
Abstract
Changes of Treg/Th17 cells ratio and their associated cytokines have some correlations with an immune modulatory effect of Telbivudine treatment. The aim of our study was to investigate the role of the dynamic ratio of Treg/Th17 cells in the mechanism of LdT therapy and their relationships with the clinical responses. We detected the frequency and cytokines production of Treg and Th17 cells in 28 hepatitis B envelope antigen (HBeAg)-positive CHB patients at 0, 12, 24, 36, 48, and 96 weeks after initial LdT therapy. LdT could upregulate the frequency of Th17 cells and Th17 cells associated cytokines, downregulated the frequency of Treg cells and level of TGF-β, which leads to the decrease of Treg/Th17 ratio in HBeAg-positive CHB patients. Treg/Th17 ratio at treatment week 36 could independently predict HBeAg seroconversion in the first 2 years of Telbivudine treatment. Telbivudine therapy can decrease Treg/Th17 ratio, which may predict HBeAg seroconversion during treatment.
Introduction
H
Currently, the globally approval of CHB treatment involves only two types of antiviral therapy, nucleo(s)tide analogs (NAs) and standard interferon alpha (IFN-α) or Pegylated interferon α2a (PegIFN-α2a) (19). IFN-α (conventional or pegylated) has been widely reported to inhibit HBV replication through a variety of mechanisms, including immune modulatory effects, which is associated with higher and more durable hepatitis B envelope antigen (HBeAg) seroconversion rates than oral NAs (11).
Telbivudine (LdT), an orally bioavailable L-nucleoside, has potent and specific anti-HBV activity, which is activated by phosphorylation with cellular kinases. The active form of Telbivudine, LdT-5′-triphosphate, can then inhibit HBV DNA polymerase by competing with the natural substrate, thymidine 5′-triphosphate. Effect of LdT-5′-triphosphate incorporation into HBV DNA is DNA chain termination, leading to suppressing HBV replication. Interestingly, LdT achieves a relatively higher HBeAg seroconversion rate in comparison with other NAs in the previous studies, comparable to IFN-α. Therefore, LdT was considered to regulate the host immune system as IFN-α, and some emerging clinical immune research findings have supported this hypothesis, which is mainly associated with restoring CD4+ T-cell responses against HBV virus (15,20,29,35,40,47).
As proved by an HBV model, CD4+ T cells serve as master regulators of the adaptive immune response to HBV (42), which can usually be classified to at least four subtypes on the basis of their signature cytokines and master transcription factors, the two old major subtypes are Th1 and Th2, the other two new subtypes are regulator T (Treg) cells and interlukin-17-producing CD4+ T helper (Th) 17 cells (42). Treg cells, driven by forkhead family transcription factor 3 (Foxp3), are engaged in dominant control of self-reactive T cells, which is mainly through contact-dependent suppression or releasing anti-inflammatory factors (TGF-β and IL-10) on other immune cells such as CD4+ and CD8+ T cells, natural killer (NK) cells, B cells, and dendritic cells, helping the maintenance of immunologic self-tolerance and immune balance (30). In CHB patients, the proportion of Tregs is significantly upregulated in peripheral blood mononuclear cells (PBMC) and liver tissues, which is positively correlated with serum HBV DNA load (29). By contrast, Th17 cells, due to production of interleukin (IL)-17 family cytokines (IL-17A and IL-17F), has been believed as a proinflammatory T-cell subset involved in strong inflammation, which was observed largely accumulated in the CHB livers and increased in CHB PBMC (16,32,41,44). Based on the same origination between Th17 cells and Treg cells, complicatedly, Treg cells could convert into IL-17-expressing cells if cultured in IL-6. Since the close association of their development pathways and the mutual antagonism in immune response, Treg and Th17 cells can act in an interactive manner in CHB patients. Evidenced previously, the frequencies of Th17 and Treg cells, the ratio of Treg cells to Th17 cells, and the level of their associated cytokines can play an important role in the progress and prognosis of HBV infection disease (2,4,11,32,42,45).
Recent data have shown that the clinical response of CHB patients under LdT treatment have some correlations with an immune modulatory effect, focusing on change of Treg and Th17 cells and their associated cytokines (9,40,47). However, the exact role of the dynamic balance of Treg/Th17 cells in the mechanism of LdT therapy and their relationships with the clinical responses is still not fully understood, especially the relatively high HBeAg seroconversion. Thus, we detected the frequency and cytokines production of Treg and Th17 cells in HBeAg-positive CHB patients before and after LdT therapy, intending to further understand the difference between these two closely associated subtypes of CD4+ cells on the regulation of host immune system and better illustrate the two subtypes in the development of CHB patients with LdT treatment.
Methods
Study subjects
A total of 92 untreated adult patients, who were diagnosed with CHB in the West China Hospital of Sichuan University (Chengdu, China), were positive for HBV e antigen (HBeAg), and had serum HBV DNA loads above 5 log10 copies/mL and increased serum alanine aminotransferase (ALT) levels above 70 U/L, were screened between October 2010 and August 2012. Patients were excluded if they were breastfeeding or pregnant, had liver disease caused by conditions other than HBV infection, were with HIV infection, coexisting serious diseases, or advanced liver diseases (including cirrhosis, severe hepatitis, and liver cancer), and were undergoing antiviral or immunomodulatory therapy before the study.
Twenty-eight patients were eventually recruited and analyzed in this study. (Fig. 1.) All of these 28 patients were treated with 96-week LdT monotherapy (Sebivo, 600 mg orally per day; Novartis Pharmaceuticals Ltd.). The baseline clinical data are shown in Table 1.
