
Abstract
Hepatitis B virus (HBV) prevalence has declined remarkably in children due to nationwide universal vaccination program for HBV in China. However, the persistence of immune response against HBV infection and the optimal time point when a booster vaccination should be performed remain to be elucidated. To assess the persistence and level of antibody against hepatitis B surface antigen (anti-HBs) in a representative population of age 15 and younger who received routine hepatitis B vaccination in Mianyang City, China. A cross-sectional study was conducted in 2011. One thousand five hundred twenty-six children of age 15 and younger who received three doses of 5 μg hepatitis B vaccine series during infancy but did not receive a booster vaccination later were enrolled. Of the 1,526 children, the mean age was 8.2 ± 4.1 and 739 children were male. The median anti-HBs level was 23.0 mIU/mL, and the total percentage of anti-HBs levels ≥10 mIU/mL was 60.9%. With an increase of age, median anti-HBs level, percentage of anti-HBs levels ≥10 mIU/mL, and percentage of anti-HBs levels ≥100 mIU/mL declined remarkably in the early period and reached the lowest level at the age of 3 and then remained relatively stable. The median anti-HBs level, the percentage of anti-HBs levels ≥10 mIU/mL, and the percentage of anti-HBs levels ≥100 mIU/mL in 1- and 2-year-old children were much higher than that in children aged 3–15 (p < 0.05, respectively). Immunity against HBV infection gradually decreased in early ages of children of 15 and younger who received three doses of 5 μg hepatitis B vaccine series during infancy in China. Three dosages of 10 μg hepatitis B vaccine for infants and repeated vaccination or additional booster vaccination for some children at or before age 3 should be provided to get much more powerful immunity to HBV.
Introduction
C
Although hepatitis B vaccine has been used for more than 20 years, HBV infection remains a serious global public health problem. Many countries have made great efforts to implement infant vaccination with hepatitis B vaccines. The Chinese Ministry of Health recommended hepatitis B vaccines for routine immunization of infants since 1992. Initially, parents instead of the government paid for the vaccine and they did not have to get their children vaccinated. Beginning at 2002, hepatitis B vaccination (5 μg/0.5 mL) was covered by the National Expanded Program on Immunization (EPI) in China (19,23). The hepatitis B vaccines have been provided and paid by the government, but the vaccine administration fees had to be paid by the parents. Since 2005, hepatitis B vaccination completely became a nationwide universal vaccination program (19,23). From 2009 to 2011, hepatitis B vaccines were freely provided to all children of 15 and younger nationwide, who did not receive the routine three doses of hepatitis B vaccination after birth.
Although hepatitis B vaccination coverage was higher in urban and high socioeconomic areas than that in rural and lower socioeconomic areas for a long time, hepatitis B infections have been declining throughout the country since 1992. The prevalence of hepatitis B surface antigens (HBsAg) for the Chinese population aged 1–59 decreased from 9.8% in 1992 to 7.2% in 2006 (19,23). The HBsAg prevalence has greatly diminished among children 15 and younger compared to that showed in the 1992 national serosurvey. Among children younger than 5, the HBsAg prevalence was only 1.0% (90% reduction) (19,23).
Reduced HBsAg prevalence was strongly associated with hepatitis B vaccination among all age groups. Conversely, the prevalence of antibody to hepatitis B surface antigen (anti-HBs) for population of age 1–59 increased from 27.4% in 1992 to 50.1% in 2006; for children between the age 1 and 4, it increased from 15.8% in 1992 to 72.3% in 2006 (19).
Although there has been a great success in reducing HBsAg prevalence and increasing anti-HBs prevalence, a relatively large number of children and adults showed anti-HBs negative. One study from Taiwan found that incomplete immunization was the most important risk predictor of the liver disease (8). Recently, vaccine breakthrough infections have been reported in blood donors, who were tested as HBV DNA positive (1,16,31,32), with histories of previous vaccination and low levels of vaccine-induced anti-HBs. Another study from India found that 5% of the undergraduate students who received the HBV vaccine as infants had isolated hepatitis B core antibodies (anti-HBc), and all the anti-HBc-positive subjects had detectable hepatitis B viral DNA in their serum with undetectable HBsAg (13). Several studies showed that a considerable proportion (27–50%) of fully vaccinated adolescents had lost both their T-cell memory and humoral immunity against HBsAg (9,20,37).
Although people with negative anti-HBs still have the risk of getting HBV infection and it is recommended for them to receive routine immunization or a booster vaccination, the appropriate time for the vaccination and the appropriate vaccination program still remain unclear.
To assess whether and when a further universal vaccination program is needed as a complementary for the universal hepatitis B vaccination program in China, the prevalence of anti-HBs levels was investigated in a representative population of 15 and younger in Mianyang City, a typical city in southwestern China, which was struck during the 7.8 magnitude Wenchuan earthquake in 2008.
