
Abstract
Toxicities related to the use of nucleoside analogues have increased the interest in developing nucleoside-sparing regimens, mainly combining protease inhibitors with raltegravir. However, data regarding the use of CCR5-antagonists in this setting and in the naive scenario are scarce. The main objective was to analyze the immunovirological efficacy and tolerability of a low-dose, once-daily, maraviroc (MVC)-containing, nucleoside reverse transcriptase inhibitor-sparing dual therapy compared with standard triple therapy after 48 weeks for naive HIV-infected patients in the routine clinical practice setting. All naive HIV-infected patients with stable clinical condition that started antiretroviral treatment since February 1, 2008 to May 30,h 2012 were included. MVC clinical test was used to select candidate subjects to MVC therapy. Thirty-two subjects with MVC + atazanavir/ritonavir (ATV/r) and 66 with standard triple therapy were analyzed. A comparable virological efficacy between groups was found after 48 weeks (87.5% vs. 80.3% of HIV undetectability, p = 0.37, MVC + ATV/r and triple therapy groups, respectively). The CD4 recovery after 48 weeks was similar and more than 200 cells/mm3 in both groups. No need of therapy changes or treatment discontinuations was observed in the MVC + ATV/r group. Effect on lipid profile, high-sensitivity C reactive protein, and β2-microglobulin was similar for both groups. Noteworthy, a significant increase of erythrocyte mean corpuscular volume was observed only in the triple therapy group. A nucleoside-sparing MVC-containing dual therapy showed similar immunovirological efficacy and tolerability than standard triple therapy in naive HIV-infected patients.
Introduction
T
Maraviroc (MVC) is an attractive option for NRTI-sparing therapies due to its low toxicity profile and the additional immunological effects reported (2,24,28). MVC belongs to the CCR5 antagonist family, being only active against CCR5 HIV strains (3). Therefore, MVC should be used at the early stage of HIV infection when CCR5 strains are predominant, since the rate of CXCR4 strains dramatically increases in advanced stages (29). However, therapeutic regimens including MVC in naive subjects have been scarcely explored and only in the context of clinical trials (16,18,25), but there are no available studies in the clinical practice setting.
Therefore, the main objective of this study was to analyze the immunovirological efficacy and tolerability of a low-dose, once-daily, MVC-containing, NRTI-sparing dual therapy compared with standard triple therapy after 48 weeks for naive HIV-infected patients in the routine clinical practice setting. Secondary objectives were to analyze the effect on systemic inflammation biomarkers of these therapeutic options.
Materials and Methods
Patients, treatments, and study design
Patients included in this retrospective study belonged to the HIV cohort from the Infectious Diseases Department at Virgen del Rocio University Hospital (Seville, Spain). All consecutive naive HIV-infected patients with stable clinical condition and available stored samples starting antiretroviral (ARV) treatment since February 1, 2008 to May 30, 2012 were included. Every patient had been followed with clinical visits and biological samples collection at baseline and every 3 months. The main study time points selected for the analysis were baseline and 48 weeks. Virological failure was considered if: (i) HIV viral load was persistently detectable after 24 weeks of treatment, (ii) two consecutive detectable HIV viral load determinations after undetectability (≤20 HIV-RNA copies/mL) had been achieved.
Two groups of patients were considered: (i) MVC group: patients who had received MVC 150 mg + atazanavir/ritonavir (ATV/r) 300 mg/100 mg QD; (ii) triple therapy group: those subjects treated with an NRTI combo + 1 non-nucleoside reverse transcriptase inhibitor (NNRTI) or PI. All patients receiving MVC had previously undergone maraviroc clinical test (MCT) to assess the suitability of MVC use (7). In brief, MCT was considered positive if undetectability or an HIV viral load reduction ≥1 log10 copies/mL was achieved after 8 days of MVC monotherapy. The MCT has been reported as a reliable method to assess HIV sensitivity to MVC without the use of phenotypic or genotypic methods (5,6).
Patients gave written informed consent before entering the study that was approved by the Ethics Committee of the Hospital.
Laboratory determinations
Plasma HIV-1 RNA was measured in fresh samples by quantitative polymerase chain reaction (PCR) (Cobas Ampliprep/Cobas Taqman HIV-1 test; Roche Molecular Systems, Basel, Switzerland) according to the manufacturer's instructions. CD4 cell counts were determined in fresh whole blood using the Epics XL-MCL flow cytometer (Beckman-Coulter, Inc., CA), according to the manufacturer's instructions.