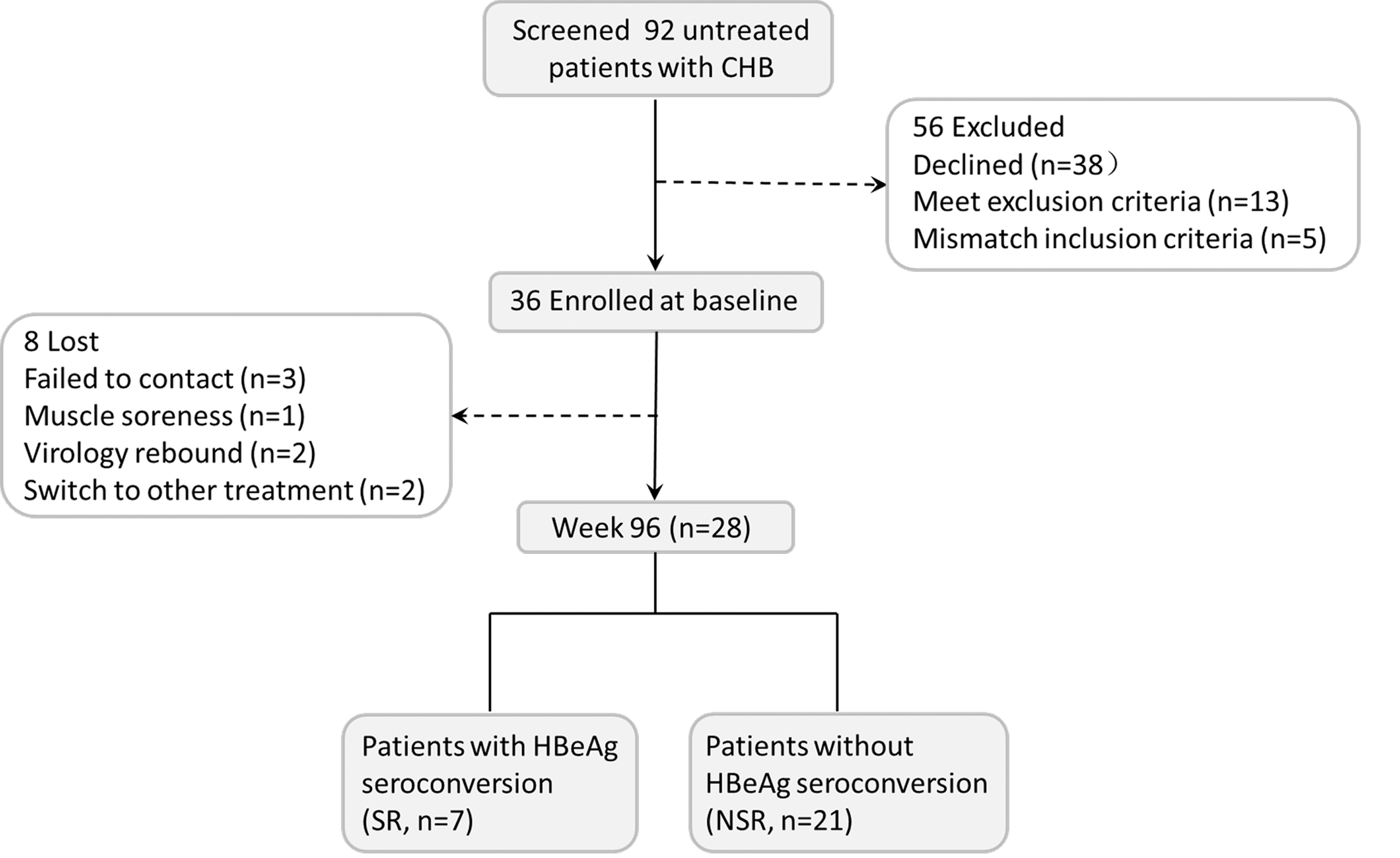
Flowchart of study participants.
Median (range).
Mean (range); otherwise as numbers.
HBV DNA, hepatitis B virus deoxyribonucleic acid; ALT, alanine aminotransferase; HBsAg, hepatitis B virus surface antigen; HBeAg, hepatitis B virus envelope antigen; Anti-HBc, antibody to hepatitis B virus core antigen.
Study design
This was a prospective controlled study, aimed to further understand the exact role of Treg and Th17 cells in the development of CHB patients with LdT treatment. Blood samples were collected from each patient at baseline (0) and 12, 24, 36, 48, and 96 weeks after initial LdT treatment. Adherence to treatment was assessed at each visit.
By week 96, patients achieving HBeAg seroconversion were defined as sero-responders (SR) and patients who failed to achieve HBeAg seroconversion were defined as non-sero-responders (NSR).
All patients wrote their informed consent before participating in the study and the study protocol, following the guidelines of the Declaration of Helsinki, was approved by the Ethics Review Committee of the West China Hospital, School of Medicine, Sichuan University.
Sample preparation and stimulation
Eighteen milliliters of fresh heparinized peripheral venous blood was obtained from each participant. The plasma was isolated from 8 mL of the peripheral blood and stored at −80°C until the concentrations of cytokines were measured. PBMCs were obtained from the other 10 mL of the peripheral blood by Lympholyte-H cell separation media (Cedarlane, CAN) using density gradient centrifugation methods on the basis of the manufacturer's protocol, and they were instantly cryopreserved in medium composed of 90% heat-inactivated fetal calf serum (FBS; Gibco) and 10% dimethylsulfoxide (DMSO; Solarbio) after isolation. The PBMCs were thawed 2 h before the experiments, then cultured at a density of 2 × 106 cells/mL in complete RPMI 1640 (Invitrogen) with 10% heat-inactivated FBS at 37°C under 5% CO2 atmosphere for 1 h. Cell viability was over 85% by trypan blue exclusion. PBMCs were stimulated with phorbol myristate acetate (PMA 50 ng/mL), ionomycin (1 μg/mL; both from Sigma), and Brefeldin A (BFA 1 μg/mL; BD Biosciences Imumunocytometry Systems) in RPMI 1640 with 10% heat-inactivated FBS at 37°C under 5% CO2 atmosphere for 5 h.
