
Abstract
Influenza vaccination is the most effective method in preventing influenza and its complications. This study's objectives were to investigate the vaccination coverage and frequency and to assess knowledge, attitudes, and practices toward influenza vaccination in Jordan during the year 2012 and the 5 years preceding it. Additionally, it aimed at identifying the barriers and motivations to receive the vaccine and the factors contributing to its uptake. In May 2012, a self-administered cross-sectional survey was distributed to 3,200 adults conveniently selected across Jordan to explore influenza vaccination status, knowledge, attitudes, and practices toward the influenza vaccine. The survey response rate was 98.3%. The overall coverage rate of seasonal influenza vaccination ranged from 9.9% to 27.5%. Results of the univariate analysis revealed that males, participants older than 45 years, business owners, and university students or graduates were more likely to take the vaccine. Healthcare workers (HCW) showed higher rates than non-HCW and those with concomitant chronic diseases were more committed to receive the vaccine. Knowledge about the influenza vaccine is considered high in the Jordanian population. Fear from side effects was the major barrier, while the fear of the virus spread and outbreak was the major reason to receive the vaccine. The coverage rates were low in Jordan compared to other countries. The need for influenza vaccine campaigns and on-going education in Jordan health schools is crucial to increase the rate and remove misconceptions and negative attitudes toward vaccination.
Introduction
I
Serious illnesses and deaths due to influenza are common in high-risk people such as those older than 65 years and those younger than 2 years, pregnant women, and those with chronic diseases such as lung, kidney, metabolic, or heart diseases (2,3,7,28,31). For such individuals, annual influenza vaccination is considered the most effective method of protection against influenza and its complications (10).
Recent reports have highlighted that vaccination coverage of people with chronic infections in the highly developed countries is highly variable ranging between 31% and 76%. The barriers to influenza vaccination in these countries include low perception of risk such as risk of infecting others, fear of side effects, cost issues, and lack of accurate information about the disease and the vaccine itself (8,13).
In Jordan, seasonal influenza vaccine is available in community pharmacies to the public at a cost, since it is not part of the national vaccination program. However, it is offered free of charge, but not mandatory, to healthcare workers (HCW) in the government sector, but not in private or nongovernment sectors. There are no official reports on influenza vaccination coverage among Jordanians and no national surveillance programs or awareness campaigns for the vaccine in the country. Thus, understanding determinants of influenza vaccine low uptake and of “vaccine hesitancy” is needed to plan, implement, and evaluate effective immunization programs in Jordan.
To the best of the author's knowledge, no previous data on the uptake of the influenza vaccine, knowledge, and attitudes of the Jordanian population toward it were reported. In light of this, their determination is an essential first step to postulating recommendations on vaccination practices in Jordan. The objectives of this study are to investigate the coverage rates in Jordan in general, during the study season 2011/2012 and the 5 years preceding it (2008–2012), and to assess the Jordanians' knowledge and explore their attitudes and practices (KAP) toward the use of the influenza vaccine. It also aims at identifying the barriers and motivations to receive the vaccine and to identify factors contributing to the use of the vaccine. Finally, it aims at comparing the responses of HCW with the rest of the participants.
Materials and Methods
Study design and participants
A cross-sectional study was carried out between February and May 2012. A prevalidated, self-administered, anonymous questionnaire was distributed by trained research assistants in paper format to a sample of 3,200 Jordanians older than 18 years after obtaining verbal informed consent. Respondents were members of the general public allocated in different cities in Jordan from different locations such as shopping malls, supermarkets, hospitals, universities, house-bound people, and others.
A comprehensive description of the study was introduced in the first page of the questionnaire and explained to the respondents by the research assistants. The respondents were informed that the study is voluntary and were assured that the answers will be treated confidentially. Questionnaire forms were collected by the research assistants from respondents on the spot after completion.
Questionnaire development
The questionnaire was designed after reviewing validated questionnaires in literature (1,11,17). The questionnaire is available on request. The following information was collected: respondents' demographics and health conditions, their views and knowledge about influenza and its vaccine, vaccine availability, sources of information to know about the vaccine, and their general attitudes and practices toward vaccination (reasons to be vaccinated or not and motivations to consider vaccination). They were also asked to indicate whether their physicians advised them to take it. Vaccination history was also collected; respondents were asked to indicate whether they had been vaccinated previously (termed as in general), vaccinated within the study season 2011/2012, vaccinated within the 5 years (2008–2012) preceding the study season 2011/2012, and the number of times receiving the vaccine within those 5 years.
The knowledge score for each respondent was estimated by asking respondents to rank their agreement with eight statements using a Likert scale. They were asked about the vaccine role, benefits and side effects, the involvement of the immune system in influenza disease and vaccine, the disease and its complications, vaccine side effects, and prophylactic role. Responses were analyzed by recoding the value 2 as “agree,” the value 1 as “neutral,” and the value 0 as “disagree.” A score of 16 indicated the best knowledge toward the given statements.
Similarly, respondents were asked to rank their agreements with the contents of three statements on attitude, using the same scale, to elicit their score. Statements were on influenza vaccine safety and necessity for students, HCW, elderly, children, and pregnant women. A score of 6 indicates highly supportive views toward the given statements.
