
Abstract
Tumor necrosis factor-alpha (TNFα) and transforming growth factor-beta (TGFβ1) cytokines are highly implicated in liver fibrosis. Polymorphisms in these cytokines affect their expression, secretion, and activity. This study aimed to evaluate the influence of TNFα -308 G/A and TGFβ1 -509 C/T polymorphism on hepatic fibrosis progression in Egyptian patients with hepatitis C virus (HCV) genotype 4. Genotyping of TNFα -308 G/A and TGFβ1 -509 C/T was performed using polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) analysis in 122 subjects (50 healthy controls and 72 HCV patients). Also, serum TNFα and TGFβ1 levels were detected by enzyme-linked immunosorbent assay (ELISA). The genotyping results of early (F0–F1, n = 36) and late (F2–F4, n = 36) HCV fibrosis patients showed that late fibrosis patients had higher TNFα -308 AA genotype and TGFβ1 -509 TT genotype than early fibrosis patients (p = 0.016, 0.028, respectively). Moreover, the TNFα and TGFβ1 serum levels were significantly higher in HCV patients with TNFα A containing genotypes (GA+AA) (p = 0.004) and patients with TGFβ1 T containing genotypes (CT+TT) (p = 0.001), respectively. The combined unfavorable TNFα (GA/AA) and TGFβ1 (CT/TT) genotypes were highly associated with abnormal liver function parameters and were significantly higher in high activity (A2–A3) and late fibrosis (F2–F4) HCV patients (p = 0.023, 0.029). The multivariate analysis results confirmed that the combined TNFα-308 (AA) and TGFβ1 -509 (TT) unfavorable genotypes increased the risk of hepatic fibrosis progression by 6.4-fold than combined favorable genotypes (odds ratio: 6.417, 95% confidence interval [1.490–27.641], p = 0.013). In conclusion, both TNFα -308 G/A and TGFβ1 -509 C/T polymorphisms synergistically influence the hepatic fibrosis progression and can be used as potential biomarkers to predict hepatic disease progression in chronic hepatitis C patients.
Introduction
H
The host immune responses in HCV-infected patients play a pivotal role not only in determining the HCV infection outcome, but also in causing liver injury, fibrosis, and HCC (50,51). While potent immune responses lead to clearance of the viral infection, weak and ineffective immune responses allow continuous viral replication and release of many inflammatory cytokines in the liver, such as interleukins (ILs) (IL-1β, IL-2, IL-6), tumor necrosis factor-alpha (TNFα), interferon-gamma (IFNγ), and hepatocyte Fas (1,48). In addition, uncontrolled HCV infection triggers cell apoptosis and downregulates the protective antioxidant mediators, all of which lead to ultimate severe liver damage. Several studies showed that TNFα and transforming growth factor-beta (TGFβ1) cause chronic liver inflammation, hepatocyte stellate cell (HSC) proliferation, and extracellular matrix deposition, which finally lead to fibrosis (2,17,26,32,40). Continuous expressions of TNFα and TGFβ1 during rat liver damage were reported to induce the synthesis of matrix protein and inhibit activated HSC apoptosis; therefore, the liver fibrosis can be maintained (30).
TNFα is a strong chemoattractant and inflammatory cytokine produced during the acute inflammation and play an important role in cell necrosis and apoptosis. TNFα gene is located within major histocompatibility complex, therefore, any polymorphisms in this locus may contribute to the pathogenesis of many infectious and autoimmune diseases. It was reported that single nucleotide polymorphism (G/A) at -308 TNFα promoter region affects the binding of transcription factor and enhances transcription in monocytic cells and macrophages (21,27,38,47). Previous studies showed that TNFα -308 A allele is associated with high TNFα expression level and susceptibility to asthma, lung fibrosis, and cystic fibrosis progression (39,52).
Different studies showed controversial results regarding the effect of TNFα -308 G/A polymorphism on the HCV severity and outcomes (18,19,41,49). Yee et al., (49) reported that TNFα -308 A allele increased the risk of cirrhosis in HCV infected, whereas Höhler et al., (19) found no association between TNFα -308 polymorphism and HCV infection. Another study showed significantly higher frequency of TNFα -308 A allele in controls than HCV patients (41). In a knockout mouse model, it was proved that TNFα plays an essential role in HCV pathogenesis and hepatocarcinogenesis (25). Kishta et al., (23) showed a positive relation between higher TNFα messenger RNA (mRNA) expression and HCV viral disease progression to HCC. Also, TNFα -308A allele is considered a risk factor for HCC development in hepatitis C virus (HBV) patients (20).
