
Abstract
Epstein–Barr virus and vitamin D both have been implicated in the pathogenesis of autoimmune diseases, especially multiple sclerosis (MS). Vitamin D influences both innate and adaptive immune responses and has been linked to increased susceptibility to other viral infections such as influenza. Here we aimed to examine the association between vitamin D and acute infectious mononucleosis (IM).This study is a case–control study that was conducted on IM patients and a control group of healthy individuals at infectious disease clinics of Isfahan University of Medical Sciences. Patients were recruited from January to December 2014. The viral capsid antigen (VCA) IgM titer and vitamin D levels were measured at the time of acute infection in IM patients. We also measured vitamin D levels in healthy controls recruited during the same period of time. A total number of 60 IM patients with the mean age of 23.26 ± 7.59 and a healthy control group with the mean age of 25.13 ± 6.72 were enrolled. In the IM patients, there was no significant association between 25(OH) D3 levels and VCA IgM titers (r = 0.190, p = 0.146). Mean 25(OH) D3 levels in IM patients were significantly lower than in the control group (15.61 ± 9.72 vs. 21.41 ± 12.64, p = 0.006). Our findings showed significantly lower vitamin D levels in IM patients at the time of infection than in the control group, providing some evidence that the two major risk factors for autoimmune diseases (e.g., MS) might not be independent risk factors.
Introduction
E
In addition to certain malignancies, EBV infection has been linked to a number of autoimmune diseases such as systemic lupus erythematosus, rheumatoid arthritis, and multiple sclerosis (MS) (2,11,12). The effect of EBV infection and autoimmunity has been postulated to be mediated by immunological cross-reactivity between EBV and self-antigen (molecular mimicry) (14,17), and most recently by EBV-infected autoreactive B-cell hypothesis of autoimmunity, which proposes that B cells infected with EBV are seeded in the target organs where they produce antibodies that cause survival of autoreactive T cells in genetically susceptible individuals (16).
Vitamin D has been shown to have immunomodulatory effects that influences both innate and adaptive immune responses. The role of vitamin D in the pathogenesis of autoimmune diseases remains elusive. However, it is proposed that vitamin D may control cellular function and proliferation of immune cells by regulating the gene expression, resulting in mediation of Th-2 response, suppressing the Th-1 response and inducing T regulatory (T-reg) cells (10,20).
Given that both vitamin D deficiency and EBV infection are risk factors for autoimmunity especially MS (1), understanding the relationship and interaction between these two factors seems imperative. We aimed to evaluate serum vitamin D levels in patients with infectious mononucleosis (IM) (symptomatic EBV infection) and compare them with healthy control group in Isfahan, Iran.
Materials and Methods
This study is a case–control study that was conducted on patients who were diagnosed with IM at infectious disease clinics of Isfahan University of Medical Sciences in Isfahan, Iran. Patients and controls were recruited from January to December 2014.
IM, infectious mononucleosis.
The diagnosis of IM was based on clinical presentations and was confirmed with serological EBV testing. Patients with clinical symptoms and signs of the disease (fever, lymphadenopathy, pharyngitis, and other constitutional symptoms) and positive viral capsid antigen (VCA) IgM who did not use any form of vitamin D supplementation during the past 6 months were enrolled in this study. A control group of healthy volunteers were recruited who had never had a history of IM and also did not take any form of vitamin D supplementation.
Serum (25)OH D3 levels and VCA IgM titer were measured using enzyme-linked immunosorbent assay. Blood was drawn during an acute infection and tested for both VCA IgM and vitamin D in IM patients. Demographic data were gathered using a questionnaire.
This study was approved by the local ethics committee and all patients in this study gave written informed consent. Data were analyzed using SPSS 19 software.
Results
A total number of 60 IM patients (F = 31, M = 29) with a mean age of 23.26 ± 7.59 and 60 healthy individuals (F = 36, M = 24) with a mean age of 25.13 ± 6.72 were enrolled. There was no significant difference between the age and gender distribution in these two groups (p > 0.05).
Mean 25(OH) D3 levels (ng/mL) in IM patients was significantly lower than in the control group (15.61 ± 9.72 vs. 21.41 ± 12.64, p = 0.006).
We also categorized participants into three groups based on their vitamin D levels: (i) insufficient (<10 ng/mL), (ii) low sufficient (10–30 ng/mL), and (iii) sufficient (>30 ng/mL). Categorical analysis revealed that significantly less IM patients are in the sufficient group and significantly more IM patients are in the insufficient group.
In the IM patients, there was no significant association between vitamin D levels and VCA IgM titers (r = 0.190, p = 0.146). The distribution of VCA IgM levels and vitamin D levels in the IM population is shown in Figure 1.