Flow cytometric analysis
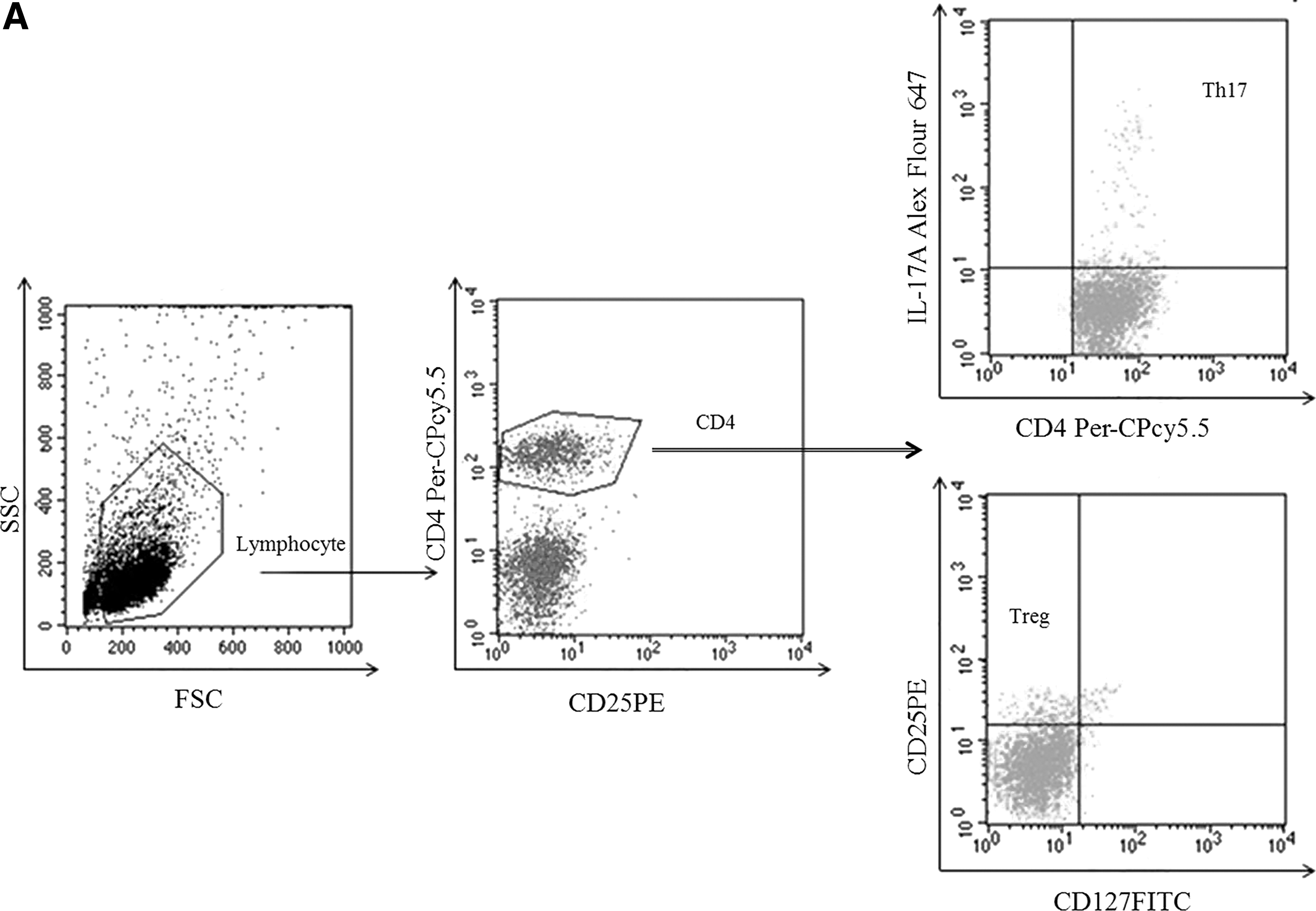
Upon harvest, the cells were transferred into FACS tubes and resuspended in 100 μL of Staining Buffer (BD Bioscience Imumunocytometry Systems) containing anti-CD4-PerCP-Cy5.5, anti- CD127-FITC, and anti-CD25-PE (BD Biosciences), incubated at room temperature in the dark for 15 min. After surface staining, the cells were fixed and permeabilized by adding 500 μL of Fixation/Permeabilization solution (BD Sciences) for 20 min incubation at room temperature in the dark, and then stained with anti-IL-17A-Alexa Fluor 647 (BD Sciences) for intracellular staining. Then, the cells were washed again and resuspended in 500 μL PBS/2% paraformaldehyde solution for flow cytometry analysis. Th17 cells (CD4+IL-17+ T cells) and Treg cells (CD4+CD25+CD127− T cells) were analyzed with flow cytometry (BD FACSCalibur).
Enzyme-linked immunosorbent assays
The concentrations of IL-17A and TGF-β in the plasma were measured using their respective enzyme-linked immunosorbent assays kits according to the manufacturer's instructions (MultiSciences). The absorbance was recorded at 450 nm in a microplate reader (BIO-RAD Laboratories). All samples were repeated three times.
Virological and biochemical assessments
Serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TB), direct bilirubin (DB), indirect bilirubin (IB), and other biochemical indicators were determined by using an automatic biochemical analyzer (Beckman AU5811, Beckman). Hepatitis B surface Antigen (HBsAg), anti-HBs, Hepatitis B envelope Antigen (HBeAg), anti-HBe, total IgM anti-HBc, anti-HAV, anti-HDV, and anti-HCV were analyzed using an Roche Cobas E601 system (Roche Molecular Systems, Inc.). Serum HBV DNA was measured with quantitative fluorescent PCR using commercially available kits (ABI7300; Perkin Elmer) following the manufacturer's instructions. The detection limit of HBV DNA is 500 copies/mL.
Statistical analysis
All data were analyzed with SPSS version 18.0 (SPSS, Inc.). Categorical variables were expressed as numbers, asymmetric data were shown as median (min-max), and continuous data were expressed as mean ± standard deviation (SD). χ 2 analysis, Student's t-test, one-way ANOVA, Wilcoxon rank sum test, Kruskal–Wallis H test, Mann–Whitney U test, Pearson correlation and receiver operating characteristic curve were properly performed. p < 0.05 (two-tailed) was considered statistically significant for all tests.
Results
Clinical outcomes
The viremia of all 28 patients exhibited a rapid decline to a low or undetectable level at week 12, which stayed through the treatment course (Fig. 2). However, HBeAg level showed two sharp declines respectively at week 12 and week 36. As shown in Table 2, the SR, and NSR respectively represented 7 (25%) and 21 (75%) patients in the sample of 28. The age, ratios of gender and HBV genotype, HBV DNA load, and levels of HBeAg, HBsAg, and ALT were similar at baseline between the two groups. After 96 weeks of telbivudine monotherapy, serum HBV DNA levels were undetectable (the detection limit is 500 copies/mL) in 21 of 28 patients, 7 in the SR and 14 in the NSR. There was a significant difference in serum levels of HBsAg between SR and NSR at week 48 (p = 0.044), week 96 (p = 0.027). A loss or remarkable reduction of HBeAg was observed in 25 patients, and 10 of these patients had the appearance of anti-HBe. HBsAg loss was not achieved in any of the 28 patients but 1 in the NSR obtained anti-HBs. In accordance with profound suppression of HBV replication, ALT levels of these 28 patients was significantly reduced beginning at week 12, compared with the baseline (p = 0.000), which suggested that liver inflammation was largely alleviated. At week 96, normal ALT was found in 5 of SR, 11 of NSR.
