
Abstract
Melanoma differentiation-associated protein 5 (MDA5) and retinoic acid-inducible gene 1 (RIG-1) as the pattern recognition receptors play important roles in viral mRNA recognition. Chronic HBV-infected (CHB) patients are unable to properly respond to hepatitis B virus (HBV). Therefore, the aim of the present study was to evaluate the mRNA levels of MDA5 and RIG-1 in the peripheral blood immune cells of CHB patients in comparison to healthy controls. In this cross-sectional study, the mRNA levels of MDA5 and RIG-1 were examined in 60 CHB patients and 60 healthy controls using the real-time polymerase chain reaction (PCR) technique. Our results showed that mRNA levels of MDA5 and RIG-1 were significantly decreased and increased, respectively, in CHB patients when compared to healthy controls. Our results also revealed that mRNA levels of MDA5 and RIG-1 were not altered among CHB patients with various states of e-antigen of hepatitis B and HBV-DNA viral loads. According to the results presented here, it may be concluded that downregulation of MDA5 may be a responsible mechanism from several reasons, which leads to HBV persistence in CHB patients.
Introduction
R
Materials and Methods
Subjects
An equal number of patients and controls (60 in each group) were recruited in this cross-sectioned study. Peripheral blood samples were collected from healthy controls and CHB patients from Rafsanjan city (south-east of Iran) in 5.5-mL tubes either anticoagulant coated or without an anticoagulant. CHB patients who had detectable measures of HIV and HCV antibodies as well as patients with infections caused by other types of viruses, such as Epstein–Barr virus, hepatitis A, C, D, E viruses, and cytomegalovirus, were all excluded from the study. The CHB was diagnosed with regard to the “Guide of Prevention and Treatment in Viral Hepatitis” by an expert internal medicine specialist. In summary, CHB patients had normal serum levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), direct bilirubin (DB), and total bilirubin (TB). All patients were hepatitis B surface antigen (HBsAg) positive for a period of more than 6 months. They were recruited to the study according to the evaluation of their previous clinical and experimental records. Control subjects were recalled with the same sex and age status. All patients with the following criteria were also excluded from the study: patients receiving therapy with immunosuppressive and interferon or antiviral medications before the biopsy, coexistence of CHB with other liver diseases, breastfeeding or pregnancy, cirrhosis, Wilson disease, having a history of liver transplantation, and/or exhibiting evidences for hepatocellular carcinomas (HCC). The samples collected with anticoagulant were instantly used for RNA extraction. The samples collected without an anticoagulant were also centrifuged at 3,500 rpm for 4 min, and the sera were collected and stored at −20°C for further liver enzymes and HBV-DNA assessments. The Ethics Committee of the Rafsanjan University of Medical Sciences has approved the protocol of this study, and a written informed consent was separately obtained from each patient or healthy control before sample collection.
Measurement of serological HBV markers
All of the samples were screened for the e-antigen of hepatitis B (HBeAg) and HBsAg using ELISA (enzyme-linked immunosorbent assay) (Behring, Marburg, Germany) according to the manufacturer's guidelines.
HBV-DNA extraction and real-time PCR condition
Viral DNA extraction and HBV-DNA quantification were performed using commercial kits from Cinnaclon (Tehran, Iran) and Design Primer (London, United Kingdom) companies according to the manufacturer's guidelines.
RNA extraction, reverse transcription, and quantitative real-time PCR
Methodology of total RNA purification, cDNA synthesize, and real-time polymerase chain reaction (PCR) protocol was described in our previous study (5). In real-time PCR, the β-actin (as housekeeping gene) was used for normalization of amplification signals of target genes. Sequences of the primers, which were used in this study, are presented in Table 1.
MDA5, melanoma differentiation-associated protein 5; RIG-1, retinoic acid-inducible gene 1; F, forward; R, reverse.
Liver function tests
To examine the serum levels of ALT, AST, ALP, DB, and TB, commercial kits from MAN Company (Tehran, Iran) were used.
Data analyses and statistical methods
The analyses were performed using t test and one-way analysis of variance under SPSS software version 18. A p-value less than 0.05 was considered significant.
Results
Detection of HBsAg, HBeAg, and HBV-DNA copy numbers
According to the fact that the CHB patients who evaluated in this study were the same as our previous study (14), hence, the results regarding the statuses of HBsAg, HBeAg, and HBV-DNA copy numbers/mL have been reported in our previous study. In brief, all of the studied patients were HBsAg positive, and only 16 (26.7%) of them were HBeAg positive. HBV-DNA was found in all patients, and 28, 14, and 18 patients were carrying <20,000, 20,000–100,000, and >100,000 HBV copy number/mL, respectively.
