only one copy of the OAS1 gene on chromosome 12q24.2, but alternative splicing gives rise to several isoforms with different sizes and activities, such as the p42, p44, p46, p48, and p52 forms. The OAS1 gene contains eight exons and all the splice variant isoforms have exons 1–5, but vary with regard to downstream exons (5,24,27).
Different studies showed that the basal OAS activity is under strong genetic control and different SNPs produce isoforms with diverse enzyme activities. More than 12 SNPs in OAS1 were reported to affect the OAS enzyme activity and were associated with host susceptibility to many viral infections (5,15,25). The OAS1 exon 3 SNP rs3741981 was related to susceptibility to coronavirus infection and development of severe acute respiratory syndrome (15), while the OAS1 SNP rs34137742 was associated with West Nile virus (WNV) infection (4). The most important is the A/G SNP at OAS1 exon 7 splice acceptor site (SAS) rs10774671, which was shown to alter the splicing of the OAS1 gene. In this polymorphism, the G allele generates the active p46 enzyme isoform, whereas the A allele changes the splice site and generates p48 and p52 isoforms.
Several studies proved that the basal 2′,5′-OAS activity is higher in persons carrying the G (p46) allele than in those having only the A (p48/p52) allele. Genetic polymorphism at OAS1 exon 7 SAS was proved to significantly influence the host susceptibility to viral infection (5). Recently, it was reported that the OAS1 SNP rs10774671 at exon 7 SAS was associated with response to IFN treatment in HCV-infected patients (7,18).
There is a need for further research on the risk factors that affect liver progression and lead to fibrosis, cirrhosis, and HCC in HCV-infected patients. The detection of the host factor contributing to HCV pathogenesis and liver progression will help to understand host–virus relationships and to improve the control of HCV infection. HCV in Egypt is a public health problem with a prevalence rate of 14.7% and most of the patients are infected with HCV genotype 4 (29). Nevertheless, few studies were done on Egyptian genetic factors that affect the natural course of HCV genotype 4. So, in this study, we investigated the OAS1 SNP rs10774671 at exon 7 SAS in 195 Egyptian subjects; 60 healthy controls and 135 HCV genotype 4 patients with different fibrosis grades to assess the impact of this OAS1 SNP on liver fibrosis progression and HCV outcome.
Materials and Methods
Subjects
One hundred ninety-five subjects were enrolled in this study, 135 with proven chronic hepatitis C who did not receive any treatment and 60 healthy controls (negative for HCV Ab and RNA, as well as hepatitis B surface antigen HBsAg). All subjects were Egyptians and unrelated to each other. All HCV patients were clinically investigated at the Department of Tropical Medicine, Kasr El Ainy Hospital, Cairo University. Blood samples were collected with the appropriate institution ethics review board permission according to the Helsinki Declaration 1975 revised in 2008. All enrolled patients were positive for both anti-HCV antibody and HCV RNA and none of them had evidence of metabolic liver diseases, autoimmune, drug- or alcohol-induced hepatitis, hypo- or hyper thyroidism, or active schistosomiasis. The liver biopsy was carried out for histopathological examination and assessment of the liver fibrosis stages according to the Metavir Score (3).
Nested and real-time polymerase chain reaction of HCV
The RNA was extracted using the QIAamp Viral RNA Mini Kit (Qiagen, Hilden, Germany) to determine the presence of HCV RNA in serum. The HCV viremia was detected by reverse transcription polymerase chain reaction (RT-PCR) using nested primers derived from the highly conserved HCV 5′ untranslated region (UTR), as previously described (9,10), and real-time polymerase chain reaction (PCR) using the Artus HCV RT-PCR kit (Qiagen), according to the manufacturer's instructions. All patients were infected with HCV genotype 4a, as detected by INNO-LiPA HCV (Innogenetics, Ghent, Belgium).