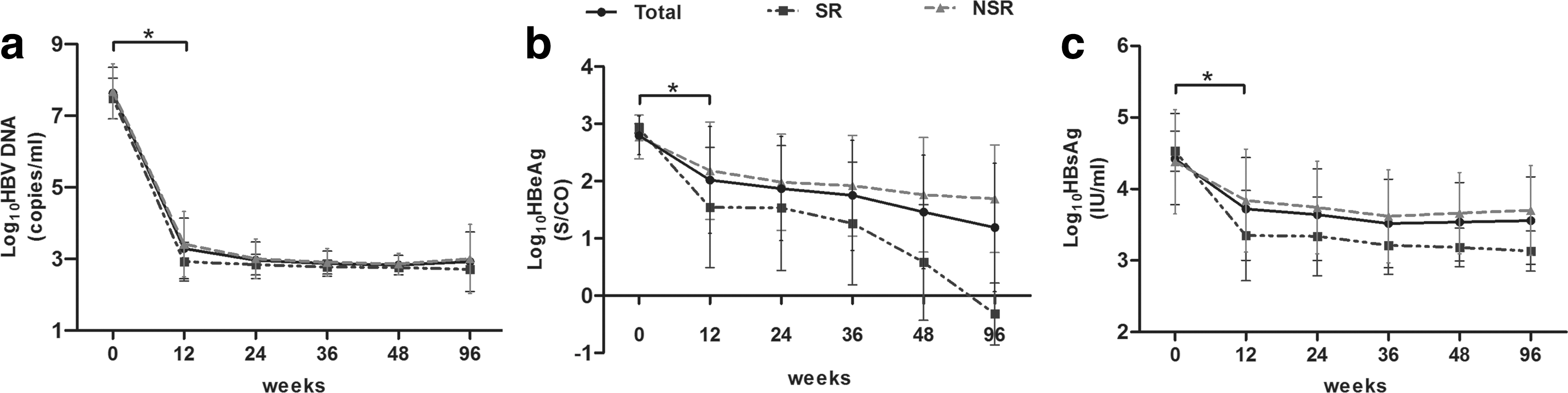
The changes of HBV DNA
Data shown are mean ± standard deviation, median (range), or expressed as numbers, unless otherwise indicated. p-Values indicate the comparison among SR and NSR groups, presenting in bold when p < 0.05. One-way ANOVA and χ 2 analysis were used as appropriate. SR, a seroconverse-response to TdL treatment; NSR, a nonseroconversion to TdL treatment; Week, treatment week.
Different responses of Treg and Th17 cells in SR and NSR groups during Telbivudine monotherapy
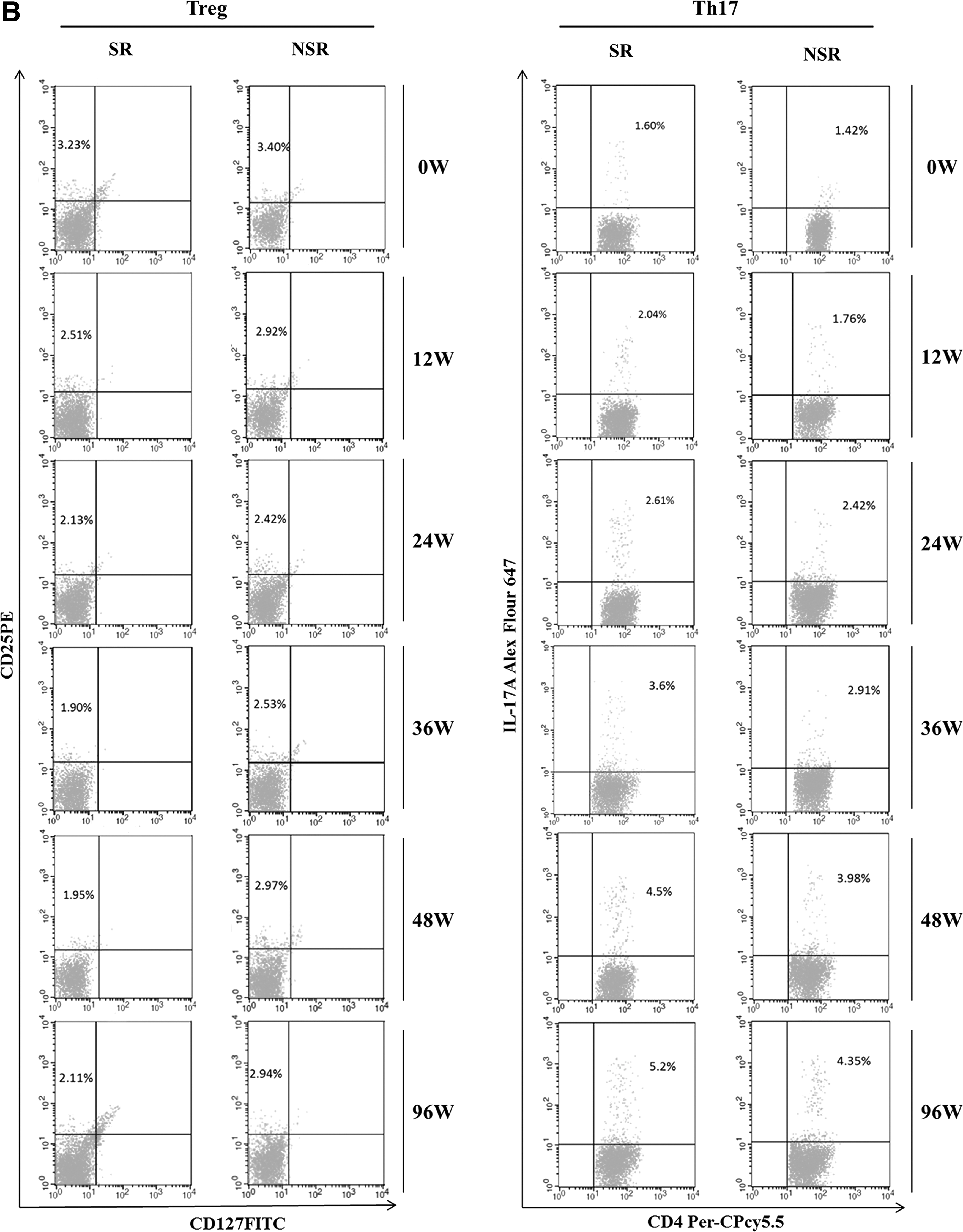
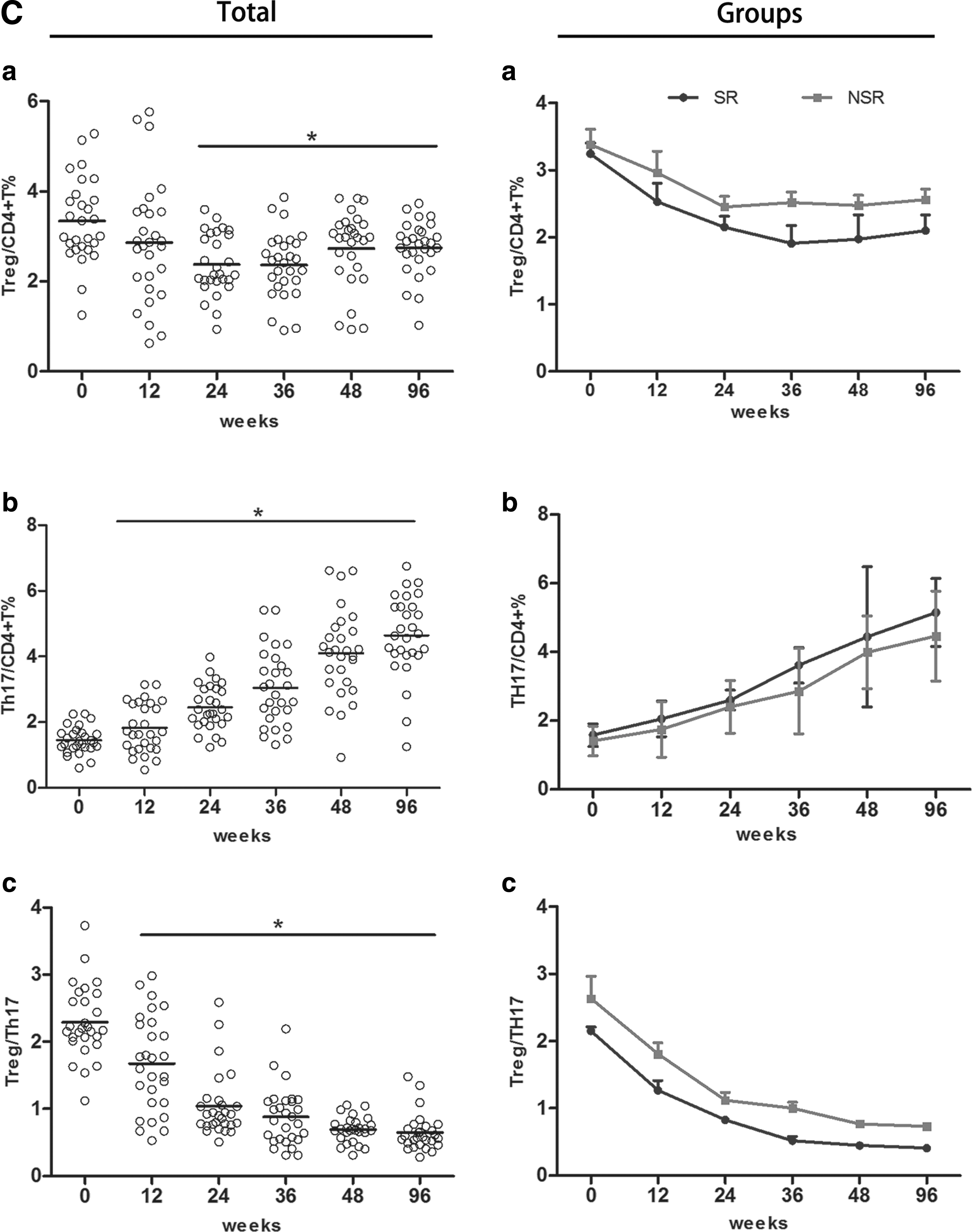
As shown in Figure 3C, results showed that, both in SR and NSR, Treg frequencies decreased in general with twice mild increases while Th17 frequencies consistently increased throughout the 96 weeks. For SR, Th17 frequencies achieved the highest point at week 