Serum levels of liver enzymes
Present results identified that all patients had normal serum levels of AST, ALT, ALP, DB, and TB (Table 2).
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CHB, chronic HBV-infected; HBV, hepatitis B virus.
Expression levels of target genes
Our results showed that expression of MDA5 in the PBMCs of CHB patients was 1/46-fold decreased in comparison to healthy controls (Fig. 1). Statistical analysis of findings demonstrated that the difference between groups regarding expression of MDA5 was significant (p = 0.047) (Fig. 1). These results also revealed that mRNA levels of RIG-1 in the PBMCs of CHB patients were −0/96 ± 0/22 in CHB patients and −2/17 ± 0/15 in healthy controls, where the difference was significant (p < 0.001) (Fig. 1). Our result also demonstrated that the expression levels of MDA5 were −1/4 ± 0.17 and −1/2 ± 0.27 in HBeAg-negative and HBeAg-positive CHB patients, respectively (Fig. 2). Statistical analysis of data showed that the difference was not significant (p = 0.652). The current result also revealed that expression levels of RIG-1 did not differ in HBeAg-negative and HBeAg-positive CHB patients (p = 0.369) (Fig. 2). Moreover, our results displayed that expression levels of MDA5 (p = 0.588) and RIG-1 (p = 0.99) did not differ between CHB patients with various HBV-DNA copy numbers (Fig. 3).

Expression levels of MDA5 and RIG-1 in CHB patients in comparison to healthy controls. The figure demonstrated that expression levels of MDA5, but not RIG-1, were significantly decreased in CHB patients in comparison to healthy controls. CHB, chronic HBV-infected; HBV, hepatitis B virus; MDA5, melanoma differentiation-associated protein 5; RIG-1, retinoic acid-inducible gene 1.
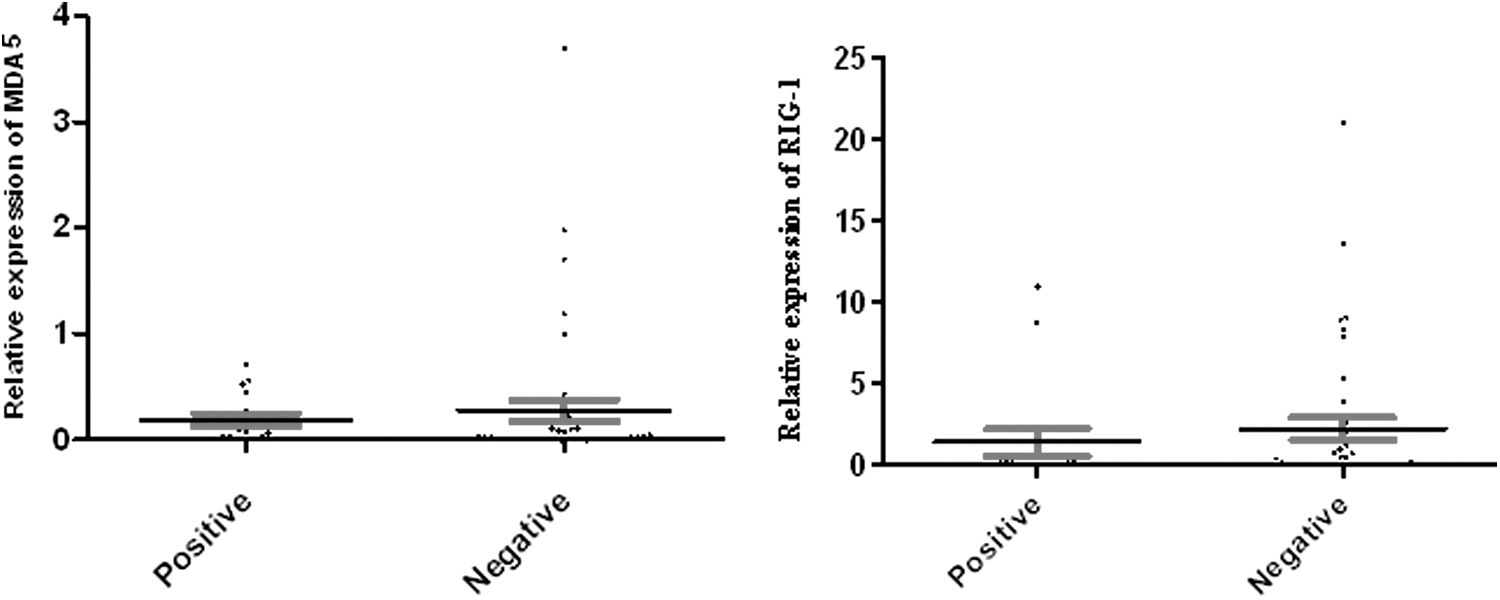
Relative expression of MDA5 and RIG-1 in HBeAg-positive and HBeAg-negative CHB patients. The results reveal that the mRNA levels of MDA5 and RIG-1 were not altered among HBeAg-positive and HBeAg-negative CHB patients. HBeAg, e-antigen of hepatitis B.