Materials and Methods
Study design and participants
To assess the persistence of anti-HBs levels in a representative population of age 15 and younger, a cross-sectional study was conducted in 2011. Children of age 15 and younger who received routine hepatitis B vaccination in Fucheng district were enrolled. Fucheng district is in the west-central part of Mianyang city, which is located in northern Sichuan province and was selected as one of the representative areas in China in 2009 for controlling and preventing major infectious diseases, such as hepatitis B, active pulmonary tuberculosis, and acquired immune deficiency syndrome.
This study was planned to enroll 1,500 children with ∼300 of them in each age group. Children 2 and younger were from the communities, and children aged 3–15 were from the kindergartens, elementary schools, and junior high schools. Only those children who had received a complete primary hepatitis B vaccination during infancy were enrolled. All the children participated in this study voluntarily with informed consents from their parents. Only those children whose parents signed the agreements of investigation were enrolled in the study. The vaccination history was verified by the certifications of vaccination and was distributed to each newborn by the local Center of Diseases Control and Prevention (CDC), if available. Otherwise, the vaccination histories were verified by hepatitis B vaccination database recorded in the Fucheng CDC. Children who received additional booster vaccinations were excluded.
At last, 1,526 children were enrolled in this study. All the children were administered three standard doses of intramuscular injection of recombinant yeast hepatitis B vaccine (5 μg/0.5 mL) at birth and at the ages of 1 and 6 months. All the children did not receive additional booster vaccinations. The recombinant yeast hepatitis B vaccines received by every child were from different producers, whose hepatitis B vaccines were widely used in China. However, the brand names for those used vaccines were unavailable since long time past from the original vaccination.
Laboratory test
A two microliter blood sample was collected from each child. Serums were separated from these blood specimens, and anti-HBs levels were measured in the Clinical Laboratory of Mianyang Infectious Diseases Hospital, Mianang City, Sichuan, China. Serums anti-HBs levels were tested and quantified by the time-resolved immunofluorometric assay according to the instruction (Xinbo Biotechnology Limited Company, Suzhou, China). The detection range of this reagent was ≤960 mIU/mL.
Definition
It is generally considered that people with anti-HBs level ≥10 mIU/mL (responders) are protected against HBV infection by hepatitis B vaccination (24,30). People with a quantitative anti-HBs level <10 mIU/mL, 10–99 mIU/mL, or ≥100 mIU/mL are considered to be nonresponders, poor responders, or good responders, respectively (2). Of the good responders, people with a quantitative anti-HBs level in 100–999 mIU/mL or ≥1,000 mIU/mL are considered to be normal responders or high responders, respectively (39). Nonresponders and poor responders should receive repeated hepatitis B vaccination or additional booster vaccinations.
Quality control
Infectious disease specialists and epidemiologists from West China Hospital and West China School of Public Health of Sichuan University were convened to guide scientific design, epidemiological investigation, laboratory test, and statistical analysis. Staff of Fucheng CDC and Mianyang Infectious Diseases Hospital were trained and responsible for administering the questionnaire, collecting the blood specimens, and separating, storing, and transporting the serum specimens.
Ethical issues
The study was approved by the Ethics Committee of West China Hospital of Sichuan University. All study components were done according to the national ethics regulations. All the children, who could understand, and their parents were informed of the purpose of this study. All the personal information was kept confidential. The children and their parents had the rights to withdraw from this study at any time.
Statistical analysis
Qualitative anti-HBs level was the proportion of participants with appropriate anti-HBs level, analyzed using the X 2 test. Quantitative anti-HBs level was presented as median concentration. The other data were presented as mean ± SD. Quantitative anti-HBs levels were compared between groups by the rank sum test because the normal distribution was not satisfied even after data conversion. SPSS software (version 17.0) was used for all statistical analysis. All p-values were two sided, and p < 0.05 was considered as statistically significant.
Results
Of the 1,526 children, the mean age was 8.2 ± 4.1 and 739 children were male. The median anti-HBs level was 23.0 mIU/mL, and the total percentage of anti-HBs level ≥10 mIU/mL was 60.9%. Children whose anti-HBs were positive (anti-HBs level ≥10 mIU/mL) were younger than those anti-HBs-negative children (anti-HBs level <10 mIU/mL) (age 7.8 ± 4.3 vs. age 8.8 ± 3.7, p = 0.000) (Table 1). The anti-HBs levels were undetectable in 200 of the anti-HBs-negative children. The median anti-HBs levels of the anti-HBs-negative children and anti-HBs-positive children were 3.6 and 64.1 mIU/mL, respectively.
Anti-HBs, antibody to the hepatitis B surface antigen.
With the increase of age, the median anti-HBs level declined remarkably in the early period (Table 2 and Fig. 1). The median anti-HBs level in children aged 1 was much higher than that in children aged 3–15 (147.8 vs. 16.2–30.7 mIU/mL, p < 0.05). The median anti-HBs level in children aged 2 was much higher than that in children aged 3–15 (86.8 vs. 16.2–30.7 mIU/mL, p < 0.05). Although the median anti-HBs level in 1-year-old children was higher than that in 2-year-old children, there was no statistical difference (147.8 vs. 86.8 mIU/mL, p > 0.05). With increase of age among children 4–15 years old, the median anti-HBs level increased slightly, but overall, it remained relatively stable (17.7 mIU/mL in children aged 7 vs. 25.3 mIU/mL in children aged 12, p < 0.05; the others, p > 0.05). Between the ages of 3 and 4, median anti-HBs level reached the lowest level.