Validation and reliability
The initial draft of the questionnaire was circulated among the members of the research team and modifications were implemented to enhance clarity and readability of the study questionnaire. Validity and reliability of the questionnaire were evaluated by an expert committee of two clinical pharmacists, one clinical immunologist, one clinical microbiologist, and one statistician. This was to ensure that its applicability was relevant to the Jordanian population. The questionnaire was translated from English into Arabic and back by two senior academic staff members who were fluent in both languages. The questions were written with no medical jargons or difficult terminology. The questionnaire was pretested and validated on a pilot sample of 100 participants representing 3% of the target sample to clarify any ambiguities and to ensure that the data would provide reliable information. Internal consistency reliability was tested by the Cronbach's alpha coefficient.
Statistical analyses
Statistical analyses were conducted using SPSS version 17.0 for Windows (SPSS, Inc., Chicago, IL). Pearson's chi-square was used to compare categorical variables. Bivariate analysis was used to measure the correlation between receiving the vaccine and other independent variables. Results were considered significant when p-value was less than 0.05 and highly significant when p-value was less than 0.01. In a few cases, some participants failed to answer some questions, resulting in missing data, which were not included in the analysis. Descriptive measures presented include percentages and mean or median as appropriate.
Multiple logistic regressions
Multiple logistic regressions were performed to identify predictors for the use of influenza vaccination among Jordanians. Whether the participant took the vaccine or not during the last 5 years, including the study year (2008–2012), was the dependent variable. Odds ratios (ORs) were determined by stepwise backward elimination.
Results
Sociodemographic characteristics
Of the 3,200 Jordanians who were offered to participate in the study, a total of 3,145 answered the questionnaire with a response rate of 98.3%. Forty-one forms (1.3%) were excluded due to incompletion, missing data, or being inappropriately answered. Consequently, 3,104 participants completed the survey and were included in the study analysis.
Respondents were generally younger than 45 years, 2,489 (80.2%), married, 1,583 (51%), and with a majority being females 1,798 (57.9%). They were mainly university graduates 2,077 (66.9%) and 811 (39%) of them were employees followed by 695 (21.2%) students. Respondents working in health sectors comprised 522 (16.8%). The majority of respondents were living in the capital city and in central Jordan, with a monthly household income ranging between JD 350 and 1,000 ($500–1,500), and with average family members of four to six persons. The majority of the respondents, 2,216 (71.4%), were free from chronic diseases, while 170 (5.5%) reported having diabetes, 104 (3.4%) with cardiovascular disease, and 100 (3.2%) having asthma.
Demographic characteristics of the study respondents are summarized in Table 1.
JDs, Jordanian dinars.
Influenza vaccination coverage rates of the study sample
In this study, the coverage rate is defined as the number (percentage) of people who have received the vaccine at least once during the mentioned periods in the study sample surveyed. A total of 853 (27.5%) participants reported receiving the influenza vaccine previously. Of the occupational groups, business owners showed the highest vaccination rates (41.1%) followed by students and office employees, 27.6% and 27.3%, respectively. The majority of the participants, 1,084 (34.9%), reported having the influenza disease only once yearly, where 792 (73.1%) of them did not receive the vaccine previously.
The influenza vaccination coverage rate for 2011/2012 season was only 9.9%. The coverage rate during the 5 years preceding the study season, that is, from 2008 to 2012 was 22.3% (i.e., vaccinated at least once during this period). One hundred thirteen respondents (3.6%) had the vaccine more than three times between 2008 and 2012. Business owners also showed the highest coverage rates (17.1%) during the study season 2011/2012 and 27.4% throughout 2008–2012 ranging from one to three times. The coverage rate was significantly higher among participants older than 45 years who took the vaccine during 2011/2012 and 2008–2012 seasons (12.8% vs. 9.2%, p = 0.007 and 25.8% vs. 21.4%, p = 0.007, respectively).
Influenza vaccination coverage rates among individuals with chronic diseases
The general vaccination coverage rate of those who reported having chronic diseases was 35.6%, with the majority (58.6%) older than 45 years. Almost 30% of those with chronic diseases were older than 45 years and reported having diabetes as the major disease. The vaccination coverage rate in the 5 years (2008–2012) preceding the study season was 32.1%, while it was only 18.4% in the study season (2011/2012). Among those who received the vaccine between 2008 and 2012, 76.6% had it once to three times. Diabetes was the major chronic disease affecting almost 40% of the participants who received the vaccine previously for at least once over the 5 years preceding the study.
Influenza vaccination coverage rates among HCW
Thirty-six percent of HCW participants received the vaccine previously. Almost 50% of them indicated receiving the vaccine in the study season of 2011/2012. On the contrary, 25.6% of the non-HCW participants received the vaccine previously, while one-third of them received it in 2011/2012 study season. In the 5 years before the study season (2011/2012), 25.6% of the non-HCW participants received the vaccine at least once. Of the two age groups (18–45 years and older than 45 years), the coverage rate was significantly higher for the group of 18–45 years of age during the study season 2011/2012 (12.8% vs. 5.4%, p = 0.010) and during the 5 years preceding them (25.6% vs. 8.2%, p = 0.008). Other vaccination coverage rates for HCW and non-healthcare workers (non-HCW), in general, during the study season 2011/2012 and over the 5 years preceding the study are shown in Figure 1.