Relative expressions of MDA5 and RIG-1 in CHB patients with hepatitis B virus-DNA copy numbers/mL < 20,000 (A), between 20,000 and 100,000 (B) and >100,000 (C). The figure illustrates that expression levels of MDA5 and RIG-1 were not changed in CHB patients with various viral loads.
Discussion
Our results demonstrated that the expression levels of MDA5 were significantly decreased in CHB patients when compared to healthy controls. Concerning the fact that MDA5 plays important roles in viral PAMPs recognition (7,9), decreased expression of this molecule may result in impaired HBV recognition and consequently disrupted immune responses in CHB patients. These results also revealed that the mRNA levels of RIG-1 were significantly increased in CHB patients in comparison to healthy controls. Therefore, according to these results, it appears that CHB patients are unable to express MDA5, but not RIG-1, hence, HBV will be persistent in these patients. In a study, Lu and Liao reported that HBV replication in Huh7 cells and livers of mice hydrodynamically injected with the HBV replicative plasmid leads to increased expression of MDA5, but not RIG-I (11). The researchers also have cotransfected Huh7 cells with the RIG-I or MDA5 expression plasmid and demonstrated that MDA5, but not RIG-I, at a similar protein level, significantly suppressed HBV replication (11). Furthermore, it has been documented that HBV replication was increased as a result of knocking down of MDA5, but not RIG-I (11). Therefore, according to Lu and Liao, as well as our own findings, it seems that CHB patients fail to express adequate levels of MDA5 to recognize HBV-RNAs and further expression of proinflammatory cytokines. In addition, it is likely that HBV targets MDA5 and its associated signaling molecules to escape from innate immune responses. For instance, Wang et al. indicated that hepatitis B x (HBx) protein interacts with VISA, the adaptor protein for MDA5 signaling, and disrupts its association with upstream and downstream molecules (16). Wei et al. also showed that HBx interacted with VISA and increased the degradation of this molecule through ubiquitination at Lys(136) (17). Another study demonstrated that increased expression of IPS-1 suppresses the replication of hepatitis B in HepG2 or Huh7 Liver originated cells (8). Consistent with our results, Mozer-Lisewska et al. reported that expression levels of RIG-1 have not changed in the HBV-infected hepatocytes (15). Overall, based on aforementioned studies and our own study, it may possibly be concluded that MDA5, but not RIG-1, plays crucial roles in recognition of HBV and activation of appropriate immune responses. Therefore, it appears that further studies on MDA5 and its signaling molecules can improve our knowledge regarding the responsible mechanisms involved in impaired immune responses against HBV in CHB patients. Our results also showed that expression levels of MDA5 and RIG-1 were not significantly changed in HBeAg-positive in comparison to HBeAg-negative CHB patients (Fig. 2). Accordingly, HBeAg is associated with several complications of hepatitis B, including cirrhosis and HCC, hence, it seems that MDA5 may play a role in the pathogenesis of hepatitis B. Additionally, our results revealed that mRNA levels of MDA5 and RIG-1 were not altered in CHB patients with various HBV-DNA copy numbers (Fig. 3). Thus, it could be suggested that HBV replication is not associated with expression levels of MDA5 and RIG-1.
Finally, due to the current results, it may be concluded that decreased expression levels of MDA5, independent to HBV replication, confirmed the important roles played by the molecule and can be considered as a key candidate for recognition of HBV and activation of immune responses in CHB patients.
Footnotes
Acknowledgment
This project was supported by a grant from the Rafsanjan University of Medical Sciences.
Author Disclosure Statement
No competing financial interests exist.