96 and Treg frequencies got the lowest point at week 36. Also, NSR had Th17 frequencies peaked at week 96 but frequencies of Treg being lowest at week 24. When we compared SR with NSR, we observed that SR exhibited a higher Th17 frequency and a lower Treg frequency, despite the nonsignificant manners, consequently leading to a continuously decreased Treg/Th17 ratio with significance since week 36. Representative flow cytometric analyses of Treg and Th17 cells were shown in Figure 3B.
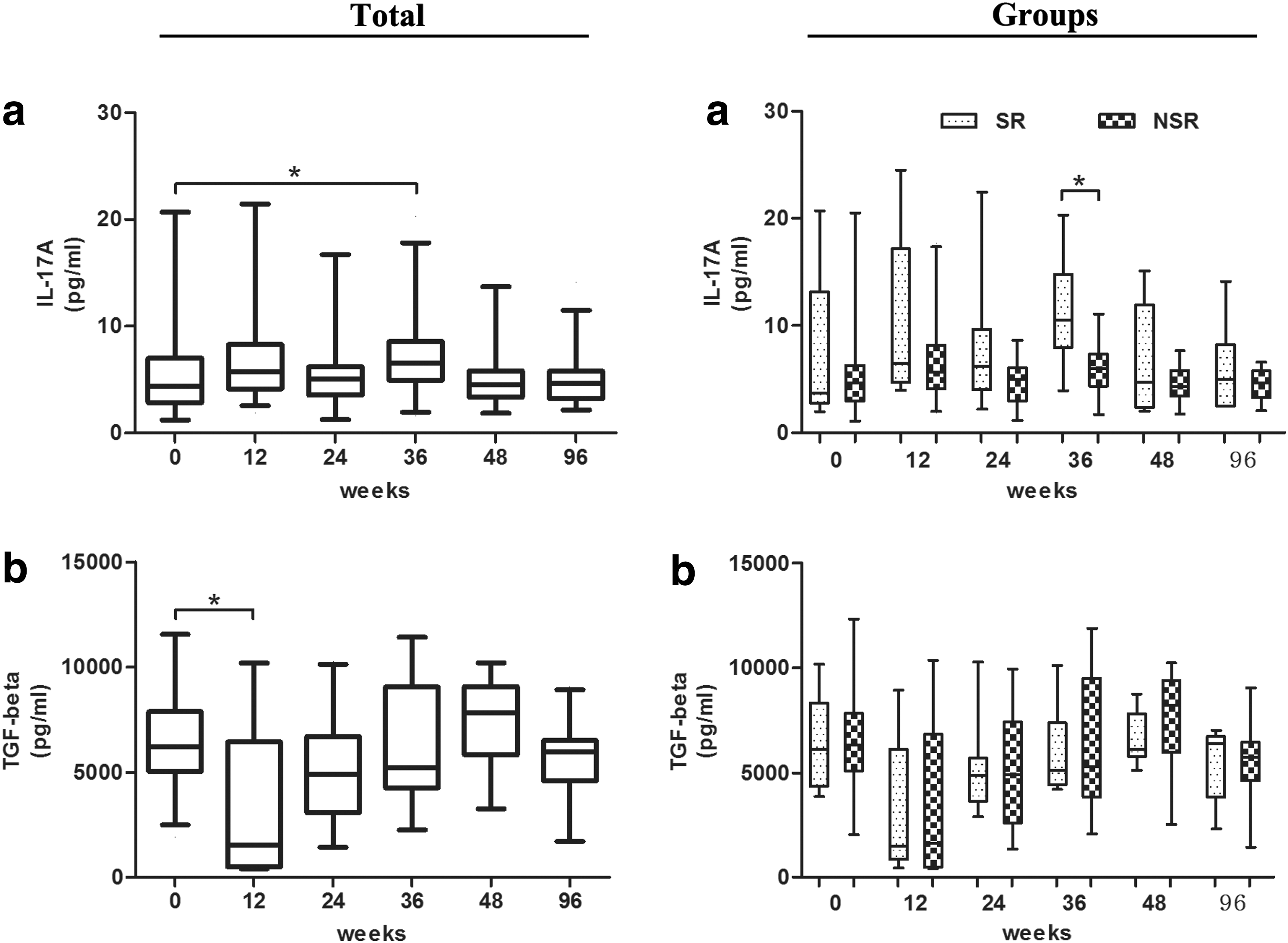
Alteration of IL-17A and TGF-β serum levels in response to Telbivudine treatment
To find out the role of cytokines associated with Treg and Th17 cells, we detected two subgroups: Th17 secreting cytokines IL-17A and Treg differentiation cytokine TGF-β. As shown in Figure 4a, IL-17A levels were notably increased until week 36 and subsequently