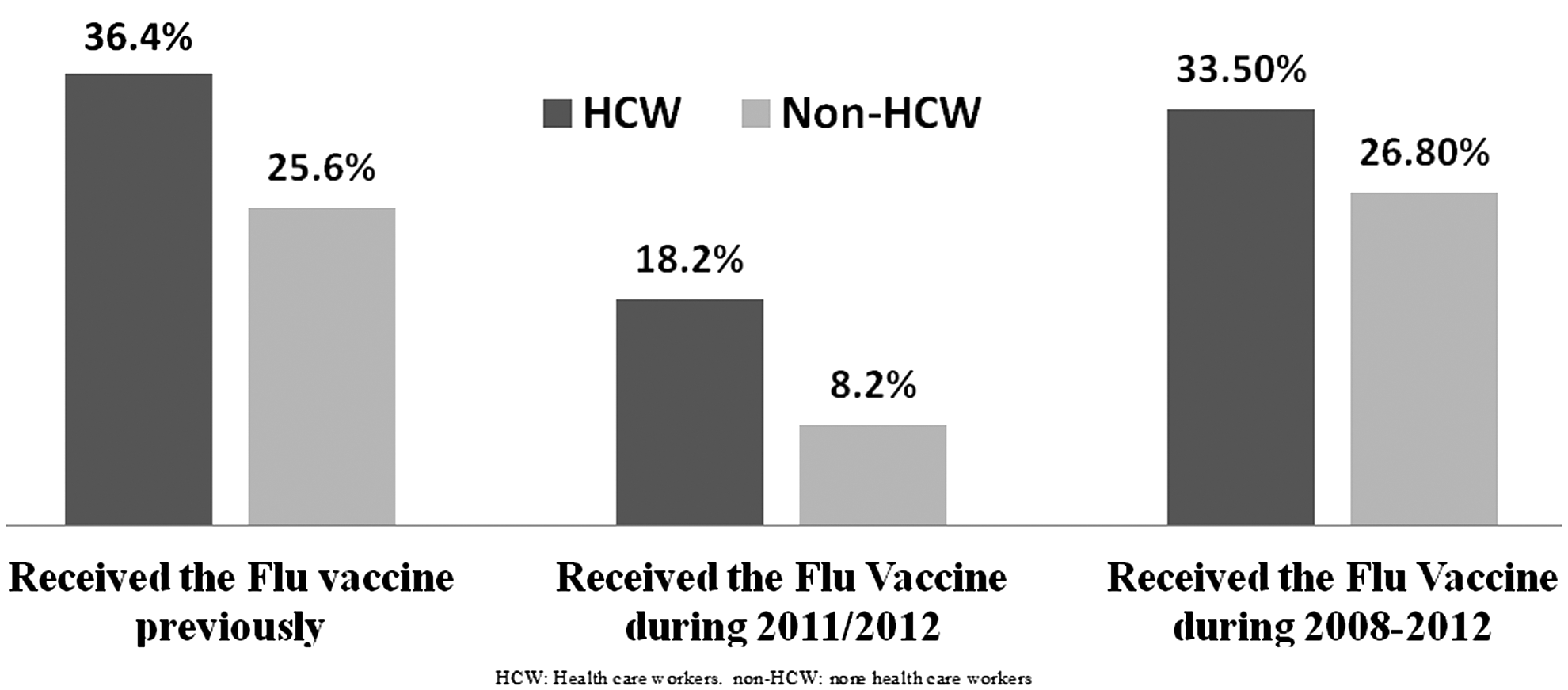
Vaccination coverage rates for the HCW and the non-HCW participants. HCW, healthcare workers.
Frequency of vaccination over the 5 years preceding the study
When the participants were asked about the number of times they received the influenza vaccine during 2008 and 2012, 579 (18.7%) reported receiving it once to three times, while only 113 (3.6%) received it more than three times. A total number of 146 (83.4%) of the 175 HCW who received the vaccine during the study season 2011/2012 reported receiving it once to three times during the 5 years preceding the study season (2008–2012). Figure 2 shows the frequency of receiving vaccine among HCW and non-HCW. The proportion of HCW who received vaccine up to three times or more was almost double the proportion of non-HCW.
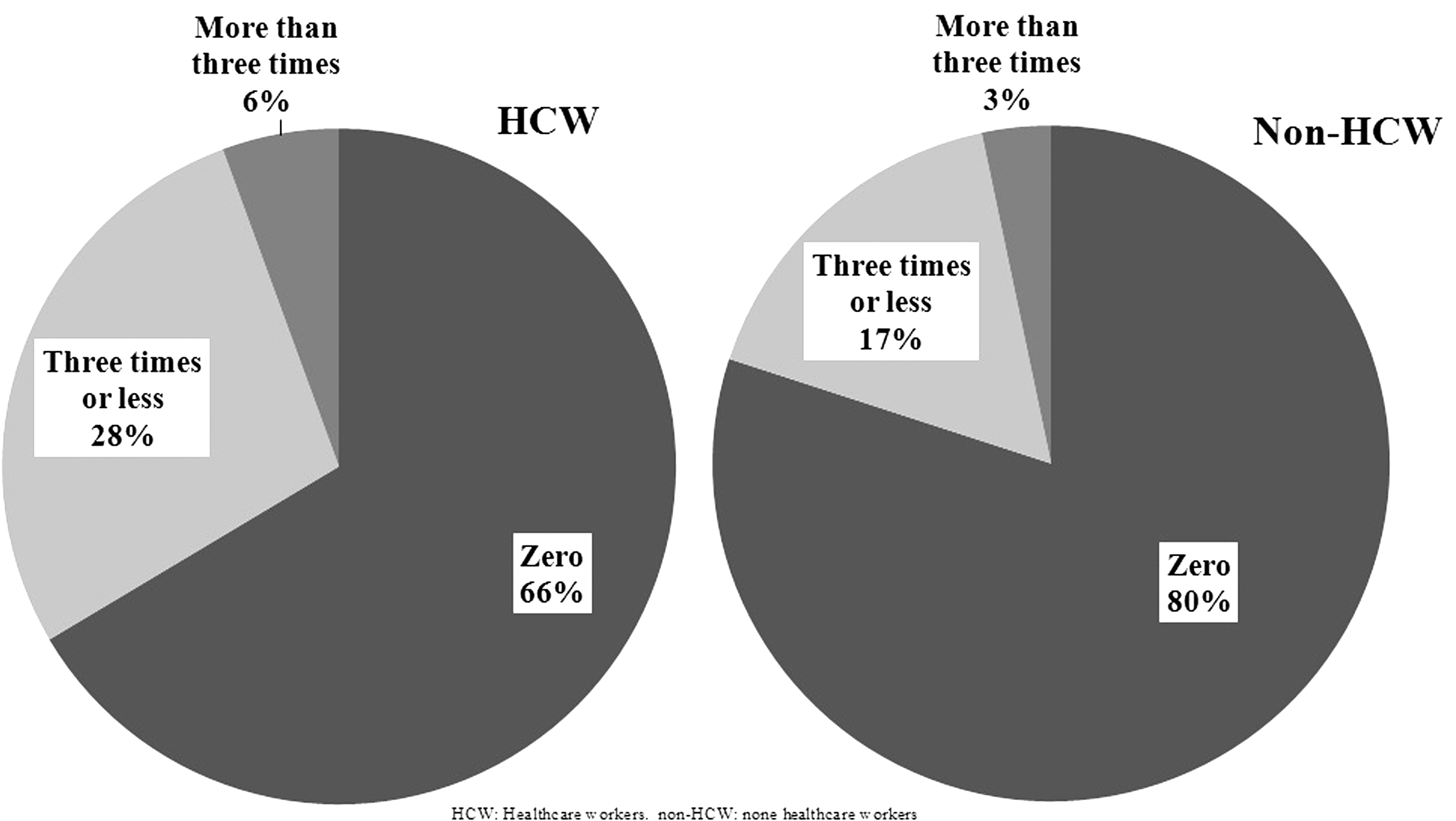
The frequency of vaccination times among the HCW and non-HCW participants between 2008 and 2012.
Knowledge about the influenza vaccine
The majority of the study participants knew about the vaccine, while only 158 (5.1%) of them admitted that they have never heard about it before. Those who knew about the vaccine indicated that they heard about it from friends/family members, 803 (25.9%), or from TV/media 732 (23.6%). Other sources were the Internet, physicians, and medical brochures.
A higher percentage of HCW participants compared to non-HCW participants knew about the vaccine, 455 (87.2%) and 1,126 (43.6%), respectively. Of the HCW participants, 56.1% learnt about the vaccine during their university/college study. Regarding non-HCW participants, 29.8% knew about it from family members/friends and 26% knew about it from TV/media.
The mean (standard deviation [SD]) knowledge score was 12.61 (0.2) out of 16. Mean knowledge scores for the HCW were significantly higher than those of non-HCW: 13.72 (0.14) and 10.41 (0.34), respectively. Half of the questions were answered with agree by both HCW and non-HCW participants. As for the other four questions regarding the benefits and side effects of the vaccine and the effects of the vaccine and the immune system on each other, the majority of the non-HCW answered with neutral/uncertain, while HCW agreed that they feel very informed about them.