TGFβ1 is a potent inflammatory and regulatory cytokine, which modulates the cell proliferation, differentiation, adhesion, movement, and controls the inflammatory responses. TGFβ1 is very important for the immune system by affecting Foxp3 + regulatory T cell differentiation and preventing phagocyte activation. Also, the TGFβ1 protein is a strong profibrogenic that induces collagen and TIMP-1 expression and downregulates MMP-3 expression. Therefore, polymorphisms of TGFβ1 gene have been shown to affect hepatic fibrosis (33,45).
Different polymorphisms in TGFβ1 gene are probably related to differences in TGFβ1 synthesis and expression. Some TGFβ1 polymorphisms at -509 C/T, +869 C/T, and +915 C/G were documented to affect the TGFβ1 level. Previous reports showed that the TGFβ1 -509 C/T polymorphism in the promoter region is associated with portal vein thrombosis, lymph node metastasis, which finally leads to tumor invasiveness. TGFβ1 -509 T allele is associated with higher TGFβ1 serum level and the concentration is increased with homozygote TT genotype than heterozygote CT genotype (13,37). Moreover, HCC patients had a higher frequency of TT genotype at TGFβ1 -509 polymorphism (29). Therefore, in the current study, we evaluated the influence of TNFα -308 G/A and TGFβ1 -509 C/T polymorphisms on the progression of hepatic fibrosis in Egyptian patients infected with HCV genotype 4.
Materials and Methods
Subjects
The study was approved by the Ethics Committee of the National Research Center, Egypt. A total of 122 subjects, 50 healthy controls and 72 naive treatment HCV-infected patients with a different fibrosis grade, were enrolled in this study. Before enrolling in the study and collecting blood samples, informed consent was obtained from all study subjects. The healthy controls (mean age, 40.3 ± 8.3 years) have no HCV infection (confirmed by antibody and polymerase chain reaction [PCR]), and no history for any liver diseases. The HCV patients (mean age, 43 ± 8.6 years) were clinically investigated at the Ahmed Maher Hospital. The exclusion criteria were HBV or schistosoma infection, decompensated cirrhosis, alcohol- or drug-induced hepatitis, metabolic liver disease, or any significant coexisting medical conditions. The liver function tests, HCV viral load, fibroscan test, and liver biopsy were done for all patients.
Detection of HCV virema and liver biopsy grading
The anti-HCV antibodies in the subjects' sera were detected using Axium HCV Rapid test. The concentration of HCV RNA load in patients' sera was quantified by real-time PCR. Briefly, viral RNA was extracted by using the QIAamp Viral RNA Extraction Kit (Qiagen GmbH, Hilden, Germany) following the manufacturer's protocol. Purified RNAs were quantified by using the Artus HCV RT-PCR Quantification Kit (Qiagen GmbH) on Stratagene Mx3000P Real-Time PCR system according to the manufacturer's protocol. For liver biopsy grading, the liver specimens obtained from all HCV patients were preserved into a 10% buffered formalin solution, according to Hegarty and Williams (16), and were subjected to routine histopathological diagnosis with grading of inflammation and staging of fibrosis. Liver sections were graded according to the degree of periportal and intralobular inflammation, necrosis, and portal inflammation using the METAVIR scoring system (5,42). This scoring system consists of two separate scores, one for necroinflammatory grade (activity scale A0–A3) and another for the stage of fibrosis (fibrosis scale F0–F4). The stages of fibrosis (F) are defined as F0: no fibrosis; F1: portal fibrosis without septa; F2: portal fibrosis with rare septa; F3: numerous septa without cirrhosis; F4: cirrhosis. The grades for activity (A) are A0: no histological necroinflammatory activity; A1: minimal activity; A2; moderate activity; and A3: severe activity.