Amplification of OAS1 exon 7 SNP rs10774671 region by PCR
Genomic DNA was extracted from the peripheral blood mononuclear cells of all subjects using the QIAamp DNA Mini Kit (Qiagen), according to the manufacturer's instructions. Then, the OAS1 exon 7 SNP rs10774671 was amplified by PCR using the primers designed by El Awady et al. (7). These primers cover exon 7 AG splice acceptor site region and produced a 203 bp PCR fragment. The PCR amplification was carried out in 25 μL, containing 100–500 ng DNA, 2.5 mM MgCl2 (Promega, Madison, WI), 500 nM of each primer, 200 μM dNTPs (Promega), 1× PCR buffer (Promega), and 1 U Go Taq DNA polymerase (Promega). Thermal cycling in an MJ Research cycler included denaturation at 94°C for 5 min, followed by 35 cycles each of denaturation at 94°C for 30 s; annealing at 58°C for 30 s; and extension at 72°C for 1 min. Cycling was followed by a final extension step at 72°C for 10 min. Primer sequences were as follows: OAS1 forward primer 5′-tgcaatgcaggaagactcc-3′ and OAS1 reverse primer 5′-tgcaggtccagtcctcttct-3′.
Determination of OAS1 exon 7 SNP rs10774671 by restriction fragment length polymorphism
A restriction fragment length polymorphism (RFLP) analysis was previously constructed for detection of AG allelic nucleotides at OAS1 SNP rs10774671 at exon 7 SAS region by El Awady et al. (7). The 203 bp long PCR fragments from all subjects were digested with AluI (Promega). The digestion reaction was carried out in a total volume of 20 μL containing 1× restriction buffer, 8 μL of the PCR product, and 5 U of AluI, according to the manufacturer's recommendations. The AluI restriction digestion was performed at 37°C for 4 h. Then, 10 μL of the digested products was run on a 2% of agarose gel stained with ethidium bromide.
Statistical analyses
Data are expressed as mean ± SD or number percent (%). Comparison between mean values of different parameters was performed using analysis of variance and t-test. Comparison between different OAS genotypes (GG, GA, and AA) or OAS alleles (G and A) in control and chronic patients with different fibrotic stages was performed using the chi-squared test. Then, univariate and multivariate logistic regression analyses were used to identify predictors associated with degree of fibrosis in chronic HCV patients. All statistical analyses were performed using the SPSS statistical software program (version 19 windows). The odds ratio (OR) and 95% confidence interval (CI) were calculated to assess the relative risk confidence. The data were considered significant if p-values were <0.05 and highly significant if p < 0.01. The statistical analysis determined the degree at which the OAS1 SNP rs10774671 can influence liver progression in HCV-infected patients.
Results
The clinical data of chronic HCV-infected patients
One hundred thirty-five chronic HCV-infected patients were categorized into three groups based on the degree of fibrosis: early fibrosis (F0–F1, n = 45), mild fibrosis (F2–F3, n = 45), and advanced fibrosis (F4, n = 45). The clinical data of all chronic HCV patients are expressed as mean ± SD and summarized in Table 1.
The statistical analysis of all clinical data of the early, mild, and advanced fibrosis patients showed that the alanine transaminase (ALT) level was higher in the advanced fibrosis patients than in mild or early fibrosis patients (p = 0.05), while age, total bilirubin, and alpha fetoprotein (AFP) levels were significantly higher in advanced fibrosis patients (p < 0.001). In contrast, the albumin level was significantly lower in advanced fibrosis patients (p < 0.001).
p-Value is significant when p ≤ 0.05 and highly significant if p < 0.01.
BMI, body–mass index; HCV, hepatitis C virus.
Distribution of different OAS1 SNP rs10774671 genotypes in controls and chronic HCV patients
The presence of homozygote GG genotype was indicated by the presence of 203 bp PCR fragment, intact, while the presence of homozygote (AA) genotype at the exon 7 SAS was indicated by AluI digestion of the 203 bp into two fragments of 150 and 53 bp. In cases of heterozygosity (AG), three fragments of 203, 150, and 53 bp appeared on agarose gel electrophoresis. The distribution of different OAS genotypes and allele frequencies in both healthy controls and chronic HCV patients is summarized in Table 2. The OAS genotypes in the control group were 51.7% GG, 40% GA, and 8.3% AA. The results indicated that the G allele tends to be more frequent than the A allele in both control (71.7% vs. 28.3%) and HCV-infected patients (64.4% vs. 35.6%). In all chronic HCV patients, genotype GG is slightly less than in controls without a statistically significant difference (37.8% vs. 51.7%).