Attitudes, beliefs, and practices toward the benefits and effects of the influenza vaccine
A total of 1,681 (54.2%) of the participants indicated that autumn is the best season for receiving the influenza vaccine. Of the respondents who received the vaccine, 399 (46.8%) believed that the vaccine protection would last for 1 year. More than one-third of those who received the vaccine believed in the prophylactic role of the vaccine and reported that they took it to protect themselves from infected people around them. Sixty-one percent (1,564) of the non-HCW respondents reported that if a family member gets flu with serious complications, they would follow their physicians' advice regarding receiving the vaccine, while 42.9% (224) of the HCW indicated that they would receive it to protect themselves and their families. In general, 693 of the non-HCW reported that they would receive it if recommended by their physicians, taking into consideration that 563 (81.2%) of them did not receive the vaccine previously. Moreover, the main reasons for receiving the vaccine by the majority of HCW (75.3%) and the non-HCW (55%) who previously received the vaccine were to protect themselves and the people around them. Also, the majority of the HCW (75.8%) and the non-HCW (65.4%) who previously received the vaccine believed that the vaccine is effective. Table 2 presents some beliefs in the influenza vaccine comparing total participant responses with HCW responses.
Respondents were asked to choose one answer. p-Values <0.05, chi-square test.
HCW, healthcare workers.
The majority of participants, 2,036 (65.6%), believed that the vaccine is effective, and 577 (67.6%) of those who received the vaccine previously were in agreement with this. Four hundred thirty-eight (41%) of 1,068 who believed that the vaccine is ineffective had previous experiences with friends/family members who took it without experiencing any benefits. While 64.9% reported that the vaccine will become ineffective due to the development of new viral strains. Other participants' beliefs in the ineffectiveness of the influenza vaccine are indicated in Table 3.
Percentages of participants who expressed agreement with the statements.