Genotyping of TNFα -308 G/A and TGFβ1 -509 C/T using PCR-restriction fragment length polymorphism analysis
Whole blood on EDTA was collected from all controls and patients. Then, DNA was extracted by salting out method using the QIAamp Blood Kit according to the manufacturer's instructions (Qiagen GmbH). The PCR technique was used to amplify both the TNFα -308 A/G region and the TGFβ1 -509 C/T region according to Shmarina et al. (39) and Cotton et al. (6). Then the genotyping of each polymorphism was done using the restriction fragment length polymorphism (RFLP) analysis. The amplified -308 TNFα PCR product was digested with NcoI restriction enzyme (Promega, Madison, WI), whereas the amplified -509 TGFβ1 PCR product was digested with Bsu36I restriction enzyme (Promega). The digestion reaction for both TNFα and TGFβ1 PCR product was carried out according to the manufacturer's recommendations. Then, 10 μL of the digested products were run on 4% of agarose gel stained with ethidium bromide. For TNFα -308 polymorphism, the AA genotype showed one fragment of 107 bp, the GG genotype showed two fragments of 87 and 20 bp, whereas the GA genotype showed three fragments of 107, 87, and 20 bp. For TGFβ1 -509 polymorphism, the TT genotype showed one fragment of 153 bp, the CC genotype showed two fragments of 117 and 36 bp, whereas the CT genotype showed three fragments of 153, 117, and 36 bp.
Serum TNFα and TGFβ1 level measurement
Serum samples were collected and stored at −80°C. TNFα and TGFβ1 serum levels were measured in 122 subjects (50 controls and 72 HCV patients) using the TNFα and TGFβ1 ELISA Kit (BioSource Europe S.A.) according to the manufacturer's instructions. The concentrations of TNFα and TGFβ1 in serum were determined using a double antibody sandwich enzyme-linked immunosorbent assay (ELISA). All samples were analyzed and recombinant standards were included in every plate.
Statistical analysis
Data were collected, prepared, and analyzed using (SPSS version 16). Comparisons of the clinical parameters were performed by t-test or chi-squared test. The distribution and frequency of genotypes and alleles in controls and patients were analyzed by chi-squared test. The stepwise logistic regression analysis was used to determine factors associated with hepatic fibrosis progression. The odds ratio (OR) and 95% confidence interval (CI) were calculated to assess the relative risk confidence. Data were considered significant if p values were ≤0.05 and highly significant if p < 0.01.
Results
The clinical data of chronic HCV-infected patients
The 72 HCV fibrosis patients (F0–F4) were divided into early (F0–F1, n = 36) and late (F2–F4, n = 36) fibrosis patients. Comparisons of all clinical parameters in early and late fibrosis patients are summarized in Table 1. Significantly lower levels of platelet count and albumin, and higher levels of liver enzymes, aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and total bilirubin, were found in late fibrosis patients (F2–F4) as compared with early fibrosis patients (F0–F1).
The univariate analysis of all clinical parameters showed that late fibrosis patients have significantly higher ALT, AST, ALP, total bilirubin levels (p = 0.007, 0.01, 0.013, 0.004, respectively) and lower albumin level and platelet counts (p = 0.003, <0.001) than early fibrosis. Also, higher liver activity (A2–A3) was highly detected in late fibrosis patients (p < 0.001). All values were expressed as mean ± SD. p-Value <0.05 is significant, <0.01 is highly significant.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; HCV, hepatitis C virus; SD, standard deviation.
Distribution of different TNFα -308 and TGFβ1 -509 genotypes and alleles in controls and HCV patients
The amplified TNFα -308 PCR products were digested with NcoI restriction enzyme, whereas the amplified -509 TGFβ1 PCR product was digested with Bsu36I restriction enzyme as shown in Figure 1. The distribution of TNFα -308 and TGFβ1 -509 genotypes in controls and HCV patients are shown in Figure 2. The TNFα genotyping results showed statistically significant difference between the controls and HCV-infected patients (p = 0.001). The frequency of A containing genotypes (GA+AA) were significantly different in HCV patients than controls (56.9% vs. 26%, p = 0.002). Actually, both the AA genotype and A allele were increasingly detected in HCV patients compared with controls (p = 0.034, <0.001 respectively). On the other hand, the TGFβ1 genotyping results showed statistically significant difference between the controls (46% CC, 46% CT, and 8% TT) and HCV-infected patients (30.6% CC, 44.4% CT, and 25% TT) (p = 0.024). Generally, the TT genotype and T allele were increasingly detected in HCV patients than controls (p = 0.003, 0.001, respectively). The frequency of each TNFα and TGFβ1 genotype and allele in controls and HCV-infected patients are shown in Table 2.