reduced during the period, which were markedly higher in SR than NSR at the same time point. Given the results above, it is demonstrated that LdT had been conductive to the expression of Th17. However, a significant reduction of TGF-β was observed at week 12 and 24; then it gradually increased till the end of treatment. Moreover, the levels of TGF-β were lower in SR than in NSR, but these differences failed to achieve significance (Fig. 4b).
The concentrations of IL-17A
Correlation between therapeutic responses and the ratio of Treg to Th17 cells in HBeAg-positive patients with Telbivudine therapy
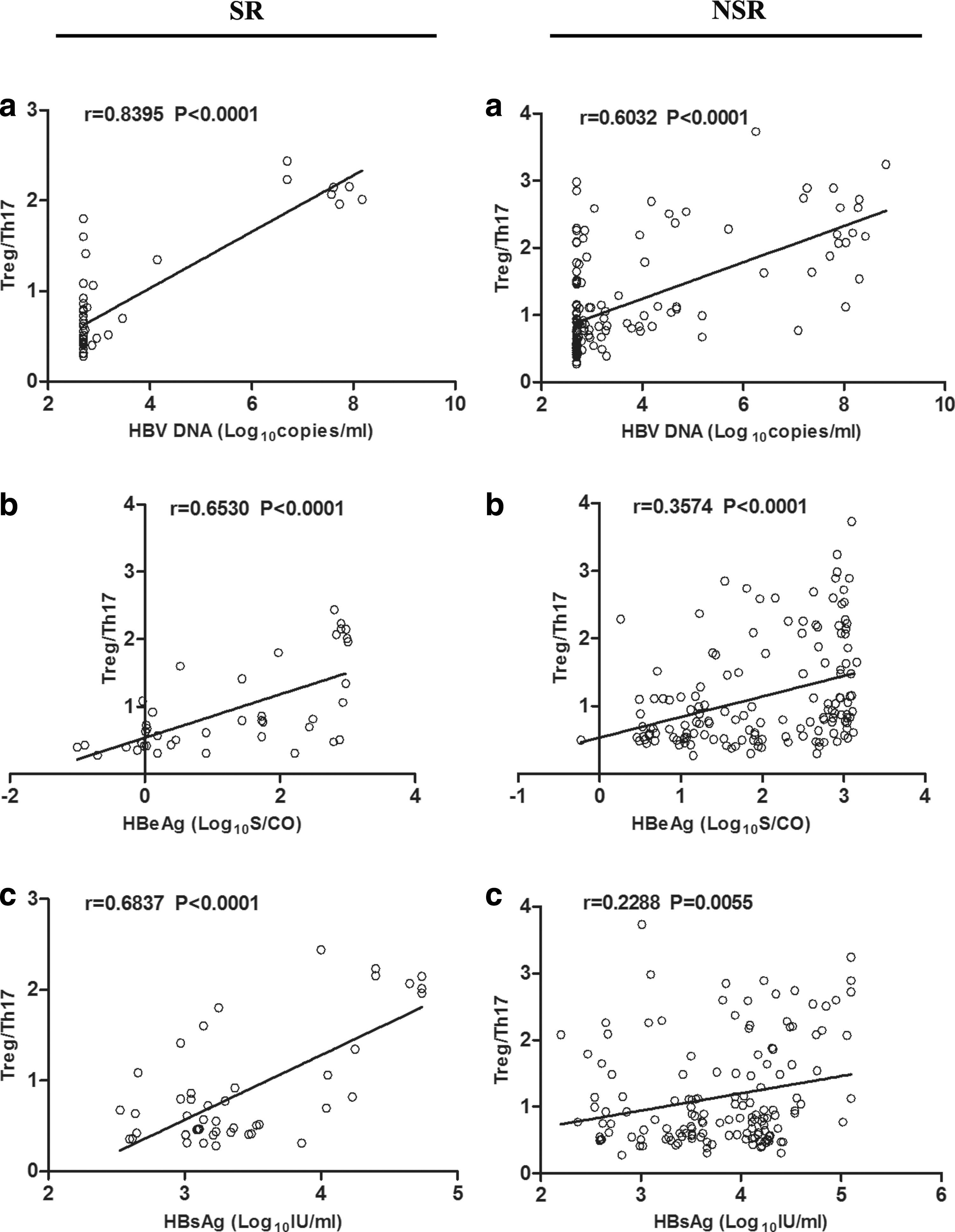
To further determine the association of therapeutic responses with Treg/Th17 ratio, we analyzed correlations between HBV DNA loads, HBeAg, HBsAg levels, and Treg/Th17 ratio before and until the treatment course ended.