The majority of the participants, 2,166 (69.8%), reported that they will consider receiving the vaccine if it is offered for free. Of them, 1,438 (66.4%) did not receive the vaccine previously. The attitude score (SD) of participants toward the influenza vaccine safety, necessity for students, HCW, elderly and pregnant women was 4.28 (0.2) out of 6. Both HCW and non-HCW participants had almost similar attitude scores: 4.22 (0.13) and 3.98 (0.06), respectively. However, less than 50% of non-HCW agreed that the vaccine is safe and not harmful, whereas 40.9% were uncertain/neutral. On the contrary, 62% of the HCW agreed that the vaccine is safe, and the rest were either uncertain/neutral or disagree. Although more than 50% of the participants agreed that influenza vaccine should be mandatory for students and HCW, almost 30% of the rest were totally in disagreement with this statement. Finally, the majority of the participants completely disagreed with the statement indicating that the vaccine is only for children, pregnant women, and elderly. This response is higher among HCW (69.5%) compared to non-HCW (55.8%).
Reasons for and barriers against receiving the vaccine among the study sample
Eight hundred (25.8%) participants indicated that they took the vaccine based on their physician's advice. Fifty-nine patients (1.9%) indicated that their physicians actually advised against the use of the vaccine. An analysis of participants who did not receive the vaccine previously showed that 932 (41.4%) reported that they might receive it if free of charge and 719 (77.1%) reported they will take it only after physician counseling and not self-decision. In addition, 884 (40.1%) indicated that fear from side effects was the major reason for not taking the vaccine and even one-third of the HCW participants had the same fear.
When all participants were asked to depict the main reasons that would encourage them to receive the vaccine, the majority (69.9%) indicated that it is because the virus spreads easily in the air and in crowded areas, which makes them vulnerable to infection. Reasons for and barriers against receiving the vaccine are presented in Figure 3.
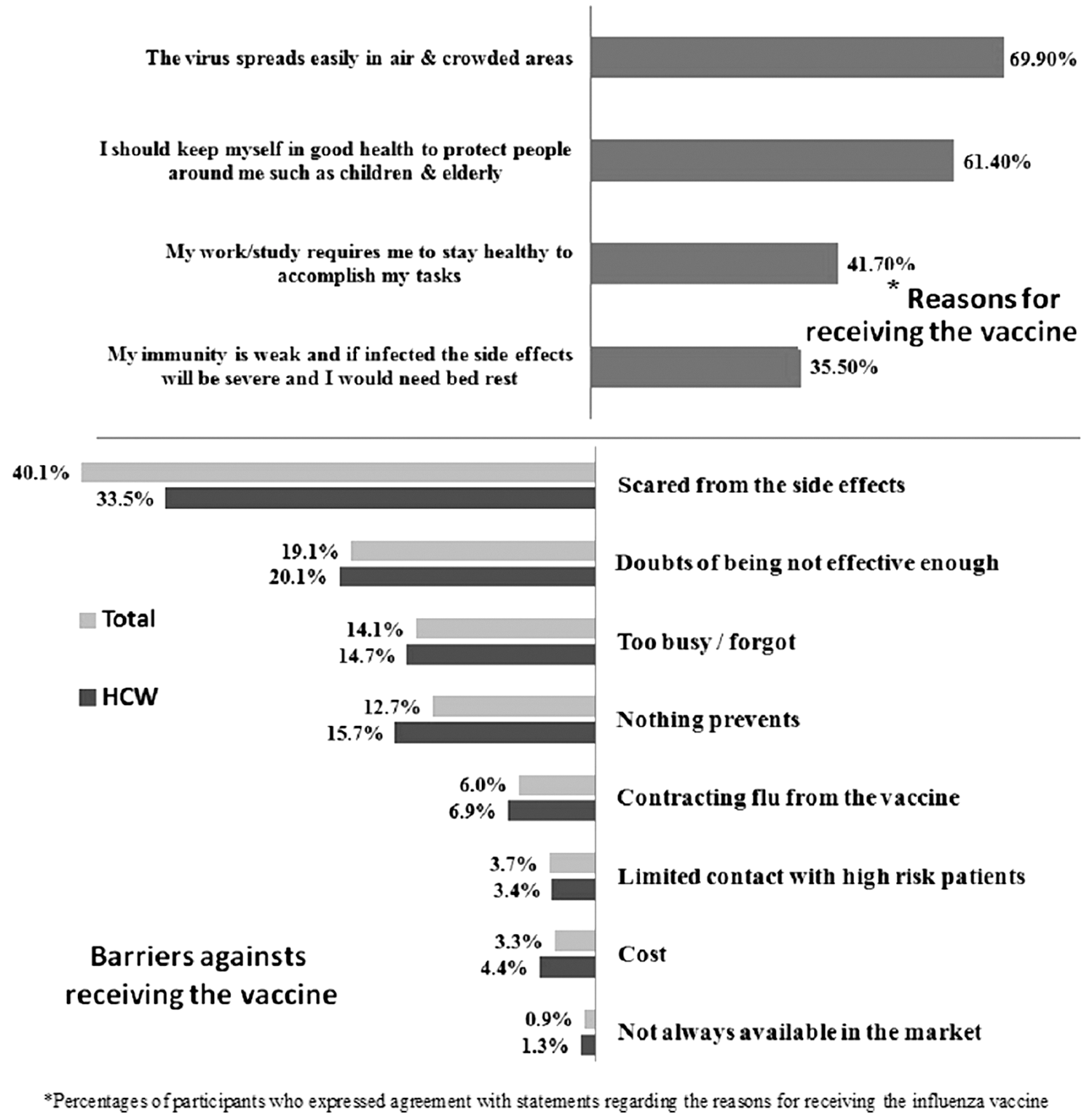
Reasons for receiving the vaccine by all participants, and barriers against receiving the vaccine by those who did not receive the vaccine previously. Total denotes all those who did not receive vaccine previously compared to HCW who did not receive it previously, too.