OAS1, oligoadenylate synthetase 1; SNP, single-nucleotide polymorphisms.
In early fibrosis HCV patients, 53.3% were GG, 42.2% were GA, and 4.4% were AA genotypes. The distribution of different OAS genotypes in early, mild, and advanced fibrosis HCV patients is shown in Figure 1. The OAS GG genotype was 47% in early fibrosis, 31.4% in mild fibrosis, and 21.6% in advanced fibrosis, while the AA genotype was 16.6% in early fibrosis and 41.7% in both mild and advanced fibrosis. The distribution of different OAS alleles in early, mild, and advanced fibrosis HCV patients is shown in Figure 2. In early fibrosis HCV patients, the OAS G allele is higher than the A allele (74.4% vs. 25.6%, respectively) with a statistically significant difference (p = 0.001).

The distribution of oligoadenylate synthetase 1 (OAS1) single-nucleotide polymorphism (SNP) rs10774671 genotypes in early (F0–F1), mild (F2–F3), and advanced fibrosis (F4) hepatitis C virus (HCV) genotype 4 patients. One hundred thirty-five chronic HCV patients were subjected to polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) analysis to detect OAS1 SNP rs10774671. The percent of GG, GA, and AA genotypes was compared in the early fibrosis group (F0–F1, n = 45), (white bar), mild fibrosis group (F2–F3, n = 45) (hatched bar), and advanced fibrosis group (F4, n = 45) (black bar).
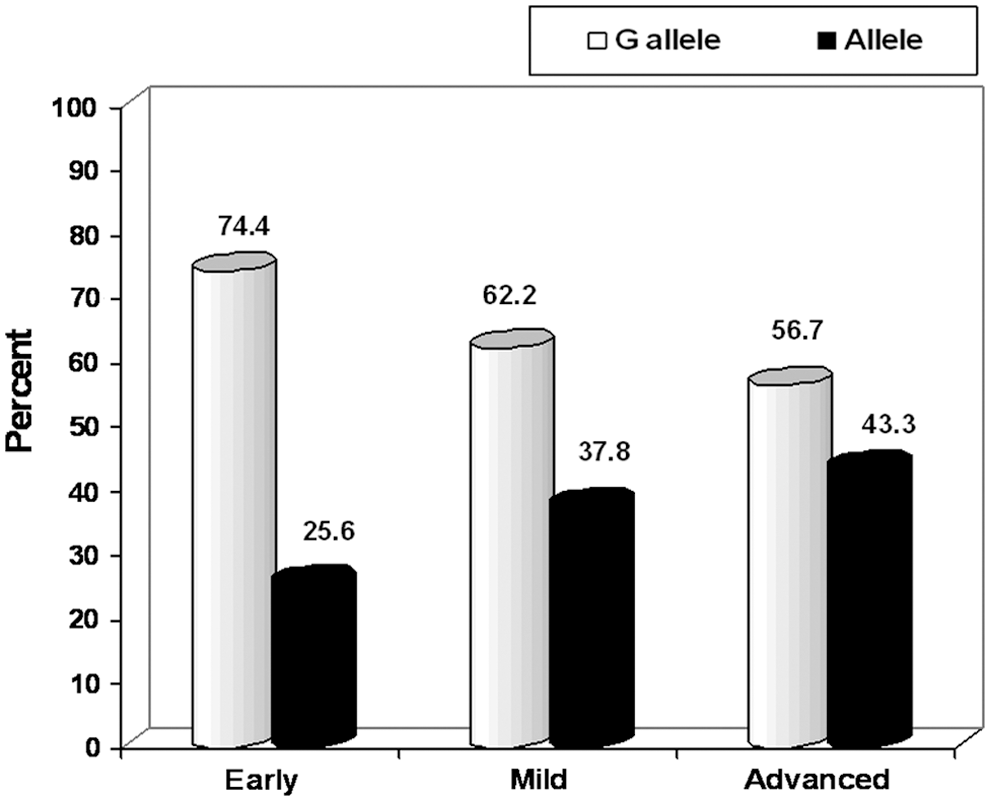
The frequency of OAS1 SNP rs10774671 alleles in early fibrosis (F0–F1), mild (F2–F3), and advanced fibrosis (F4) HCV genotype 4 patients. Frequencies of the G allele (white bar) and A allele (black bar) were calculated using the chi-square statistical test and presented in the early fibrosis group (F0–F1, n = 45), mild fibrosis group (F2–F3, n = 45), and advanced fibrosis group (F4, n = 45).