Lipid profile including triglycerides, total cholesterol, direct high-density lipoprotein (HDL) cholesterol, and direct low-density lipoprotein (LDL) cholesterol was performed in the routine biochemistry laboratory, using the Cobas 8000 modular analyzer series (Roche Diagnostics, Barcelona, Spain) according to the manufacturer's instructions. Erythrocyte macrocytosis has been reported with the use of first-generation NRTIs, related to mitochondrial toxicity (15,26). Therefore, the erythrocyte mean corpuscular volume (EmCV) was assessed using Advia 2120i (Siemens Healthcare Spain, Madrid, Spain). In addition, high-sensitivity C-reactive protein (hsCRP) and β2-microglobulin levels were determined with an immunoturbidimetric assay on frozen sera, using Cobas 701 (Roche Diagnostics, Mannheim, Germany).
HIV tropism assessment by genotypic method
The third variable loop (V3) of the HIV-1 Env protein was amplified by PCR after the DNA was purified from peripheral blood mononuclear cells using the High Pure PCR Template Preparation Kit (Roche Diagnostics, Barcelona, Spain). The V3 sequences were interpreted using the bioinformatics genotypic tropism predictor geno2pheno (G2P), freely available online (
Statistical analysis
Continuous variables are expressed as median (interquartile range) and categorical variables are expressed as number of cases (percentage). Differences between groups were analyzed using Chi-square test to compare categorical variables and the Mann–Whitney U-test for comparisons of continuous variables. Linear regression test was used to adjust relevant baseline variables for some 48-week outcomes. An intention-to-treat analysis was used to compare the immunovirological efficacy between groups. The Pearson correlation coefficient was used to assess linear correlation between variables. All differences between groups with a two-sided p < 0.05 were considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences software (SPSS 17.0; SPSS, Inc., Chicago, IL). Graphs were drawn using GraphPad Prism (version 6.01 for Windows; GraphPad Software, La Jolla, CA).
Results
Baseline patient characteristics
Ninety-eight patients were finally included in the study: 32 in the MVC group and 66 in the triple therapy group. Baseline characteristics of the patients are summarized in Table 1. All baseline variables were similar in both groups except for gender, CD4 cell count, and Nadir CD4 cells.
Bold means that the result of p comparison value is below 0.05 and therefore statistically significant.
Results are expressed as number of cases and percentage for categorical variables and median and IQR for continuous variables. Chi-square and Mann–Whitney U-tests were used to compare categorical and continuous variables, respectively.
Available for 21 and 59 patients, respectively.
HCV, hepatitis C virus; HDL, high-density lipoprotein; IQR, interquartile range; LDL, low-density lipoprotein; MVC, maraviroc; mCV, mean corpuscular volume; PCR, polymerase chain reaction.
Viral tropism assessment by G2P genotypic method
Thirty patients in the MVC group had available baseline samples to assess genotypic HIV viral tropism. Two subjects had an X4 tropism result (2/30, 6.6%), 3 (3/30, 10%) patients were undetermined due to unsuccessful amplification, and the remaining 25 (83.3%) had an R5 result. Since all patients receiving MVC had a positive MCT, five patients (16.6%) showed discordance between the genotypic tropism and MCT results.
ARV use in the triple therapy group
Thirty-six subjects (36/66, 54.5%) received tenofovir/emtricitabine while the remaining 30 patients (46.5%) received abacavir/lamivudine. The additional drug used in this group was ritonavir-boosted PIs in 24/66 (37.9%) and NNRTIs in 42/66 subjects (62.1%), especially nevirapine (NVP) that was present in 30 patients (30/42, 71.4%). All ARV combinations included in the triple therapy group are detailed on Supplementary Table S1 (Supplementary Data are available online at
Immunovirological efficacy
Thirteen patients (13/98, 13.2%) developed virological failure during the observation period: 10 (10/66, 15.1%) in the triple therapy group and 3 (3/32, 9.3%) in the MVC group (p = 0.32). Eleven patients with virological failure (11/13, 84.6%) showed persistently detectable viral load beyond 24 weeks since therapy onset, whereas the other two occurred close to week 48. Two patients in the triple therapy group suspended therapy due to major side effects (severe rash and central nervous toxicities) and were considered also treatment failures. Finally, two subjects (one in each group) quit therapy by self-decision close to week 48.