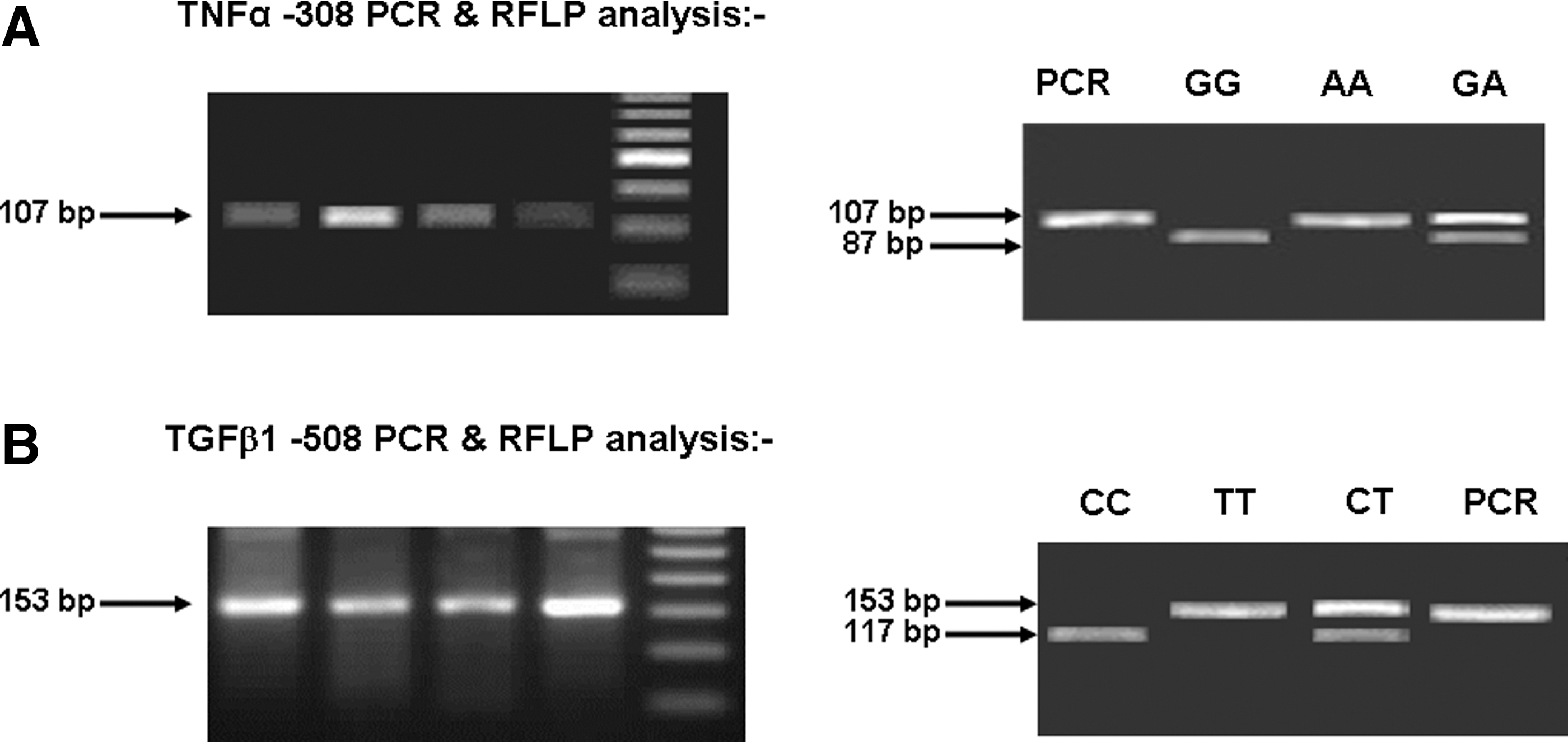
The TNFα -308 and TGFβ1 -509 PCR-RFLP analysis. Genomic DNA was extracted, amplified by PCR, digested with specific restriction enzyme, and run on 4% agarose gel.