There were no significant differences in the ratios of HCW and non-HCW reasons for receiving the vaccine other than the reason regarding the importance of being healthy to accomplish their work/study, where HCW obtained a significantly higher ratio (51.3%) compared to non-HCW (39.7%). In contrast, fear from side effects was also a major barrier against receiving the vaccine by both HCW and non-HCW participants. It showed a significantly higher ratio for non-HCW (41.4%) compared to HCW (33.5%). The second highest ratio for both HCW (20.1%) and non-HCW (18.7%) reported was their doubts of being ineffective.
Factors associated with receiving the influenza vaccine
The logistic regression model investigating the predictor of vaccine uptake among Jordanians is presented in Table 4. Independent variables, including age, marital status, number of family dependents, were not found significant predictors for receiving the influenza vaccine.
Bold values represent statistically significant differences with P < 0.05.
Compared to respondents living in Amman.
Compared to respondents not working.
Compared to unmarried respondents.
Compared to family income more than 1,000 JDs.
Compared to families with dependents more than 10.
CI, confidence interval; OR, odds ratio.
Males were more likely to use vaccine as well as older respondents and those who obtained a higher education level. Compared to respondents living in Amman, those who lived in other areas were less likely to take the vaccine. However, this was not a significant predictor.
Those working in the medical field were more likely to take the vaccine; OR (95% CI) = 1.5 (0.51–0.81), p < 0.05. Business owners and office employees appeared more likely to take the influenza vaccine, p < 0.05. Family income was shown as a significant predictor where families with income between 350 and 700 JDs ($500–$1,000) were more likely to take the vaccine.
The earlier model demonstrated good fit for the use of flu vaccine (p = 0.63, Hosmer & Lemeshow test) and it accounts for 15% (Nagelkerke R2 = 0.13) of the variances.
Discussion
Influenza vaccine coverage rates and frequencies
Overall, the influenza vaccination coverage rate for Jordanian adults was 9.9% for the study season 2011/2012. The rate over the 5 years preceding 2011/2012 is 27.5%. This 5-year rate is comparable to what was recently reported in a neighboring country, Lebanon, for the season of 2014/2015, where the overall seasonal influenza vaccination rate was 27.6% (14).
In general, a significant involvement of people exceeding 45 years of age was noticed. This is expected as they are at a higher risk than the younger people. Also, business owners showed the highest vaccination coverage rates among the other occupational groups. This may be explained by the fact that business owners consider their health as a priority to accomplish their work. In addition, patients with concomitant chronic diseases showed a high coverage rate, where diabetic patients showed the highest. Finally, the rate was significantly higher among HCW than non-HCW. This difference is not surprising since healthcare personnel are considered at high risk and are committed to apply safety measures. In addition to the fact that a major proportion of HCW participants work in the government sector and are offered the influenza vaccine free of charge.
Low influenza vaccination rates are a worldwide public health problem and vary from region to region. Reports from the United States, Europe, and Korea have highlighted a coverage rate ranging between 15% and 63% and the Jordanian rate is relatively fitting within this range. In the United States and Europe, the Centers of Disease Control and Prevention (CDC) have conducted several studies on this subject. In 2013, the CDC in the United States reported that the vaccination coverage from 2007/2008 through 2011/2012 influenza seasons in adults increased from 33% during 2007/2008 to 38.3% during the 2011/2012 season (20). Also, the CDC in the United States reported that influenza vaccination coverage in the 2011/2012 season varied by age and risk group. Adults of 65 years of age or older showed the highest vaccination coverage rates, but remained low and relatively stable over the past five seasons through 2011/2012 (33–39%) as measured by National Health Interview Survey (NHIS), the Behavioral Risk Factor Surveillance System (BRFSS). Vaccination coverage rates for US HCW were found to increase significantly from 47.6% in the 2007/2008 season to 62.4% in the 2011/2012 season as measured by the NHIS.
In EU/EEA countries, the seasonal influenza vaccination coverage rates were estimated by the Vaccine European New Integrated Collaboration Effort (VENICE) survey in 2011/2012 to be only 16.4% for all age groups. The rates for older population (65 years of age or older) and clinical risk groups varied from 36% to 64.1% and from 31% to 45.6%, respectively, depending on the country. The HCW coverage rate was only calculated in one country (Norway) and it was 12% (26).
Another study conducted in Korea by Yang and Cho (35) indicated variable coverage rates from 46.5% in 2008/2009 to 56.1% in 2011/2012 for all age groups, with an increase in coverage in the elderly group.
These results are in line with our findings where HCW, adults with chronic diseases, and elderly people showed high coverage rates compared to the general population. However, the overall coverage rates in the Jordanian population were very low compared to those in the United States, Korea, and to a lesser extent in the EU/EEA countries during 2011/2012 and between 2008 and 2012. The low coverage rates in Jordan would imply that the population is either not aware of the importance of the vaccine or it is not their main consideration.
In the vaccination season of 2009/2010, a new vaccine (H1N1 pandemic influenza vaccine) was developed. Vaccination coverage rates worldwide relatively increased during the pandemic year 2009/2010 and declined afterward (34). This was consistent with our results, which explain the higher vaccination coverage rates for all studied groups of the Jordanian population through the 5 years 2008–2012 compared to the study season 2011/2012 vaccination coverage rates. Conversely, during 2011/2012, the need for seasonal and pandemic influenza vaccines was much less than in the pandemic year 2009/2010. This explains the low coverage rates of vaccination in our study season 2011/2012.