Influence of OAS1 SNP rs10774671 genotypes on biochemistry parameters and liver fibrosis progression
To evaluate the effect of OAS genotypes on the biochemistry parameters and liver fibrosis progression, the chronic HCV patients were categorized into two groups; the early fibrosis group (F0–F1, n = 45) and late fibrosis group (F2–F4, n = 90). The influence of different OAS genotypes on the biochemistry parameters is summarized in Table 3. The chi-square statistical test showed that OAS GG genotype patients have a significantly lower level of alanine transaminase (ALT), total bilirubin, and alpha fetoprotein (AFP) than GA+AA patients (p = 0.04, 0.004, 0.001, respectively). The early fibrosis patients showed a trend of having the G allele more than A allele as 47.1% of GG genotype, 26.4% of AG genotype, and 16.7% of AA genotype were detected in them (p = 0.025) as shown in Table 4. On the other, there was an increasing trend of liver fibrosis progression as 52.9% GG, 73.6% GA, and 83.3% AA genotypes were detected in late fibrosis patients (p = 0.025). Figure 3 showed that the AA genotype in the late fibrosis group was statistically significantly different than in the early fibrosis group (83.3% vs. 16.7%, p = 0.001). The late fibrosis patients had a higher frequency of the A allele (76.0%) compared with the early fibrosis patients (24.0%) with a statistically significant difference (p = 0.001).
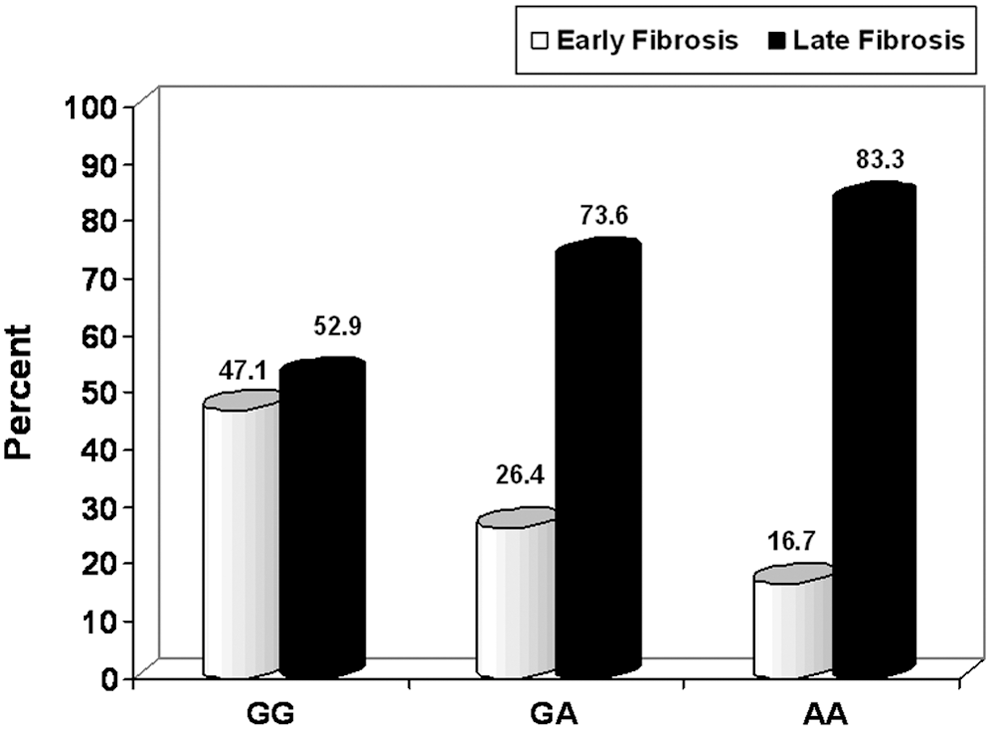
The distribution of OAS1 SNP rs10774671 genotypes in early fibrosis (F0–F1) and late fibrosis (F2–F4) HCV genotype 4 patients. Different OAS1 SNP rs10774671 genotypes (GG, GA, AA) were compared using the chi-square statistical test in the early fibrosis group (F0–F1, n = 45) (white bar) and late fibrosis group (F2–F4, n = 90) (black bar).