Results showed that (Fig. 5), in the relations to HBV DNA loads, Treg/Th17 ratio showed an obviously positive correlation in both groups. However, the correlation was much tighter in SR than NSR. Moreover, the correlation between HBV DNA loads and Treg/Th17 ratio is the strongest. For HBeAg levels, there was significantly positive correlation between it and Treg/Th17 ratio, which existed only in SR group. Similarly, we found that HBsAg levels positive correlated with Treg/Th17 ratio, existing only in SR.
Correlations between the Treg/Th17 ratio and HBV-DNA
Relationship between the ratio of Treg to Th17 and HBeAg seroconversion
HBeAg seroconversion implies serological response, which defines as HBeAg loss and seroconversion to anti-HBe. Based on the results above, the balance of Treg and Th17 were closely correlated with therapy responses. Then, we performed some analyses between the Treg/Th17 ratio and HBe seroconversion. In this 96-week LdT monotherapy, there were seven patients (SR group) who had achieved HBeAg seroconversion. These seven patients respectively obtained HBeAg seroconversion at week 36 (two patients), week 48 (five patients).
Univariate analysis showed that Treg/Th17 ratio was significant at Week 36, 48, and 96 between SR and NSR. Logistic regression analysis found independent effect of Treg/Th17 ratio only at week 36 (p = 0.020). Receiver operating characteristic curve was produced to assess the use of 36 weeks to predict HBeAg seroconversion at 96 weeks (Fig. 6). The optimal cut-off value for 36-week Treg/Th17 ratio was 0.6797, which gave a sensitivity for detection of HBeAg seroconversion of 85.7% and specificity of 76.2%. A frequency of 36-week Treg/Th17 ratio less than 0.6797 gave a positive predictive value for complete response of 95%.
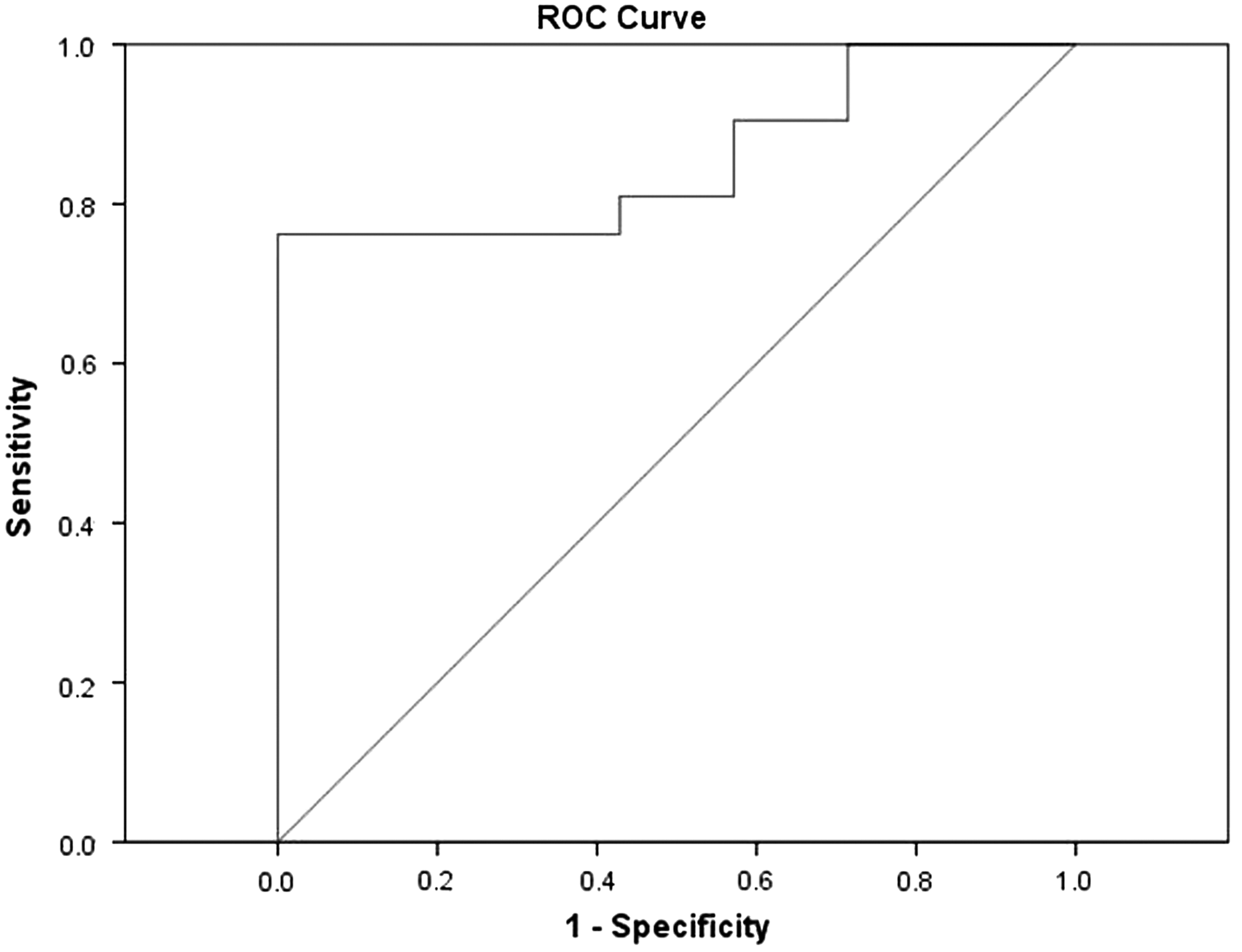
Receiver-operating characteristic curves displaying the effect of 36-week Treg/Th17 ratio on the possibility of achieving HBeAg seroconversion to LdT therapy. An AUC of 1.0 is characteristic of an ideal test, and an AUC <0.5 indicates a test of no diagnostic value. AUC, area under the curve.
Discussion
In HBeAg-positive patients, the primary end point of antiviral therapy is sustained off-therapy virological remission with HBeAg seroconversion, which is not always achievable in some patients. This is why those patients who do not successfully achieve HBeAg seroconversion have to undergo a lifelong drug therapy to suppress viral replication. Thus, it is an important and intricate issue how the underlying mechanisms between the virus and host immune promote HBeAg seroconversion. Among available NAs for HBV therapy to now, what makes Telbivudine distinctive from other NAs is the high rate of HBeAg seroconversion, which benefits from both direct antiviral effcts and immunoregulatory functions.
