
Abstract
Tumor necrosis factor (TNF)-α is a key cytokine in the pathogenesis of dengue virus infection, and its accurate detection in several types of human samples is critical. The enzyme-linked immunosorbent assay (ELISA) is the gold standard for the detection of TNF-α, but multiplexed bead-based assays such as cytometric bead array (CBA) are now frequently used. Here, using ELISA and two CBAs commercially available, we measured TNF-α concentrations in plasma and serum from children with acute dengue virus infection and healthy controls. To evaluate the detection efficiency and factors affecting it, spiked recovery and immune complex dissociation assays were also performed. The levels of TNF-α evaluated by ELISA in paired serum and plasma samples from children with dengue positively correlated (rho = 0.99, p < 0.0001). Children with dengue had higher levels of plasma TNF-α than those of healthy children (p = 0.004). The ELISA detected TNF-α in a higher number of plasma samples than the CBA (p < 0.0001), and both methods only correlated when TNF-α was evaluated in buffer-based solutions but not in plasma, indicating the presence of a factor interfering with the detection of TNF-α in plasma. The recovery of several types of human recombinant TNF-α was dramatically decreased in plasma but not in tissue culture media (p ≤ 0.01), and this effect was similar in the plasma obtained from the children with dengue or the healthy controls. The dissociation of immune complexes did not improve TNF-α recovery. Dilution of the plasma samples increased the recovery of TNF-α, but at high concentrations of the cytokine. In short, plasma affects the efficiency of TNF-α detection, and this effect should be considered in the measurement of this cytokine.
Introduction
T
Several factors affect the efficiency of the detection of CTs in biological samples, and in some cases, the results obtained may not reflect the true concentrations (38). Some biological factors that affect detection include the CT kinetics or the binding of proteins or soluble decoy receptors that could be increased during the acute phase of infections (7). Technical factors include the type of the sample and its handling, ability of the operator, and type of assay used (53). For the measurement of TNF-α, the enzyme-linked immunosorbent assay (ELISA) is the most widely used method and is considered the gold standard (19). However, bead-based assays, such as the cytometric bead array (CBA), allow for the analysis of a larger number of analytes in a smaller sample volume with a reported higher sensitivity, and thus the use of CBA has increased in recent years (37).
Dengue is a disease in which TNF-α is critical. This disease is caused by infection with the dengue virus (DENV) and is an important viral vector-borne disease worldwide (6). During the acute phase of infection, high serum and plasma levels of CTs such as IL-2, IL-6, IL-8, IL-10, interferon-γ, and TNF-α have been reported (21,34). Moreover, these CTs have been implicated in the development of vascular leakage and bleeding, which are the hallmarks of this disease (10,47), and in some studies, the plasma or serum levels of these CTs have been associated with clinical severity (29,33,42). However, the case of TNF-α is peculiar. Although TNF-α levels have been reported to increase in patients with dengue in comparison with those of healthy controls (12,35,49), the plasma and serum concentrations of TNF-α are typically very low (3,39,43). In other cases, no differences were found in the plasma levels of TNF-α between the acute and convalescent phases of the disease (46). Likewise, the relationship between the levels of TNF-α and clinical severity has been inconsistently reported, and positive (2), negative, or not associations have been shown (31). These discrepancies are less dramatic when TNF-α is evaluated in cell culture supernatant or other buffers (11,23). As the analysis of TNF-α in dengue and other infectious and autoimmune diseases is an essential requirement, studies that evaluate the factors affecting its detection are necessary.
Here, the efficiency of TNF-α measurement in plasma and serum obtained from children with confirmed DENV infection and healthy controls was evaluated using commercially available ELISA and bead-based assays. The recovery of human recombinant TNF-α from plasma and tissue culture media was also assessed. Together, the results demonstrate a low efficiency in the detection of TNF-α in plasma obtained from children with dengue or healthy controls, particularly when it is evaluated using CBA. This effect should be taken into account when using this type of sample.
Materials and Methods
Ethics statement
This study was approved by the Committee on Ethics of the Hospital Universitario de Neiva. Informed consent and assent (for children over 6 years of age) were obtained from all the subjects included. All experiments followed the principles expressed in the Declaration of Helsinki.
Patients and samples
This study was conducted from April 2009 to August 2015 in the Laboratorio de Infección & Inmunidad of the Facultad de Salud, Universidad Surcolombiana. Children between 1 and 14 years old with confirmed acute DENV infection (n = 94) on the fourth to eighth day of fever onset and healthy children who served as controls (n = 20) were included in this study. For the inclusion of the control group, a medical examination was performed for the pediatric department of the Hospital Universitario de Neiva, and any ongoing disease was ruled out. For the diagnosis, classification, and clinical monitoring of the dengue patients, the revised guidelines of the World Health Organization 2009 (1) were followed. The diagnosis of infection was confirmed by plasma evidence of the viral nonstructural protein (NS)-1 (Dengue Early ELISA, Ref: E-DEN02P) and/or dengue-specific immunoglobulin (Ig) M (Dengue IgM Capture ELISA, Ref: E-DEN01 M) (both from Panbio, Alere, Waltham, MA), which were detected using ELISA and following all manufacturer's instructions. The type of infection (primary or secondary) was determined using the dengue-specific IgM/IgG ratio (the latter evaluated with the Panbio Dengue IgG Capture kit [Ref: E-DEN02G]), where a ratio ≤2 represented a secondary infection (24).