The chi-square statistical test was used to determine the influence of different OAS1 SNP rs10774671 genotypes (GG, GA, and AA) on the biochemistry parameters such as ALT, total bilirubin, albumin, and AFP.
p-Value is significant when p ≤ 0.05 and highly significant if p < 0.01.
p ≤ 0.05.
p < 0.01.
The distribution of OAS1 SNP rs10774671 genotypes and alleles was statistically analyzed in early and late fibrosis patients. The GA and AA genotypes were significantly higher in late fibrosis patients than in early fibrosis patients (p = 0.038, 0.001, respectively). In addition, the late fibrosis patients have the A allele more than G allele (p = 0.001).
p-Value is significant when p ≤ 0.05 and highly significant if p < 0.01.
p ≤ 0.05.
p < 0.01.
Univariate analysis of factors associated with liver fibrosis progression
To explore whether any of the clinical, biochemical, or virological parameters are associated with the liver progression pattern, a comparison between early fibrosis (F0–F1) and late fibrosis (F2–F4) groups is outlined in Table 5. The univariate analyses of all factors showed that there were no significant differences between early and late fibrosis groups in sex, body–mass index, and viral loads. On the other hand, age, ALT level, total bilirubin, and AFP levels were significantly higher in late fibrosis than early fibrosis patients as shown in Table 5. In addition, the distribution of OAS genotypes was statistically significantly different between early and late fibrosis groups (p = 0.008). Both early and late fibrosis groups have different frequency of OAS G and A allele (p = 0.015). The early fibrosis group had a higher frequency of the G allele (74.4%) than the A allele (25.6%) as shown in Figure 4.
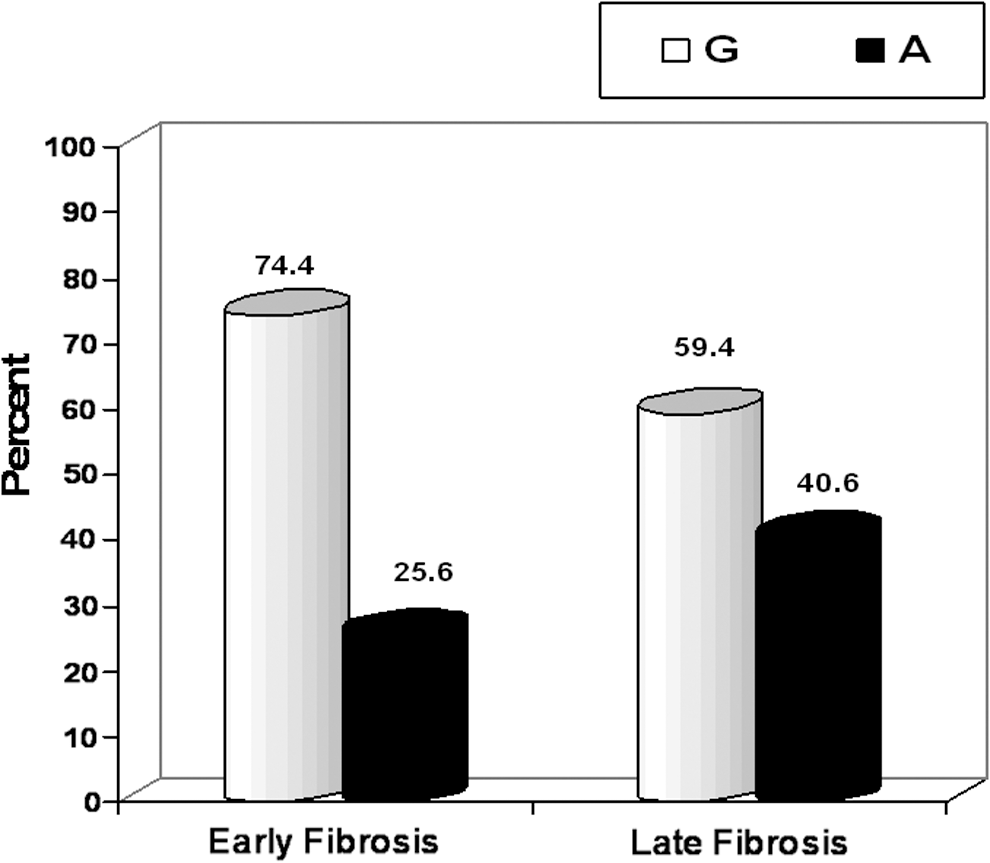
The frequency of OAS1 SNP rs10774671 alleles in early fibrosis (F0–F1) and late fibrosis (F2–F4) HCV genotype 4 patients. The chi-square statistical test was used to compare the frequencies of the G allele (white bar) and A allele (black bar) in the early fibrosis group (F0–F1, n = 45) and late fibrosis group (F2–F4, n = 90).