The level of knowledge of the Jordanian population about the influenza vaccine
Knowledge of the Jordanian population about the influenza vaccine was found satisfactory with an average score of 80%. HCW respondents' knowledge score was significantly higher compared to non-HCW. In general, both groups were knowledgeable regarding influenza disease, ways of protection, its complications, and the role and effectiveness of the vaccine. In this respect, HCW showed significantly higher scores. On the contrary, non-HCW were uncertain, with little knowledge about the benefits and side effects of the vaccine. They also felt uncertain and showed little knowledge about the vaccine's effect on the immune system and the role of the immune system in increasing the efficiency of the vaccine. In the meantime, HCW agreed that they feel very informed about them all. This is in agreement with other studies. Ofstead et al. (27) showed an average score of 74% of correct responses among HCW in the United States, whereas Khazaeipour et al. (17) reported an average score of 51% among HCW in Iran. These scores are expected due to the HCW educational and professional background.
Apart from HCW, the sources of knowledge vary among Jordanians, with family and friends being the main source to know about the vaccine. This is followed by the media and the Internet. This indicates weak governmental promotion and support or defective/absence of awareness campaigns that involve influenza vaccine. With the increasing role that can be played by telemedia, national campaigns are recommended to cover a wide range of social media and technology means. Compared to the United States, a community assessment conducted in North Carolina about H1N1 influenza vaccine knowledge showed that different media means were the source of information for the vast majority of people followed by the Internet and family and friends (9).
From our study, we were very surprised to know that only 56% of HCW participants learnt about influenza vaccine through their educational degree, which means that this vaccine is somehow neglected by many health sciences schools at the college or university level. In the United Kingdom, there was a strong link between lack of knowledge among qualified nurses and their behavior in refusing the vaccine or of being never vaccinated (37). This fact would imply that the education system of health sciences schools is to be blamed for the lack of knowledge and the low coverage rates of vaccination with this vaccine.
The Jordanian attitudes, beliefs, and practices toward influenza vaccination
In Jordan, no regular vaccination awareness campaigns are available and our study revealed that individuals depend mostly on their physicians regarding the vaccination strategies. In contrast, the majority of the Jordanians understand that the best season for receiving the vaccine is autumn and they believe that it would protect them for a whole year. Also, they believe that vaccination is effective and vital for protection from influenza infection, while with adequate precautions it would not be needed.
A number of factors were found to influence Jordanian attitudes, beliefs, and practices toward influenza vaccine. Lack of awareness is one of the factors that affect the Jordanian attitudes negatively toward the vaccine. Also, adverse effects, cost of the vaccine, and misperception about efficacy of the vaccine were among the main factors influencing their attitudes and practices toward not receiving the vaccine. Conversely, friends and family endorsement and encouragement are other factors influencing their attitudes positively toward receiving the vaccine. Personal experiences were also significant in our study, where a positive or a negative experience influenced the participants' decisions to receive or reject the vaccine in addition to affecting their beliefs. Those who do not believe in the vaccine efficacy must have experienced or witnessed negative effects of the vaccine in themselves or in others they knew. The majority of the participants believe that receiving the vaccine at the wrong time of the year and the ability of the influenza virus to develop new strains are the major reasons for making the vaccine ineffective. However, being under long-term medications will not stop them from receiving the vaccine. Having a chronic health condition was also positively associated with vaccination.
The majority (81.2%) of the non-HCW who did not receive the vaccine previously believed that they have to follow their physicians' advice regarding vaccination. This indicates that Jordanian physicians hold part of the responsibility for the low coverage rates and the negative attitudes toward the vaccine. This was more obvious in people with chronic diseases, where only one-third of them (p = 0.001) were advised by their physicians to receive it although they are considered at higher risk of having the disease complication. Both HCW and non-HCW, who previously received the vaccine, agreed to receive it to protect themselves and people around them and believe in the vaccine efficiency. Those HCW participants showed significantly better attitudes and beliefs than the non-HCW participants. They were more aware of the vaccination time, efficacy, side effects, and the role of the immune system during infection and vaccination. The majority of the non-HCW depend on their physicians' advice regarding receiving or not receiving the influenza vaccine when they or a family member get flu with serious complications, while HCW take immediate action.
The mean attitude score for the Jordanian population was 71%. This indicates a reasonable attitude toward the influenza vaccination safety, necessity for students, medical field workers, elderly, and pregnant women. Although the general attitude score of HCW and non-HCW was almost similar, HCW were more certain about the safety and necessity of the vaccine. These results can be linked to the educational and practical background of the HCW.
Our results were almost similar to previous studies (16,18,30,33,36). Positive attitudes toward vaccines with concerns about the burden of illness and confidence in the vaccines were indicated by the Canadian public and healthcare providers in a very recent study conducted by MacDougall et al. (22). They indicated that between 55.0% and 59.7% of adult participants were willing to receive the vaccine if recommended by their physicians. They also found that healthcare providers were more aware of disease burden and confident in vaccine effectiveness than the public. In addition, they showed that 48% of the Canadian public agreed about the importance of the vaccine to children (22). The National Immunization Coverage Survey conducted in Canada found that many Canadians (65%) prefer to obtain vaccination information from a HCW, whereas 28% of the Canadian adults preferred media, Internet, and publication sources (29). Same results were found in the United States, where 87% of the survey participants were likely or somewhat likely to get adult vaccines if recommended by their doctors (23). Having a chronic health condition was also positively associated with vaccination, this was also reported in other studies (17,24,29,30).