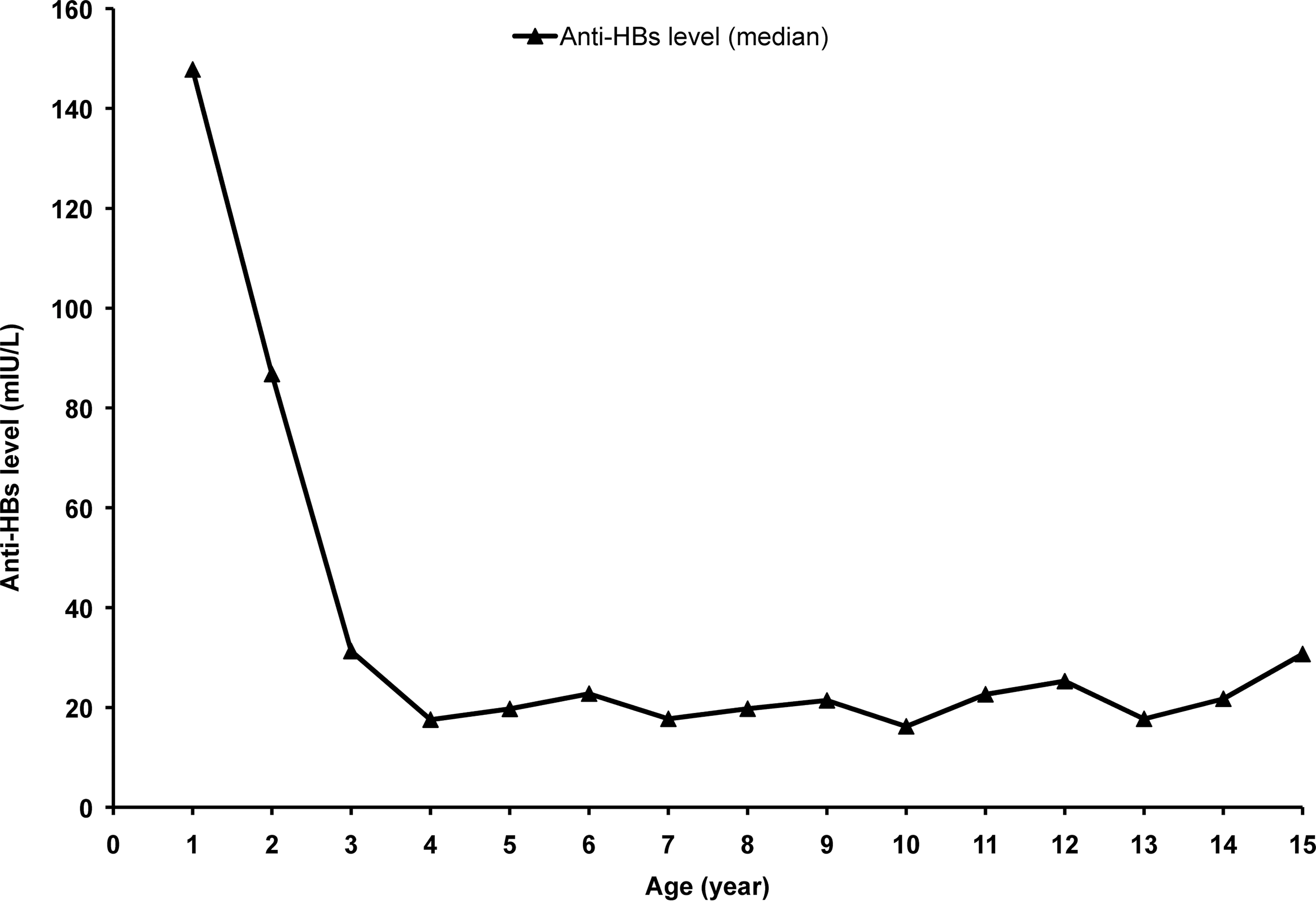
Median anti-HBs level based on ages. Anti-HBs level (median) among children ages 1–15 who received three doses of 5 μg hepatitis B vaccine series during infancy but did not receive a booster vaccination later. Median anti-HBs level in children 1 and 2 years old was much higher than that in children aged 3–15 (p < 0.05, respectively). Anti-HBs, antibody to the hepatitis B surface antigen.