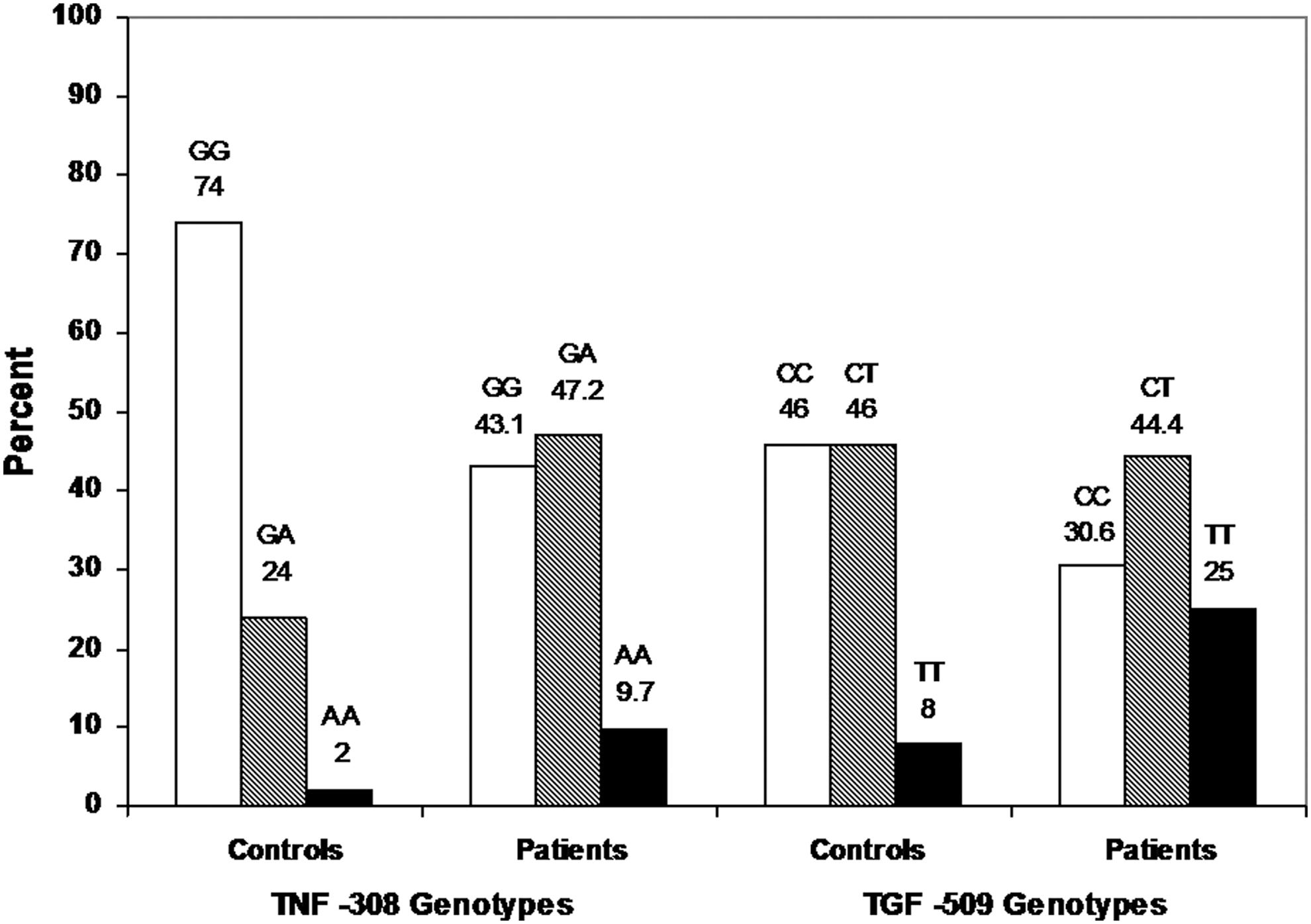
Distributions of TNFα and TGFβ1 genotypes in controls and HCV-infected patients. The PCR-RFLP analysis was used to detect TNFα -308 and TGFβ1 -509 polymorphisms in 122 subjects (50 controls and 72 chronic HCV patients). The distribution of TNFα (GG, GA, AA) and TGFβ1 (CC, CT, TT) genotypes was calculated as percent and presented as bars in controls and HCV patients. HCV, hepatitis C virus; TGFβ1, transforming growth factor-beta; TNFα, tumor necrosis factor-alpha.
One hundred and twenty two subjects (50 controls and 72 chronic HCV patients) were genotyped by PCR-RFLP analysis to detect TNFα -308 and TGFβ1 -509 polymorphisms. The frequency of each genotype and allele was compared in controls and HCV patients. Data were expressed in numbers and percent.
p value <0.05 is significant, <0.01 is highly significant.