Barriers against and reasons to receive the vaccine
Our results revealed that the major barrier preventing the previously unvaccinated participants from receiving the vaccine was their fear from side effects and doubts of effectiveness. Unsurprisingly, this also applies to HCW, which could be due to lack of awareness and knowledge at the educational and professional levels. The other important barriers to all participants were “forgot” or “too busy to receive it,” while availability and cost were the least barriers…
Similar barriers were seen in other populations worldwide. Healthcare persons in the United States indicated that the reasons for not getting the vaccine include their fear from getting the disease from it, their doubts about its effectiveness, and their belief that they do not need it (4). A surveillance conducted by the CDC in the United States through 2007–2012 (21) had revealed that the major barriers that prevented women from receiving the vaccine were safety concerns followed by doubts about its effectiveness. Another survey conducted on qualified nurses in the United Kingdom showed similar trends in the barriers where fear from side effects, their belief that they do not need it, and concerns about its safety were the three major barriers against receiving the vaccine (37). Moreover, the European Centre for Disease Prevention and Control (ECDC) indicated that low perception of risk from the disease, fear from side effects, cost, availability and convenience, and lack of accurate information about the vaccine were the main barriers against receiving the vaccine (13).
The influenza vaccine coverage rate is decreasing in high- and middle-income countries where Jordan is not an exception (25). The barriers against receiving the vaccine among Jordanians are almost the same as those observed worldwide. Such barriers are believed to encourage vaccine hesitancy that led to the refusal of vaccination and hence reduction of the vaccine coverage rates (5,12). Therefore, to overcome these barriers and increase uptake, it is recommended to increase the awareness and knowledge through vaccination campaigns and media coverage.
In contrast, the main reasons that encouraged our participants to receive the vaccine were the easy spread of the virus in the air and in crowded areas and this followed by the willingness to keep healthy and avoid spreading flu to others. Our results were consistent with those reported among vaccinated HCW in the United States during the 2013/2014 influenza season, where “to protect themselves from flu” was the most common reason (4).
Factors associated with receiving the influenza vaccine
Univariate results in our study showed that age, marital status, residence location, or number of family dependents did not significantly predict whether our participants would receive influenza vaccine or not. Whereas university education and a monthly household income of JD 350–700 ($500–$1,000) increased vaccination rates. Being a male, business owner, or an employee positively increased vaccination rates, while the cost of the vaccine negatively affected the coverage rates. However, using the logistic regression model, the university education did not show a significant correlation (OR = 1.2, p = 0.45). HCW versus non-HCW also affected vaccination coverage rates, where working in the healthcare sector increased vaccination rates. This was relatively similar to other studies showing influenza vaccination to be not significantly associated with age, sex, having children at home, or shift pattern (6,17).
Strengths and limitations of the study
The major strength of our study resides in the fact that it was the first one to include a large sample size of participants conveniently approached and recruited from the general population across the country from different locations and to report on their seasonal vaccination knowledge, attitudes, and practices. It also included both HCW and general public, thus enhancing generalizability of the study findings. On the contrary, there are a number of limitations that merit discussion. First, participants self-reported vaccination history, which was subject to their recall errors. This could influence the accuracy and reliability of the coverage estimates.
However, some studies found a very good agreement between self-reported and medical records for influenza vaccination status (19,38). Unfortunately Jordan has no national medical records for the influenza vaccination status as the case in other countries (5), therefore we had to depend on the self-reported vaccination history. Second, our evaluation focused on participants from Amman and central Jordan and university students. Amman, the capital of Jordan, occupies almost 40% of the Jordanian national population (23) from where we had the largest number of respondents. Selection and information bias was minimized by approaching the study sample in different locations and cities in Jordan. In contrast, the bias in this study could be attributed to low study sample from south and rural areas in Jordan. However, the demographics of the study participants showed distributions well among age, occupation, and monthly household income categories.
Conclusion
The present study is the first to report the rates of vaccination among the adult Jordanian population, which were relatively lower than those seen in other countries. The major barrier to abstinence from vaccination is the fear from side effect.
The current results therefore emphasize the compelling need for professional awareness campaigns to educate and spread public awareness in Jordan regarding the efficacy and benefits of seasonal influenza vaccination. In addition, there is a need for the ongoing education of HCW, during their educational degrees or careers, about the vaccine with emphasis on the CDC recommendations to increase the rate of influenza vaccination in Jordan. The campaigns and the educational activities should be aiming at removing barriers to vaccination, misconceptions, and change the attitudes that limit compliance to vaccination. Also, to consider influenza vaccination an ethical responsibility and a subject of patient safety. Thus, understanding the determinants of influenza vaccine hesitancy among the Jordanian population could help the Ministry of Health in Jordan to plan future interventions and polices aiming at increasing the influenza vaccination rates in Jordan.
Footnotes
Acknowledgments
The authors thank the questionnaire respondents who kindly devoted their time to the study and also thank their team of research assistants at the Faculty of Pharmacy for their help in data collection and entry. The authors also thank Mr. Mashhour T. Assaf for his valuable contribution while writing and editing the manuscript. The study was financially supported by the Deanship of Academic Research (DAR) at the University of Jordan.
Author Disclosure Statement
No competing financial interests exist.