Patients included in both groups experienced a comparable decrease of HIV viral load and similar percentages of undetectability at weeks 24 and 48 (Fig. 1a, b), irrespective of baseline HIV viral load (Fig. 1c). The CD4 T-cell increase was also similar (Fig. 1d), even after being adjusted by baseline CD4 T-cell count, HIV viral load, and treatment group (Table 2).

Comparison of immunovirological efficacy between the study groups.
CI, confidence interval.
Toxicities and tolerability
No single patient died or experienced clinical progression during the observation period. Only two patients in the triple therapy group (2/66, 3%) required therapy switch due to major side effects (severe rash and liver toxicity caused by NVP and central nervous toxicity related to efavirenz). No patient required change from ATV/r to darunavir/ritonavir (DRV/r) due to severe jaundice in the MVC group. The lipid modifications at week 48 are summarized in Table 3. There were no significant differences between the study groups on triglycerides, LDL, HDL, and total cholesterol. The proportion of patients with total cholesterol more than 200 mg/dL (42.8 vs. 49.1% for the MVC and triple therapy group, respectively, p = 0.59) and triglycerides more than 200 mg/dL (21.4 vs. 27.2% for the MVC and triple therapy group, respectively, p = 0.5) at the end of the study was similar in both groups.
Available for 55 patients.
Results are expressed as number of cases and percentage for categorical variables and median and IQR for continuous variables. Chi-square and Mann–Whitney U-tests were used for categorical and continuous variables, respectively.
Interestingly, patients belonging to the triple therapy group experienced a significant increase in EmCV at weeks 24 and 48 compared with the MVC group (Fig. 2a). This increase was more remarkable in those subjects receiving abacavir/lamivudine (6.8 [4.8–9.2] vs. 5.1 [2.7–7.1] fL, p = 0.025).
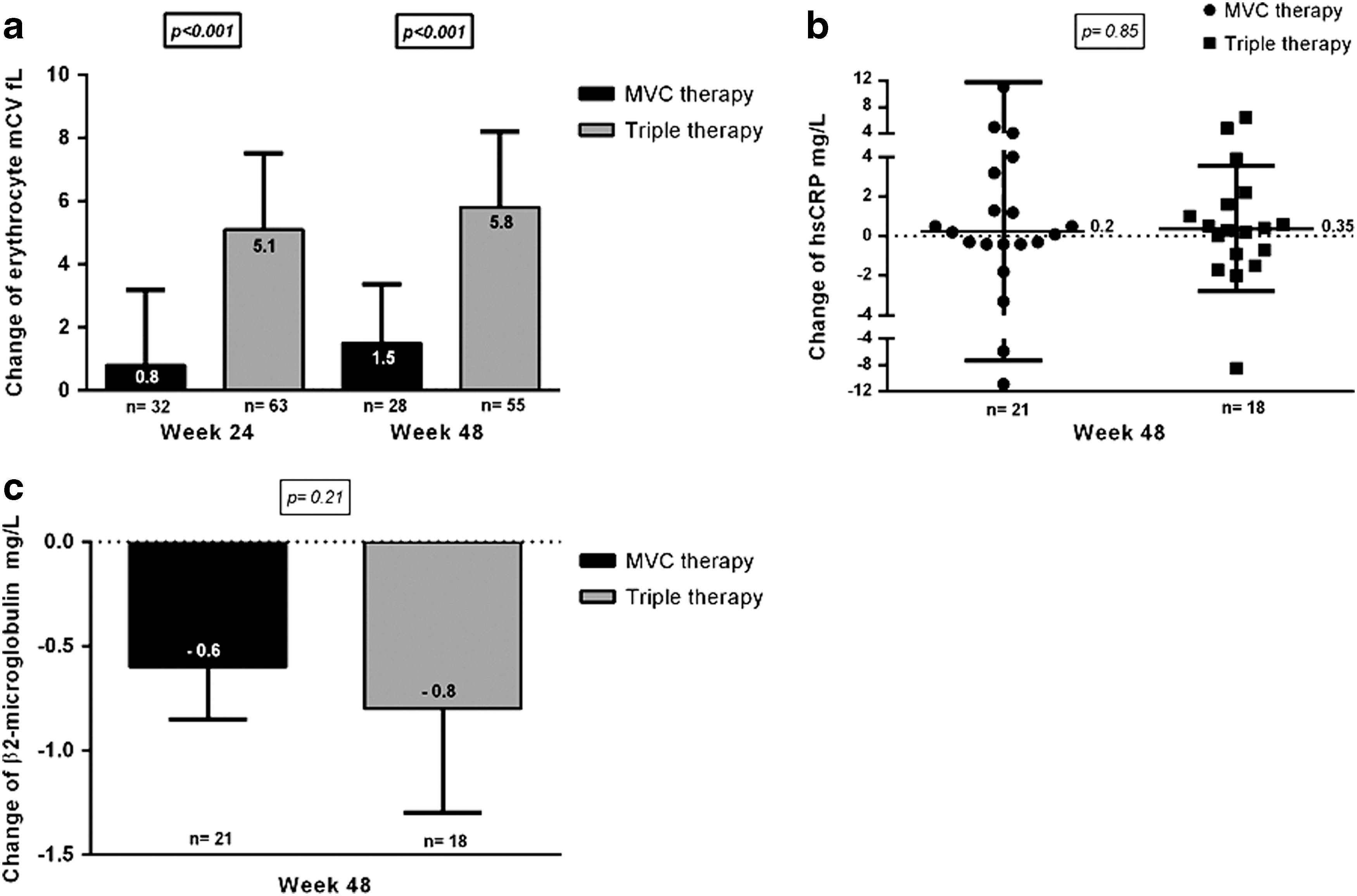
Comparative effect on EmCV and systemic inflammation biomarkers for both treatment groups.
Effect on systemic inflammation biomarkers