CI, confidence interval; OR, odds ratio; PCR-RFLP, polymerase chain reaction–restriction fragment length polymorphism; SNP, single nucleotide polymorphism.
Distribution of different TNFα -308 and TGFβ1 -509 genotypes and alleles in early and late HCV fibrosis patients
The distribution of TNFα -308 genotypes was different in early (55.6% GG, 41.6% GA, and 2.8% AA) than in late (30.5% GG, 52.8% GA, and 16.7% AA) fibrosis patients (p = 0.036). The late fibrosis patients had higher AA genotype and A allele than early fibrosis patients (p = 0.016, 0.013, respectively). On the other hand, the distribution of TGFβ1 -509 genotypes was (41.7% CC, 41.7% CT, and 16.6% TT) in early versus (19.5% CC, 47.2% CT, and 33.3% TT) in late fibrosis patients (p = 0.041). Furthermore, both the TGFβ1 -509 TT genotype and T allele were significantly detected in late fibrosis HCV patients (p = 0.028, 0.019, respectively). The frequency of each TNFα and TGFβ1 allele in early and late fibrosis HCV patients is shown in Figure 3.

The frequency of each TNFα and TGFβ1 allele in early and late fibrosis HCV patients. Frequencies of TNFα G allele (white) and A allele (black) and TGFβ1 C allele (white) and T allele (black) were calculated as percent and presented as bars into early (F0–F1, n = 36) and late (F2–F4, n = 36).
Effect of TNFα and TGFβ1 polymorphisms on serum level
The TNFα and TGFβ1 serum levels were determined in controls and HCV patients. The results showed that TNFα and TGFβ1 serum level were higher in HCV patients than controls (10.7 ± 4.6 vs. 4 ± 1.1 pg/mL, p = 0.05), (13.9 ± 5.1 vs. 4.3 ± 1.1 ng/mL, p = 0.04), respectively. The TNFα and TGFβ1 serum level in HCV patients, early fibrosis patients and late fibrosis patients are shown in Table 3. In HCV patients, statistically the TNFα level is significantly different in patients with late fibrosis than in those with early fibrosis genotype (p = 0.0002), whereas the TGFβ1 level was statistically higher in HCV late fibrosis patients with (CT + TT) genotypes than in early fibrosis patients (p = 0.0001). Patients with unfavorable TNFα GA or AA genotypes have a statistically significant difference in TNFα level than those with favorable GG genotype in HCV patients (p = 0.045), in early fibrosis patients (p = 0.004), and in late fibrosis patients (p = 0.0001). Moreover, the mean TGFβ1 level in HCV patients, early fibrosis patients, and late fibrosis patients was significantly different in patients with unfavorable CT+TT than those with favorable CC genotype (p = 0.05, 0.045, 0.0006, respectively).
The TNFα and TGFβ1 serum level were measured in early and late fibrosis patients. Data were expressed as mean ± SD.
Significant difference from GG; b p < 0.05; c p < 0.01; dsignificant difference from CC.
TGFβ1, transforming growth factor-beta; TNFα, tumor necrosis factor-alpha.
The synergistic effect of TNFα -308 and TGFβ1 -509 polymorphisms on hepatic fibrosis progression
The genotyping results showed that 15 patients have both TNFα and TGFβ1 favorable genotypes (GG+CC), 32 patients have both TNFα and TGFβ1 unfavorable genotypes (GA or AA + CT or TT), and 25 patients with mixed genotypes (GG + CT or TT) or (GA or AA+CC). The influence of separate and combined TNFα -308 and TGFβ1 -509 genotypes on hepatic fibrosis progression is shown in Table 4. Patients with elevated levels of ALT, AST, ALP, and bilirubin, and lower levels of platelets and albumin have significantly combined unfavorable TNFα -308 (GA or AA) and TGFβ1 -509 (CT or TT) genotypes more than combined favorable TNFα -308 (GG) and TGFβ1 -509 (CC) genotypes as indicated in Table 5. The statistical results showed that both late fibrosis (F2–F4) and high liver activity (A2–A3) patients have higher frequency of combined unfavorable genotypes than combined favorable genotypes (55.6% vs. 11.1%, p = 0.009; 59.5% vs. 11.9%, p = 0.001, respectively).