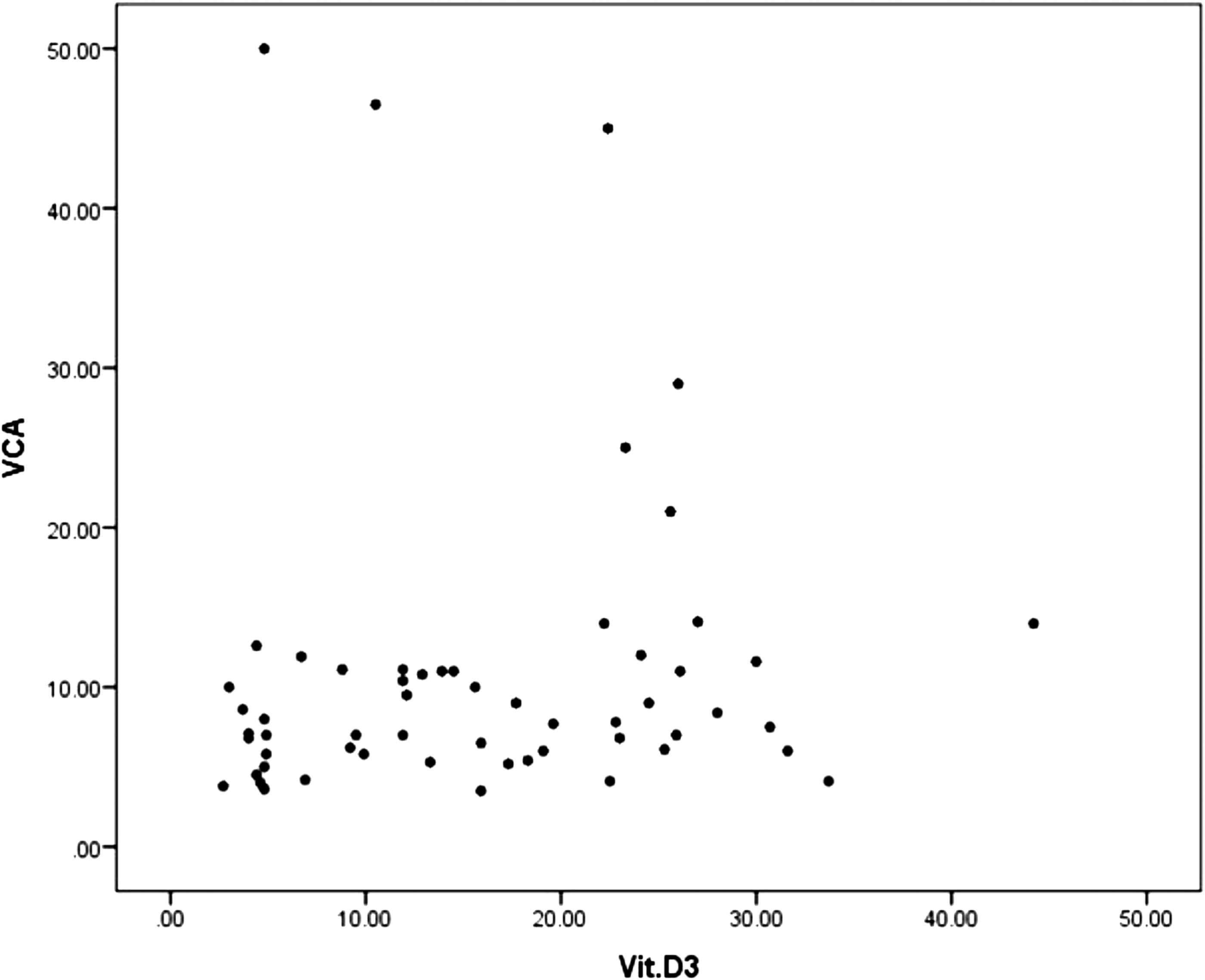
Distribution of VCA IgM and vitamin D levels in IM patients. IM, infectious mononucleosis; VCA, viral capsid antigen.
Discussion
In our study, patients with acute IM had lower levels of vitamin D than healthy controls. It seems that vitamin D deficiency and EBV (IM) that are both risk factors for autoimmunity might interact together; however, the mechanism and direction of such association remains unclear. Vitamin D deficiency has been previously linked to increase the susceptibility to other viral infections such as influenza (4). Further clinical evidence comes from a study that showed that vitamin D supplementation reduces the shedding of EBV in saliva (22). Moreover, in studies conducted on MS patients and control groups, a positive correlation between latitude and EBV seroprevalence was observed independently of MS status (7). Another study on MS patients showed EBNA-1 reactivity decreases in MS patients after vitamin D supplementation (6). The mechanisms in which vitamin D modulates the immune response have been largely debated. T regulatory (T-reg) cells might be a link between vitamin D and EBV infection. T-reg cells on one side play an important role in controlling primary EBV infection (21) and on the other side are induced by vitamin D's effect on secretion of regulatory cytokines (5). Other proposed mechanisms of interaction of vitamin D and EBV could be through cathelicidins, which are a family of proteins induced by vitamin D, with broad antimicrobial activity and thought to play a protective role against EBV infection (9,10). It could also be hypothesized that acute infection with EBV might also cause hypovitaminosis D by consumption of vitamin D.
The EBV antibody titers especially EBNA1 IgG are associated with risk of autoimmune diseases and especially MS (13). However, the studies looking at EBNA 1 IgG titers and vitamin D levels have been inconclusive with some reporting an association and others not (3,15,18,19). However, unlike other studies, we measured VCA IgM and 25(OH) D3 levels at the time of acute infection with EBV, which showed no associations.
Our findings showed significantly lower vitamin D levels in IM patients at the time of infection than in the control group, providing some evidence that the two major risk factors for autoimmunity might not be completely independent risk factors.
Author Disclosure Statement
No competing financial interests exist.