The hsCRP and β2-microglobulin levels were determined on available stored frozen serum samples (21 and 18 patients in the MVC and triple therapy groups, respectively). The subjects included in this analysis showed similar baseline characteristics (data not shown). No differences were found on high-sensitivity C-reactive protein (hsCRP) and β2-microglobulin baseline levels between groups (hsCRP: 1.6 [0.7–3.9] vs. 1.3 [0.7–2.1] mg/L, p = 0.70; β2-microglobulin: 2.4 [2.2–3.1] vs. 2.9 [2.3–3.3] mg/L, p = 0.62); for MVC and triple therapy groups, respectively). Both treatment groups experienced a mild and comparable increase of hsCRP (Fig. 2b). The proportion of patients with hsCRP more than 2 mg/L was also similar (Baseline: 38.1 vs. 27.7%, p = 0.49; week 48: 57.1% vs. 50%, p = 0.65; for MVC and triple therapy group, respectively). Finally, a significant and comparable decrease on β2-microglobulin levels at week 48 was observed (Fig. 2c). This β2-microglobulin decrease showed a moderate linear correlation with the 48-week decline of HIV viral load for the MVC group (p = 0.03, r = 0.47) but not for the triple therapy group (p = 0.51, r = 0.16).
Discussion
In this retrospective study, we show a comparable immunovirological efficacy between a once-daily, NRTI-sparing, MVC-containing dual therapy, and standard triple therapy for naive HIV-infected patients in the clinical practice setting. Interestingly, a significant increase on EmCV was selectively observed in the triple therapy group. In addition, both therapy groups had comparable effect on lipid profile and systemic inflammation biomarkers.
Only a few studies have issued the use of CCR5-antagonists as part of an NRTI-sparing regimen in naive HIV-infected subjects. The study by Mills et al. and the MODERN trial reported a reduced virological efficacy of the MVC-containing dual therapy compared with standard triple therapy (16,25). In this study, however, a similar immunovirological efficacy was observed between both study groups. Since we have previously reported a 15–20% discordant results between MCT and both genotypic and phenotypic tropism assays (6,8), the use of a clinical sensitivity test such as MCT instead of tropism methods may have improved the selection of candidate patients for MVC prescription, avoiding a functional ATV/r monotherapy with an impaired efficacy (10). Concordant with our results, an equivalent virological efficacy of low-dose, once-daily MVC combined with LPV/r compared with that of standard triple therapy has been recently reported (18).
The CD4 T-cell change was equivalent in both therapy groups, after adjusting for baseline differences. The intense and equivalent to triple therapy CD4 increase achieved by the MVC + ATV/r dual therapy seems related to the potent CD4 reconstitution effect of CCR5-antagonists (2,31).