The results showed a higher level of ALT, total bilirubin, and AFP in late fibrosis patients (p = 0.02, 0.001, and 0.001, respectively), while albumin levels were significantly lower in late fibrosis patients (p = 0.001). Moreover, the OAS1 rs10774671 genotypes and alleles showed a statistically significant difference in late than in early fibrosis patients (0.008, 0.015, respectively).
p-Value is significant when p ≤ 0.05 and highly significant if p < 0.01.
p ≤ 0.05.
p < 0.01.
Multivariate analysis of predictive factors for liver fibrosis progression in chronic HCV patients
The significance of several host factors in determining the progression of liver disease in chronic HCV patients was investigated by stepwise logistic regression analysis. ALT level, total bilirubin, albumin, AFP, different OAS genotypes, and alleles independently and significantly influenced the outcome of liver progression. HCV patients with higher ALT level, total bilirubin, and AFP had a significantly higher liver progression than those with the normal level as shown in Table 6. On the other hand, GA and AA genotypes at OAS1 exon 7 SNP rs10774671 increased the risk of liver fibrosis than those with GG genotype (p = 0.009, OR 3.46, 95% CI 1.273–7.584). In addition, the A allele increased the risk of liver fibrosis than those with the G allele (p = 0.014, OR 2.5, 95% CI 1.157–3.545).
The effects of several factors such as ALT, total bilirubin, albumin, AFP, different OAS1 rs10774671 genotypes, and alleles in determining liver progression were investigated.
p-Value is significant when p ≤ 0.05 and highly significant if p < 0.01.
p ≤ 0.05.
p < 0.01.
Discussion
The immune responses to HCV are mainly responsible for viral clearance and the disease pathogenesis during infection. Host genetic factors concerning innate immunity, specially IFN-induced genes, affect the suppression of HCV and relate to chronic infection, inflammation activity, and liver disease progression (16,22,31). Several SNPs in MxA, OAS, PKR, IL1B, and IL28B genes were reported to alter gene expression and/or gene function and therefore influenced the HCV disease outcome and the treatment response (17,21).
The OAS1 gene codes for antiviral OAS enzyme and its role in fighting and controlling different viral infections has been documented in several studies (15,25,26). The SNP at exon 7 SAS of OAS1 rs10774671 has been documented to be a functional SNP, which affects the OAS antiviral activity. So, in this study, we evaluated if the genetic OAS1 SNP rs10774671 at the exon 7 SAS is associated with liver disease progression and HCV infection outcome. The results of this study showed that OAS GG genotype is higher in control (51.7%) than in HCV-infected patients (37.8%). The G allele is more frequent than the A allele in both control and HCV-infected patients. In addition, there was an increasing trend of the A allele frequency (24.6%, 37.8%, and 43.3%) in early, mild, and advanced fibrosis HCV patients, respectively.
These results supported the previous study of Ghosh et al. (13) who revealed that OAS1 exon 7 SAS SNP produces by alternative splicing of different OAS isoforms with different antiviral activities. Therefore, the low enzyme activity p48, which is produced in patients with GA or AA genotypes fails to suppress HCV replication and subsequently leads to severe inflammation and promotes liver fibrosis. In addition, the present study findings are in agreement with Kjær et al. (20) who documented that OAS1 SNP rs10774671 leads to differentially expressed OAS1 isoforms in three human cell lines, nonetheless, in contrast to Bonnevie-Nielsen et al. (5) who found that type 1 diabetes patients have higher frequencies of genotypes GG and GA at OAS1 exon 7 SNP rs10774671 than in control subject.