Increasing with age, the percentage of anti-HBs levels ≥10 mIU/mL declined remarkably in the early period and then remained relatively stable (Table 2 and Fig. 2). In the age group of 1-year-old children, who just received full length of hepatitis B vaccination, the anti-HBs-positive rate was 95.3%. Only 4.7% of 1-year-old children had no immune response. The anti-HBs-positive rate was much higher than that in children aged 3–15 (95.3% vs. 52.7–68.3%, p < 0.05). The anti-HBs-positive rate in children of age 2 was much higher than that in children aged 3–15 (88.2% vs. 52.7–68.3%, p < 0.05). The anti-HBs-positive rate was similar between children of age 1 and 2 (95.3% vs. 88.2%, p > 0.05). Although the anti-HBs-positive rate in 3-year-old children was higher than that in children of 4, there was no statistical difference between these age groups (72.1% vs. 58.2%, p > 0.05). Increasing with age among children 4–15 years old, the anti-HBs-positive rates remained relatively stable and the anti-HBs-positive rate was 57.1%. At the age of 3–4, the anti-HBs-positive rate reached the lowest level.
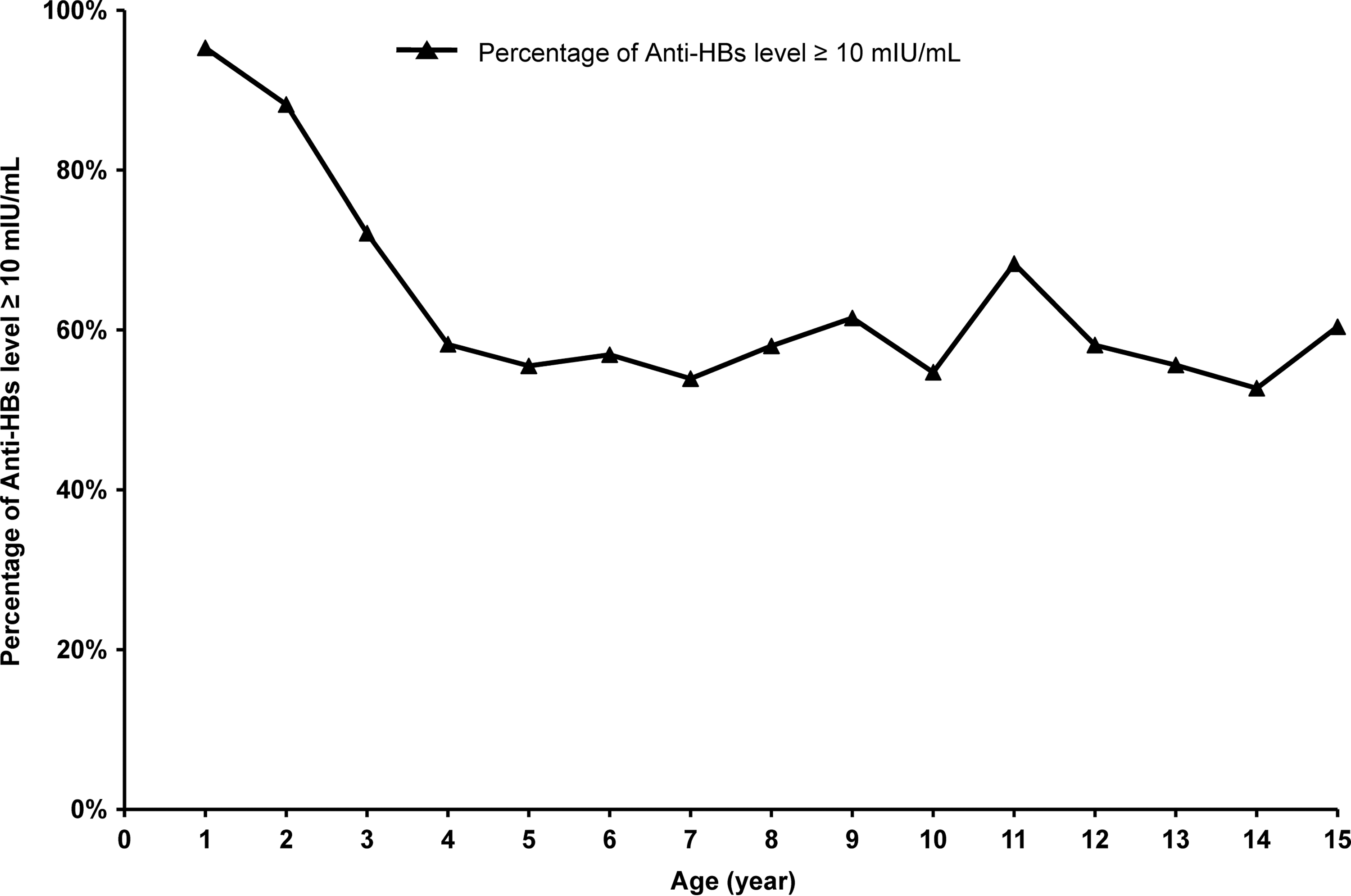
Percentage of anti-HBs level ≥10 mIU/mL based on ages. Percentage of anti-HBs level ≥10 mIU/mL among children ages 1–15 who received three doses of 5 μg hepatitis B vaccine series during infancy but did not receive a booster vaccination later. Percentage of anti-HBs level ≥10 mIU/mL in children 1 and 2 years old was much higher than that in children aged 3–15 (p < 0.05, respectively). Although the percentage of anti-HBs level ≥10 mIU/mL in children 3 years old was higher than that in children age 4, there was no statistical difference between these age groups (p > 0.05).