The effect of different TNFα -308 and TGFβ -509 genotypes, alleles on hepatic fibrosis progression was statistically analyzed in early and late fibrosis patients. The unfavorable genotypes have effect on hepatic fibrosis progression (p = 0.017). p Value <0.05 is significant, <0.01 is highly significant. Favorable genotypes: TNFα (GG)+TGFβ1 (CC); mixed genotypes: TNFα (GG)+TGFβ1 (CT or TT) or TNFα (GA or AA)+TGFβ1 (CC); unfavorable genotypes: TNFα (GA or AA)+TGFβ1 (CT or TT).
The combined bad genotypes associated with high (ALT, AST, Alk.Ph, Bilirubin) levels and lower albumin and platelet count. Moreover, the unfavorable genotypes highly affected the liver activity and fibrosis (p = 0.001, 0.009). All clinical values were expressed as mean ± SD, whereas liver activity and fibrosis were expressed as number and percent. p-Value <0.05 is significant, <0.01 is highly significant. Favorable genotypes: TNFα (GG)+TGFβ1 (CC); mixed genotypes: TNFα (GG)+TGFβ1 (CT or TT) or TNFα (GA or AA)+TGFβ1 (CC); unfavorable genotypes: TNFα (GA or AA)+TGFβ1 (CT or TT).
T.Bilirubin, total bilirubin.
Multinomial analysis of predictive factors for hepatic fibrosis progression in HCV patients
The stepwise logistic regression analysis was used to determine the significance of different host factors in the progression of hepatic fibrosis in chronic HCV patients. The results showed that the levels of ALT, AST, ALP, bilirubin, albumin, platelets count, TNFα -308, and TGFβ1 -509 combined genotypes, and alleles independently and significantly influenced the outcome of hepatic progression as shown in Table 6. The multivariate analysis results showed that HCV patients with unfavorable TNF (GA+AA) genotypes increased the risk of liver fibrosis progression (2.8-fold) than those with favorable genotypes (GG) (OR: 2.841, 95% CI 1.080–7.472, p = 0.034), whereas HCV patients with unfavorable TGF (CT+TT) genotypes had higher risk of liver fibrosis progression (2.9-fold) than those with favorable genotypes (CC) (OR: 2.959, 95% CI 1.027–8.528, p = 0.045). However, unfavorable combined genotypes in HCV patients increased the risk of liver fibrosis by 6.4-fold more than those with favorable combined genotypes (OR: 6.417, 95% CI 1.490–27.641, p = 0.013). The results showed the synergistic effect of unfavorable combined genotypes as they increased the risk of liver progression (6.4 times) than unfavorable TNF (2.8 times) or TGF (2.9 times) genotype alone. Also, combined unfavorable (A+T) alleles are risk for liver fibrosis (OR 1.976, 95% CI 1.161–2.717, p = 0.008).
The influence of ALT, AST, ALP, bilirubin, albumin and platelet count, TNFα -308 and TGFβ -509 favorable genotypes, and alleles on hepatic progression were analyzed. The OR and 95% CI were calculated to assess the relative risk confidence. p-Value <0.05 is significant, <0.01 is highly significant.
Discussion
Chronic hepatitis C is the most outstanding cause for high liver-related diseases in Egypt. HCV infection causes liver inflammation, which leads to HSCs activation and extracellular matrix deposition. Recently, it was reported that activation of HSCs is regulated by TNFα and TGFβ1 cytokines (9,17,26). It was reported that host genetic variations in TNFα and TGFβ1 influence the strength of immune response and the disease outcomes in HCV-infected patients (15). Some reports studied the role of TNFα -308 and TGFβ1 -509 polymorphisms in the susceptibility of HCV infection and treatment response (34,37). Nevertheless, in this study we evaluated the influence of TNFα -308G/A and TGFβ1 -509C/T polymorphisms on hepatic fibrosis progression in 122 Egyptian subjects (72 HCV genotype 4 patients with different fibrosis grades [F0–F4] and 50 healthy controls).