The OAS1 SNP rs10774671 has been associated with type 1 diabetes (34) and multiple sclerosis (12). The A allele at OAS1 SNP rs10774671 is considered a risk factor for WNV initial infection (25). Recently, the OAS1 SNP rs10774671 was evaluated in human bronchial epithelial cells and shown to have a potential role in the respiratory infection (30). However, little is known about the effect of this functional OAS1 SNP rs10774671 in HCV-infected patients. Only El Awady et al. (7) and Imran et al. (18) showed a significant association between the OAS1 exon 7 SNP rs10774671 and the IFN response rate in chronic HCV patients. Till now, there are no reports on the effect of OAS1 exon 7 SNP rs10774671 on liver fibrosis progression in HCV-infected patients. Therefore, we categorized the 135 HCV patients into 45 early fibrosis (F0–F1) patients and 90 late fibrosis (F2–F4) patients to study the effect of different OAS1 SNP rs10774671 genotypes and alleles on liver fibrosis progression.
The results showed that OAS GG genotype patients have a significantly lower level of ALT, total bilirubin, and AFP than GA+AA patients. In addition, there was an increasing trend of liver fibrosis progression as 52.9% GG, 73.6% GA, and 83.3% AA genotypes were detected in late fibrosis patients (p = 0.025). The late fibrosis patients have significantly higher GA and AA genotypes than early fibrosis patients (70.0% vs. 46.7%, respectively) (p = 0.008).
On the other hand, the comparison of OAS alleles in early and late fibrosis groups revealed that the early fibrosis patients have the G allele (74.4%) more than A allele (25.6) (p = 0.015). The results showed a clear association between liver disease progression and allele A containing genotypes (GA and AA) (p = 0.008) or A allele (p = 0.015). These results are similar to the findings of Li et al. (24) who reported that the G allele at OAS1 exon 3 SNP rs3741981 has an inefficient ability than the A allele to suppress HCV replication and is associated with a higher degree of liver fibrosis and cirrhosis in Japanese HCV patients. Moreover, Knapp et al. (21) found that OAS1 SNP in the 3′ UTR was related to HCV outcome in Caucasian patients.
The multivariate logistic regression analysis showed that the OAS1 GA and AA genotypes were independent factors associated with liver progression (p = 0.009, OR 3.467, 95% CI 1.273–7.584). In addition, the A allele was an independent factor associated with liver fibrosis progression (p = 0.014, OR 2.525, 95% CI 1.157–4.545). Moreover, interaction between OAS1 genotype GG and the normal level of ALT, AFP, and total bilirubin showed a decrease in liver fibrosis progression (p = 0.048, OR 2.429, 95% CI 1.007–5.856). All the study results confirmed that OAS1 polymorphisms at exon 7 SAS are associated with liver fibrosis progression and determined the outcome in an HCV-infected patient.
Genetic biomarkers can be useful to monitor the degree of inflammation, disease progression, and treatment response in HCV-infected patients. Several genetic factors were associated with liver fibrosis progression in HCV patients (31). Recently, IL28B SNP rs12979860 was significantly associated with a higher activity of liver inflammation and severe liver fibrosis (11,33). Therefore, the polymorphism at exon 7 SAS in the OAS1 gene with other previously reported genetic factors might be a potential genetic marker and can be useful in the assessment of liver fibrosis progression and disease outcome in HCV-infected patients.
Footnotes
Authors' Contributions
N.G.B. designed, supervised the experiments, and wrote the article; M.A.A. performed all experiments and helped in writing the article; R.M.D., M.K.I., R.E., and Y.S.E. helped in sample collection and experiments; and M.K.E. financially supported and directed the study.
Acknowledgments
This work was partially funded through the Science and Technology Development Fund (STDF), Egypt, Grant No. 3365 to Dr. Mostafa El Awady. All authors are thankful to Dr. Gamal Esmat for referring the cases.
Author Disclosure Statement
No competing financial interests exist.