Increasing with age, the percentage of anti-HBs levels ≥100 mIU/mL declined remarkably in the early period and then remained relatively stable (Table 2 and Fig. 3). About 64.7% children aged 1 had moderate or high immune response and had enough powerful immunity to HBV. The percentage of anti-HBs level ≥100 mIU/mL in children of age 1 was much higher than that in children aged 3–15 (64.7% vs. 13.1–28.0%, p < 0.05). The percentage of anti-HBs level ≥100 mIU/mL in children of age 2 was much higher than that in children aged 3–15 (47.1% vs. 13.1–28.0%, p < 0.05). The percentage of anti-HBs level ≥100 mIU/mL in 1-year-old children was much higher than that in 2-year-old children (64.7% vs. 47.1%, p < 0.05). With the increase of age among children aged 4–15, the percentage of anti-HBs level ≥100 mIU/mL increased slightly, but overall remained relatively stable. The percentage of anti-HBs level ≥100 mIU/mL was about 20.0% in these 4–15-year-old children. At the age of 3, the percentage of anti-HBs level ≥100 mIU/mL reached the lowest level.
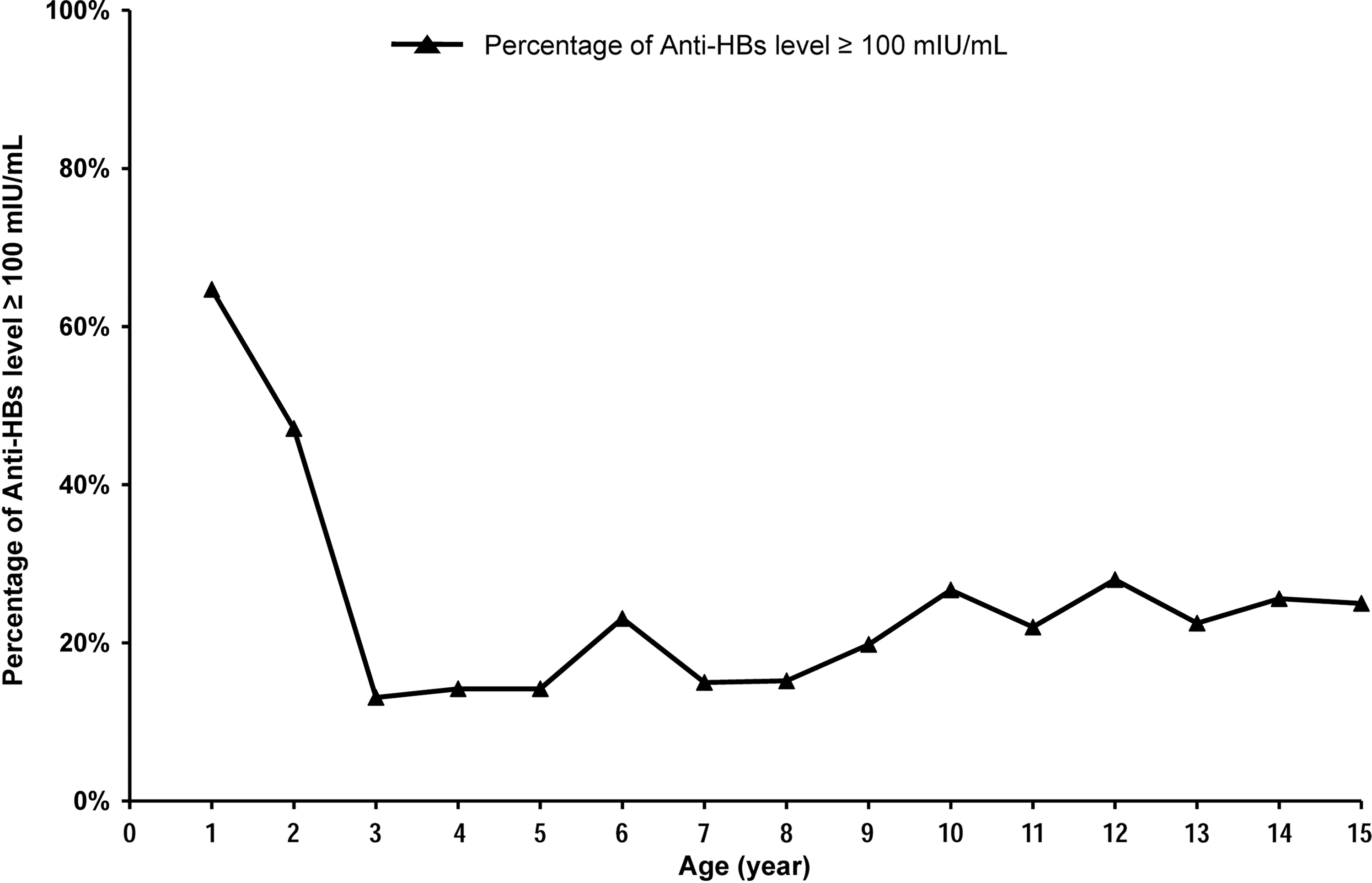
Percentage of anti-HBs level ≥100 mIU/mL based on ages. Percentage of anti-HBs level ≥100 mIU/mL among children ages 1–15 who received three doses of 5 μg hepatitis B vaccine series during infancy but did not receive a booster vaccination later. At age 3, the percentage of anti-HBs level ≥100 mIU/mL reached the lowest level. Percentage of anti-HBs level ≥100 mIU/mL in children 1 and 2 years old was much higher than that in children aged 3–15 (p < 0.05, respectively).