The TNFα -308 genotyping results revealed that genotypes (GA or AA) were higher in chronic HCV patients than controls (p = 0.002). In addition, TGFβ1 -509 genotyping results showed that genotype TT was significantly detected in chronic HCV patients than controls (p = 0.024). Similar findings were reported by Pasha et al., (34) and Dogra et al., (8) who showed that TNFα -308 (GA+AA) genotypes and A allele were significantly higher in HCV patients than healthy controls and were associated with the susceptibility to HCV infection. However, other studies failed to find any differences in TNFα -308 genotypes between chronic HCV patients and healthy subjects (19,35,44). Our TGFβ1 -509 results confirmed earlier studies which reported that the TGFβ1 -509 T allele (high TGFβ1 producer) was significantly higher in HCV-infected patients than in healthy controls (22,34).
TNFα and TGFβ1 cytokines are highly implicated in chronic liver inflammation, fibrosis, and cirrhosis development (20,29,48,50). The genotyping results in HCV patients with different fibrosis grade showed that HCV patients harboring both TNFα -308 (GA or AA) and TGFβ1 -509 (CT or TT) genotypes have higher degree of liver fibrosis (69.4%, 80.6%, respectively). Moreover, the TNFα and TGFβ1 serum level were significantly higher in HCV patients with TNFα A containing genotypes (GA+AA) (p = 0.004) and patients with TGFβ1 T containing genotypes (CT+TT) (p = 0.001).
Our observations suggested that polymorphisms at both TNFα -308 and TGFβ1 -509 involved in hepatic fibrosis progression by increasing the circulating TNFα and TGFβ1 levels in the body. These results are in agreement with previous studies, which reported higher frequency of TNFα -308 (AG + AA) and TGFβ1 -506 (CT+TT) genotypes in cirrhotic and HCC patients (12,37). Also, Kroeger et al. (27) found that the A allele at TNFα -308 alters the transcription factor binding site, which leads to high TNF gene expression. Nonetheless, Grainger et al. (13) showed that the T allele at TGFβ1 -509 is associated with lower T cell proliferation and higher TGFβ1 concentration. The severity of liver cirrhosis is associated with high TNFα and TGFβ levels and this can be explained by the fact that the biological effects of any cytokine depend mainly on its concentration in the site of action (43,51). Moreover, TNFα -308 A allele and TGFβ1 -509 T allele dose effect was reported as higher concentration of circulating TNFα and TGFβ1 levels were found in individuals with homozygote genotypes (AA/TT) than those with heterozygote genotypes (GA/CT) (12). On the contrary to our results, Höhler et al. (19) and Talaat et al. (41) did not find any association between TNFα -308 genotypes and HCV infection. However, others found that the C, not T, allele of TGFβ1 -509 could play important roles in liver cirrhosis development and TT genotype may protect from HCC (36,45).
Interestingly, the results of this study showed that combined TNFα and TGFβ1 unfavorable genotypes are associated with abnormal liver function parameters. Also, the frequency of combined unfavorable genotypes are significantly higher in HCV patients with high (A2–A3) than those with low (A0–A1) activity (78.1%, vs. 21.9, p = 0.023) and in patients with late (F2–F4) than those with early (F0–F1) fibrosis (62.5% vs. 37.5%, p = 0.029). On the other hand, the multivariate analysis results confirmed that the combined TNFα and TGFβ1 unfavorable genotypes increased the risk of hepatic fibrosis progression by 6.4-fold than combined favorable genotypes (OR: 6.417, 95% CI from 1.490 to 27.641, p = 0.013). The results confirmed the synergistic effect of unfavorable combined TNFα -308 and TGFβ1 -509 genotypes as they increased the risk of liver progression (6.4-fold) than unfavorable TNF (2.8-fold) or TGF (2.9-fold) genotype alone. Similar to these results, it was reported that TNFα -308 A allele is a risk factor for both HCC development (18,20) and treatment failure in HCV genotype 1b patients (7,14).
Several polymorphisms in IFN-induced genes and cytokines have been reported to alter the gene expressions and affect the liver disease progression (3,4,10,24). However, the current findings reveal that both TNFα -308 G/A and TGFβ1 -509 C/T polymorphisms synergistically influence the hepatic fibrosis progression and can be used as potential biomarkers to predict hepatic disease progression in chronic hepatitis C patients.
Footnotes
Acknowledgments
This work was partially funded through the Science and Technology Development Fund (STDF), Egypt, Grant No. 3365 to M.K.E.A. All authors thank Dr. Amr Moustafa for referring the cases.
Author Disclosure Statement
No competing financial interests exist.