Regarding tolerability, no change from ATV/r to DRV/r due to severe hyperbilirubinemia was observed in our study, despite the high rates reported by Mills et al. (16). The routine clinical setting of our study could explain that asymptomatic biochemical hyperbilirubinemia did not result in any PI switch. Although MVC has been reported as a favorable drug for the lipid profile (14), in our study both therapy groups had a similar effect on the different lipid determinations. The high proportion of patients receiving NVP (45.4%) in the triple therapy group, a drug with the most favorable effect on lipids among the available ARV (20), could have influenced these results.
Noteworthy, a significant increase of EmCV was observed in the triple therapy group that seems related to the use of NRTIs, especially in those patients receiving abacavir/lamivudine. Significant macrocytosis associated with the clinical use of first-generation NRTIs was reported more than a decade ago (15,22). The effect of currently available NRTIs on EmCV has been barely explored but seems milder than zidovudine and not reaching the macrocytosis range, according to our results. The cause of this phenomenon is not completely clear, but it could be related to mitochondrial toxicity and subsequent hepatic dysfunction (26), reduced telomerase activity (12), or genotoxicity reported with the use of NRTIs (1,19). The clinical relevance of this potential NRTI toxicity is uncertain; however, the EmCV has been reported as a marker of resting lactate concentrations and consequently of lactic acidosis risk in NRTI-treated patients (32). An NRTI-sparing regimen seems to prevent this EmCV increase according to our results. The potential role of MVC preventing the EmCV increase could not be addressed with our study design.
In addition, MVC has been reported to show a favorable profile on activation and inflammation biomarkers compared with other ARV regimens (4). We have recently reported a decrease of some inflammatory biomarkers 24 weeks after switching to an NRTI-sparing MVC-containing regimen in HIV-infected experienced patients (23). However, in our study, no significant variation in hsCRP levels was found in both treatment groups. This result is most likely explained by the low hsCRP baseline levels in our patients, probably related to the short time from HIV diagnosis, which may have hampered a significant reduction. The decrease of β2-microglobulin levels was concordant with our previous result in experienced patients (23), but no additional benefit was observed in the MVC group compared with triple therapy.
This study has several limitations. First of all, the retrospective design implies known disadvantages compared with prospective studies or clinical trials but gave us the opportunity to explore the clinical practice setting. The significant differences on baseline CD4 counts were addressed by statistical methods as already described. The triple therapy group included different ARV regimens that could have influenced the consistency of this group for comparisons. Only those patients from our cohort with available stored samples could be analyzed for inflammatory biomarker determinations, resulting in low sample sizes and a potential risk of bias, so those results about this particular subanalysis should be considered with caution. Finally, the use of statins in both groups was not controlled since the prescription of these drugs relies on general practitioners in our health system. However, the potential effect of these drugs on lipid profile results was possible for both groups.
In conclusion, treatment with low-dose, once-daily, NRTI-sparing, MVC + ATV/r combination showed immunovirological efficacy comparable with standard triple therapy after 48 weeks with adequate tolerability for naive HIV-infected patients in the clinical practice setting. Moderate increase of EmCV related to NRTIs use is an interesting finding with uncertain clinical relevance that will require further investigation.
Footnotes
Acknowledgments
This study was supported by Fondo de Investigaciones Sanitarias (CP08/00172 to E.R.-M. and CPII13/00037 to Y.M.P.). Redes Temáticas de Investigación en SIDA (ISCIII RETIC RD12/0017/0029 to E.R.-M. and M.L.), Proyecto de Excelencia from the Consejería de Innovación, Ciencia y Empresa (P11-CTS-06313 to E.R.-M.), and Consejería Andaluza de Salud (PI-0278-2010 to E.R.-M.). Ministry of Economy and Competitiveness (Ramón y Cajal grant RYC-2010-07419 to M.R.B.), Consejería de Salud y Bienestar Social de la Junta de Andalucía (Nicolás Monardes' program [C-0010/13] to Y.M.P).
We are grateful to all of the patients who participated in this study and to Maria del Mar Rodriguez, Marien Gutierrez, Magdalena Rodriguez, and Isabel Hidalgo from the Infectious Diseases Service and Hospital de Día.
Author Disclosure Statement
E.R.-M. and M.L. have a grant from Pfizer/ViiV Healthcare (WS2425049). The remaining authors have no competing financial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.