As shown in Table 2 and Figure 4, the percentage of anti-HBs level <100 mIU/mL increased remarkably in the early period and then remained relatively stable. The percentage of anti-HBs level <100 mIU/mL in children of age 1 or 2 was much lower than that in children aged 3–15. The percentage of anti-HBs level <100 mIU/mL in children aged 1 was much lower than that in children aged 2. With the increase of age among children 4–15, the percentage of anti-HBs level <100 mIU/mL decreased slightly, but overall remained relatively stable. The percentage of anti-HBs level <100 mIU/mL was about 80.0% in these 4–15-year-old children. At the age of 3 years, the percentage of anti-HBs level <100 mIU/mL reached the highest level.
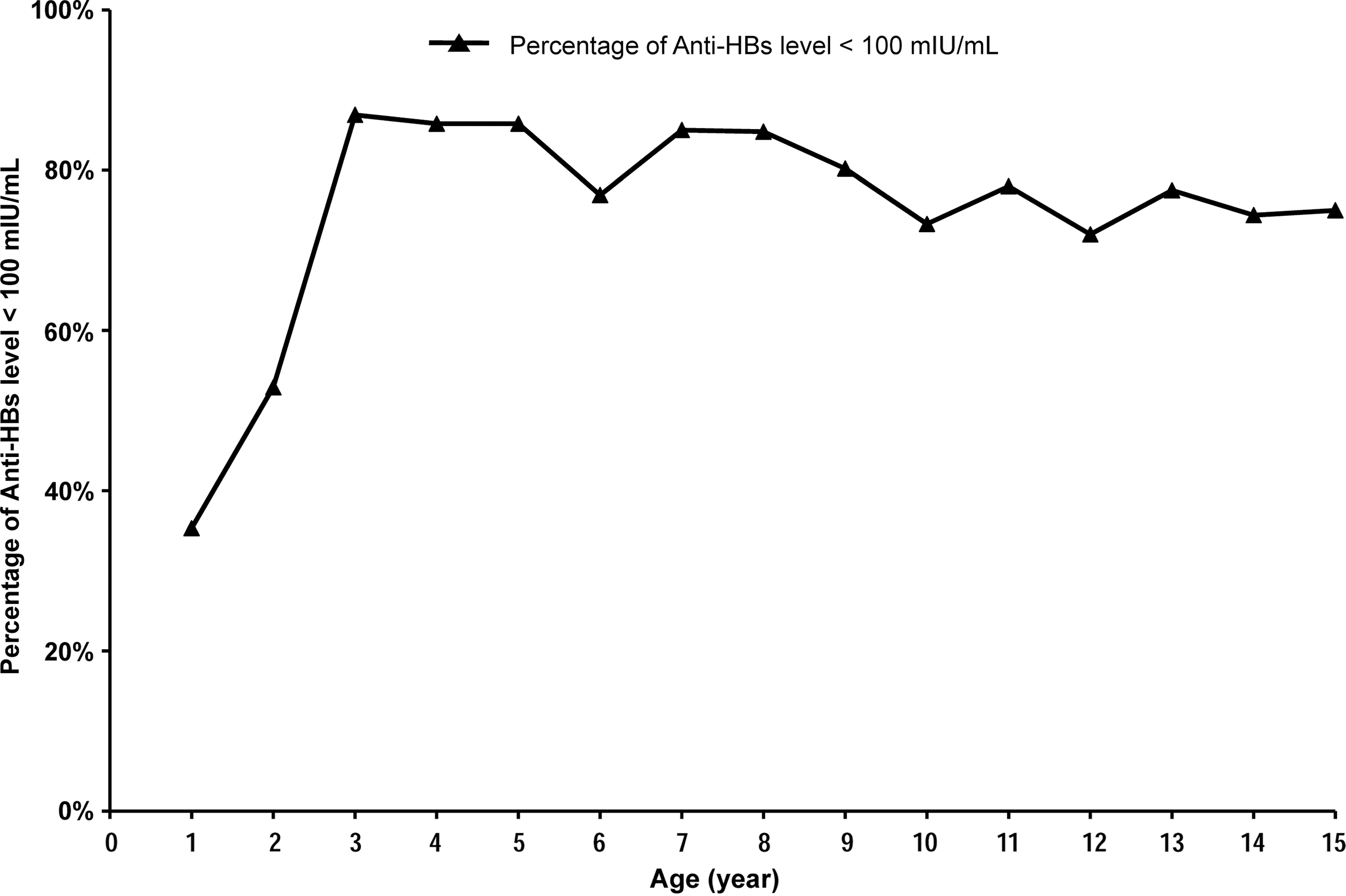
Percentage of anti-HBs level <100 mIU/mL based on ages. Percentage of anti-HBs level <100 mIU/mL among children ages 1–15 who received three doses of 5 μg hepatitis B vaccine series during infancy but did not receive a booster vaccination later. At age 3, the percentage of anti-HBs level <100 mIU/mL reached the highest level. Percentage of anti-HBs level <100 mIU/mL in children 1 and 2 years old was much lower than that in children aged 3–15 (p < 0.05, respectively).