Here, in our study, 96 weeks treatment of LdT showed potent abilities to inhibit HBV replication, normalize ALT, reduce HBsAg levels, and achieve high rate of HBeAg seroconversion, consistent with previous studies (10,12 –14,18). As identified in other researches (6,22,23,37,38), high ALT levels at baseline and rapid HBsAg decline during treatment are the predictors of HBeAg seroconversion, which is demonstrated again in the SR group of our study. In addition, HBV genotype plays no role in the virological response to LdT.
Immunoregulatory functions of LdT have attracted much attention and many studies suggested that early host immune restoration under LdT therapy may partly report and even predict the long-term responses to antiviral therapy (5,6,21). The balance between Treg and Th17 cells can mediate inflammation and may contribute to the progression of HBV-infected diseases, demonstrated in several researches (5,25,26,46). However, the studies above fail to provide longitudinal changes of Treg and Th17 cells during LdT long-term monotherapy, especially analysis of the relationship between Treg/Th17 ratio and LdT-induced HBeAg seroconversion. Here, we detected frequencies and cytokines production of Treg and Th17 cells during 96-week LdT monotherapy.
The important ability of Treg cells is to keep immune tolerance against antigens. The immune function of Treg cells mainly depends on secreting cytokines of TGF-β. A higher frequency of Treg cells was observed in CHB than healthy controls (17,29,31,33,39), which can indirectly prove that CHB is characterized by impaired immune response to HBV. Several studies have demonstrated that the frequency and function of Treg cells is significantly decreased by LdT treatment in CHB (24,29,47). Here, in our study, both the frequency of Treg cells and the levels of TGF-β were significantly decreased over 36 weeks of LdT treatment and then slightly increased after 48 weeks of this treatment. Concomitantly, the levels of HBV DNA rapidly decreased over 36 weeks of treatment and then almost maintained. The results indicate that, after LdT therapy, the rapidly and sharp reduction of HBV DNA loads could weaken the immune tolerance by decreasing Treg cells and TGF-β levels. Meanwhile, the frequency of Treg was positively correlated with serum HBV DNA loads, HBeAg, HBsAg, and ALT levels (data not shown), which suggests that Treg cells are closely associated with the progress of HBV infection.
Th17 cells, which shared the same signaling pathways of cell differentiation with Treg cells, have gained much insight into its participation in clearance of HBV (8,36,43). Th17 cells secrete IL-17A at the early start of the inflammatory response. We found that Th17 cells frequency were steadily increased over 36 weeks of treatment and obviously upregulated after 48 weeks of LdT treatment. IL-17A levels increased before 36 weeks and then downregulated after 48 weeks of the treatment. The frequency of Th17 was negatively correlated with serum HBV DNA loads, HBeAg and HBsAg levels (data not shown). All these findings suggest that Th17 cells are involved in the antiviral therapy process of CHB and may play an important role in the viral clearance.
The Treg/Th17 ratio is closely related to the inflammation control (48) and may be a potential marker for assessing the severity of some human infectious diseases (27). In this study, we found that favorable responses are particularly correlated with early and significant downregulated Treg/Th17 ratio responses, as shown in SR group. The low Treg/Th17 ratios, and the low frequencies of Treg cells and high frequencies of Th17 cells, raise the possibility that ratio of Treg/Th17 cells is a component of the immune responses associated with HBeAg seroconversion and valid control of HBV replication. This would be consistent with some recent studies in which lower Treg/Th17 ratios were found to have a positive role in the complete response of CHB patients with positive HBeAg (20,32,45). The ratio of Treg/Th17 cells was tightly positively correlated with serum HBV DNA loads, HBeAg, and HBsAg levels. We found that ratio of Treg/Th17 cells at 36 treatment week independently predicted HBeAg seroconversion in the first and half years of Telbivudine treatment and the optimal cut-off value for 36-week Treg/Th17 ratio was 0.6797, which gave a sensitivity for detection of anti-HBe seroconversion of 85.7% and a specificity of 76.2%.
The changes in the frequencies of Treg and Th17 cells and the levels of related cytokines at different times during treatment had been measured, they would help to explain the role of Treg/Th17 cells and related cytokines in T-cell immune reconstruction after antivirus treatment. After LdT antivirus therapy, the T-cell immune response, in which Th17 cell frequency and IL-17A levels had increased, was partially restored. Meanwhile, the frequency of Treg cells was decreased, and the suppression function was weakened. Because the balance of Treg/Th17 was skewed toward Th17 cells, the immune inflammatory response may be beneficial to clearing HBV. In the early stage of immune clearance in HBeAg-positive patients, the frequency of Treg cells remains high and helps to maintain immune tolerance. HBeAg is the main factor mediating immune tolerance associated with Treg cells. These observations may be the reason for the different observed correlations between the Treg/Th17 ratio and treatment response.
There is still need to identify reliable on-treatment markers that can predict the outcome of antiviral therapy for CHB in individual patients. The Treg/Th17 ratio at treatment week 36 not only independently predicted HBeAg seroconversion in therapy, but also can be able to identify the patients where a low ratio of Treg/Th17 cells had a 85.7% positive predictive value for HBeAg seroconversion. However, the sample size of our study is the limited factor. This observation needs to be confirmed in a larger group of patients, and bingding Treg/Th17 ratio with HBV-DNA levels, HBeAg concentrations, and ALT levels to obtain an index for treatment response in a larger sample size should be explored. In addition, the viral genetic and host immune mechanisms that drive HBeAg seroconversion have not yet been fully understood. This is an important and difficult issue because available antiviral drugs that potently suppress HBV replication to very low levels in CHB patients do not always induce HBeAg seroconversion, although the liver inflammation is controlled. The result of this is that CHB patients who do not achieve HBeAg seroconversion are committed to the expense and inconvenience of lifelong drug therapy.
Conclusion
Our study showed that LdT could upregulate the frequency of Th17 cells and Th17 cells associated cytokines, downregulated the frequency of Treg cells and level of TGF-Beta, which leads to the decrease of Treg/Th17 ratio in HBeAg-positive CHB patients. Treg/Th17 ratio at treatment week 36 could independently predict HBeAg seroconversion in the first 2 years of Telbivudine treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.