The anti-HBs-positive rates in children aged 1–4, 5–9, and 10–14 and 15 were 74.6%, 56.6%, 57.1%, and 60.4%, respectively (Table 3). The anti-HBs-positive rate in children aged 1–4 was much higher than that in other age groups (74.6% vs. 56.6%, 57.1%, and 60.4%, p < 0.05). The anti-HBs-positive rates were similar among children aged 5–9, 10–14 and 15 (56.6% vs. 57.1% vs. 60.4%, p > 0.05). Although hepatitis B vaccination has become a nationwide universal vaccination program and has been provided for free in China since 2005, and the anti-HBs-positive rate in children aged 1–4 increased from 71.2% to 74.6% over the past 4 years before this study (2007–2011), there was still no statistical difference between this study and the epidemiological serosurvey of hepatitis B in China in 2006 (74.6% vs. 71.2%, p > 0.05).
Data from this study.
Data from the epidemiological serosurvey of hepatitis B in China at 2006 (19).
Discussion
Although there has been great progress in reducing HBsAg prevalence and increasing anti-HBs prevalence, about 40% of the Chinese population aged 1–59 was antis-HBs negative until 2006 (19). People with negative anti-HBs still have the risk of getting HBV infection and are recommended to receive routine immunization or a booster vaccination, leaving the appropriate vaccination time point and specific program still to be elucidated. The findings from this survey indicate that the immunity against HBV infection is rapidly weakened in the early ages of children aged 15 and younger who received three doses of 5 μg hepatitis B vaccine series during infancy in China. Anti-HBs reached the lowest level at the age of 3 and then remained relatively stable.
The median anti-HBs level, the percentage of anti-HBs level ≥10 mIU/mL, and the percentage of anti-HBs level ≥100 mIU/mL reached the lowest level at the age of 3, and only 64.7% children of age 1, 47.1% children of age 2, and 13.1% children of age 3 got a good immune response. Due to the limitation of the cross-sectional study, whether children aged 3–15 with anti-HBs level ≥100 mIU/mL were mainly from the good responders after the vaccination program is uncertain. It is also unclear whether children aged 1–2 with anti-HBs level <100 mIU/mL maintained that level without change. Although many researches focused on evaluating immune effect, almost all of them used anti-HBs-positive rate rather than anti-HBs level as the important evaluating indicator. To our knowledge, no research has been dedicated to perform a longitudinal study to investigate the evolution of the anti-HBs level in children who received primary immunization till now.
Consistent with our observations, a Chinese study from another representative area for control and prevention of major infectious diseases showed that, of 675 preschool children, there was a negative correlation between the anti-HBs-positive rate and age in children under 3 and the anti-HBs-positive rate remained stable in children above 3 (17). A study from Taiwan found that older age was an independent factor associated with positive HBsAg (12). The possibility of a low level of or even negative anti-HBs for children at or under age 3 should be a concern. Repeated hepatitis B vaccination or additional booster vaccination should be provided to these children to get more powerful immunity to HBV.
Over the past 4 years before this study (2007–2011), the hepatitis B vaccination program during infancy had continued, but the anti-HBs-positive rate in children aged 1–4 in this study in 2011 was still similar to that in the epidemiological serosurvey of hepatitis B in China at 2006 (19). It seems difficult to get a much higher anti-HBs-positive rate only by administering hepatitis B vaccination program during infancy.
Meanwhile, the percentage of anti-HBs levels <100 mIU/mL increased remarkably in the early period and then remained relatively stable. The anti-HBs-positive rate in our study among children aged 4–15 (57.1%) was similar to that in the epidemiological serosurvey of hepatitis B in China in 2006 and that reported by McMahon et al. (19,26). McMahon et al. found that 60% of 493 participants who received primary immunization with plasma-derived hepatitis B vaccine during childhood and adulthood still had an anti-HBs level ≥10 mIU/mL at least 22 years later (26). It indicates that it may not be appropriate for all children to receive the three doses of 5 μg hepatitis B vaccine series during infancy, and it may not be enough for some children who only receive primary immunization during infancy without receiving repeated hepatitis B vaccination or additional booster vaccination.
Many factors are involved in poor and nonresponse to hepatitis B vaccination, and a low dose of hepatitis vaccine was suggested to be one of the most important reasons (12,29). One study from China compared the antibody response induced by primary immunization with 5 and 10 μg hepatitis B vaccine made by recombinant DNA techniques on 0-1-6 schedule among 13,523 newborns aged 7–12 months (39). The non, poor, normal response rates were all higher in the 5 μg group than in the 10 μg group (p < 0.01), while the high-response rate and the geometric mean concentration were much higher in the 10 μg group than in the 5 μg group (p < 0.01 and p < 0.001, respectively) (39).
Recently, one study found that the 10 μg strategy should be cost-effective, even more possibly highly cost-effective or cost-saving, compared with the current 5 μg strategy for newborn hepatitis B vaccination in China (38). Moreover, 10 μg hepatitis B vaccine is not much more expensive than 5 μg vaccine in China, suggesting that 10 μg hepatitis vaccine should be recommended and could be provided freely to all newborns to get much more powerful immunity to HBV during the young age.
Researchers already observed that people who received hepatitis B vaccination during infancy may keep immune memory against HBV (4,26,33,34,37); therefore, the hepatitis B immunization program for these persons may differ from that in the neonatal period. Until now, the appropriate vaccination program for anti-HBs-negative people who already received the hepatitis B vaccination during infancy is not clear. Although we did not conduct a reimmunization program in this study to propose some immunization strategy for these children, some studies had investigated the effect of several immunization programs.
McMahon et al. found that 81% of 164 participants whose anti-HBs levels were <10 mIU/mL responded to a booster dose of 10 μg of hepatitis B vaccine 60 days later (26). Considering participants with an anti-HBs level ≥10 mIU/mL 22 years later and those who responded to the booster dose, the protection afforded by hepatitis B vaccination was demonstrated in 87% of the participants (26). Two studies demonstrated that 10 μg of hepatitis B vaccine was more effective than 5 μg of hepatitis B vaccine (6,18). In another study conducted by Wu et al. (37), a booster dose of 20 μg of hepatitis B vaccine was administered to 1974 HBsAg- and anti-HBs-negative high school students who received postnatal passive–active hepatitis B vaccination. The total proportion of postbooster anti-HBs titer ≥10 mIU/mL was 72.1%.
Participants with prebooster anti-HBs level of 1.0–9.9 mIU/mL had a significantly higher postbooster anti-HBs level than those with prebooster anti-HBs level of <1.0 mIU/mL (37). Similarly, one study found that the prebooster antibody titer higher than 2 mIU/mL in adults might be predictive of an anamnestic response to booster vaccination, whereas the titer below this value may indicate likelihood of nonresponse (7).
The efficacy of modified three-dose booster protocol (recombinant DNA HBV vaccine, each time 20 μg) in neonatally vaccinated college students in Taiwan was studied by Su et al. (33). Of the 316 students with anti-HBs level <10 mIU/mL, 75.3% (238/316) of them responded to a dose booster of hepatitis B vaccine 4 weeks later. The rest 78 students with anti-HBs level <10 mIU/ml received another dose of the HBV vaccine, followed by a third dose 5 months later. One hundred twenty-eight of the 316 students were still followed up 3 years later. It was believed that 95.3% (122/128) of the students maintained protective anti-HBs 1 month after completing the modified three-dose booster protocol 3 years ago (33). Several studies have suggested a success rate of greater than 95% for maintaining a protective anti-HBs level, followed by three booster doses of the HBV vaccine in adolescents and young adults (6,14,15,21). These studies demonstrated that the three-dose booster protocol benefits nonresponders with a high conversion of anti-HBs and long-term persistence of seroprotection.
In conclusion, the results of this study showed that higher doses, 10 μg instead of 5 μg, of hepatitis B vaccine for the newborn in China should be provided to get much more powerful immunity to HBV, and there is a necessity to make a complementary universal vaccination program, especially for the nonresponders, poor responders, and the responders whose anti-HBs diminished years later. Although appropriate use of hepatitis B vaccines for newborns is still very important to control HBV infection more intensively and eliminate it eventually in a visible future, intensive supplementary vaccination should be given to other people with negative anti-HBs or a low level of anti-HBs. It should be considered as a routine work of postvaccination detection of anti-HBs levels. As long as the anti-HBs level is <10 mIU/mL, even <100 mIU/mL, appropriate booster hepatitis B vaccinations should be provided for more powerful immunity to HBV.
Footnotes
Acknowledgments
This study was supported by the National Science and Technology Major Project for major infectious diseases such as AIDS and viral hepatitis prevention and control (2009ZX10004-905) and the Science and Technology Support Project of Sichuan Province (2013SZ0002; 2014SZ0109).
Special thanks to postgraduate students of West China School of Public Heath, Sichuan University, and health workers of Mianyang Fucheng Centers for Disease Control and Prevention, Mianyang Centers for Disease Control and Prevention, and Mianyang Infectious Diseases Hospital for their strong collaboration in this study. All authors had full access to all of the data in this study and took responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
No competing financial interests exist.