Two to four milliliters of venous blood was collected in tubes containing ethylenediaminetetraacetic acid (EDTA; BD Vacutainer, San Jose, CA; Cat: 367861). To obtain paired serum samples, venous blood was taken in tubes without anticoagulants from some children (n = 30) (BD Vacutainer; Cat: 367812). Within 2 h of collection, the tubes were centrifuged at 300 g for 10 min, and the plasma and serum were immediately collected and stored at −70°C until the time of analysis. All of the plasma and serum samples were obtained in the morning hours. The median (range) storage time of samples from the children with dengue and the healthy controls were 29 (6–83) and 25 (14–79) months, respectively (p = 0.1, Mann–Whitney test). Due to limited sample volume, some of the children were not included in all the analysis.
Additionally, adult patients with lung diseases (such as suspected pulmonary tuberculosis, bacterial pneumonia, or tumors, n = 50) who underwent a diagnostic bronchoscopy with bronchoalveolar lavage (BAL) were also included. All of these participants were sero-negative for Human Immunodeficiency Virus infection. To obtain the BAL, 80 mL of sterile normal saline solution (Baxter, Deerfield, IL; Cat: ARB1322) was added through a flexible bronchoscope (Fujinon, Saitama, Japan; Ref: EB-470S), retired during the procedure and at least 5 mL was collected, centrifuged at 300 g for 10 min, filtered with a 0.22 μm filter (Merck Millipore, Billerica, MA; Cat: SLFG025LS) before storage at −70°C. The bronchoscopy procedure was completed by a trained pulmonologist.
Evaluation of TNF-α concentrations by ELISA and CBA
At the time of analysis, each plasma, serum or BAL sample was thawed at room temperature and centrifuged at 2,600 g for 10 min. The concentration of TNF-α was evaluated by ELISA using a commercial kit (DuoSet Human TNF-α, R&D, Minneapolis, MN; Cat: DY-210) following all of the manufacturer's recommendations. The reported detection limit was 3 pg/mL. The mean optical density (OD) of the negative controls (diluent medium alone) at 450 nm was 0.060. TNF-α concentrations were calculated by interpolation of OD of the samples to a standard curve using 4-parameter logistic regression with GraphPad Prism® 7.0 (GraphPad Software, La Jolla, CA). In the case of CBA, the Human Th1/Th2 Cytokine Kit II (BD; Cat: 551809) and the Human TNF Enhanced Sensitivity Flex Set (BD; Cat: 561516) were used following all of the manufacturer's recommendations. The assay's limit of detection for TNF-α was 2.8 pg/mL for the Th1/Th2 Kit II and 0.067 pg/mL for the Enhanced Sensitivity Flex Set. The FACS Diva software (v. 6.1.3) and FCAP (v. 3.0.14) software, both from BD, were used for bead acquisition and calculation of CT levels, respectively. The ELISA and CBA analyses of plasma and serum were simultaneously completed using the same samples. The samples were analyzed in duplicate, and a variability of less than 10% was noted. Only ELISA and CBA experiments with standard curves with R 2 > 0.98 and significant p values were included.
Human recombinant TNF-α spike recovery assays
Known amounts of human recombinant TNF-α (hrTNF-α; R&D; Cat: 840121 and BD; Cat: 51-9003509) were added to plasma (from children with dengue and healthy controls) or to sterile tissue culture media (RPMI 1640; Gibco, Carlsbad, CA; Cat: 11875-085). After incubation for 30 min at 37°C, the samples were analyzed by ELISA and/or CBA as described above. Additionally, in some experiments, two-fold serial dilutions of plasma samples after the addition of the hrTNF-α were performed using 1% Bovine Serum Albumin (BSA, Sigma-Aldrich, St. Louis, MO; Cat: A7906) in 1 × DPBS (Gibco; Cat: 21600-069), pH 7.3, filtered, as diluent medium. The concentrations of hrTNF-α in the diluted samples were interpolated from the ELISA standard curve (as described in the Evaluation of TNF-α concentrations by ELISA and CBA section) and then multiplied by the dilution factor. The percentage of hrTNF-α recovery was obtained as previously reported (41):% Recovery = (spiked sample result–unspiked sample result)/known spike added concentration × 100.
Dissociation of immune complexes
A previously described protocol for the dissociation of immune complexes in plasma was applied (27,30). Briefly, 100 μL of plasma with and without hrTNF-α were mixed with 50 μL of 0.5 N hydrochloric acid (Merck, Darmstadt, Germany; Cat: K21327817 488; pH 2.5–3), incubated for 60 min at 37°C, and neutralized with 50 μL of 0.5 N sodium hydroxide (Merck; Cat: B676398 522; pH 6.8–7.2). The concentrations of hrTNF-α were measured by ELISA in the treated and untreated pared samples. To prove the efficiency of the protocol used here, we evaluated the level of dissociation of DENV-specific IgM - DENV complexes in plasma from three children with secondary acute DENV infection. After the pH treatment, four 10-fold serial dilutions of the samples were performed, and the DENV-specific IgM was semi-quantified in duplicate using a commercial ELISA (Dengue IgM Capture ELISA, Panbio, Alere, Waltham, MA; Ref: E-DEN01 M). The dissociation of the immune complexes was demonstrated by increased absorbance at OD450 nm after treatment.
Statistical analysis
GraphPad Prism® 7.0 software for Mac was used for the statistical analysis. The data are presented as medians and ranges. For statistical purposes, a value equal to half of the reported limit of detection of the assays was assigned to samples with TNF-α levels below the cutoff. The Mann–Whitney and Wilcoxon tests were used to analyze two independent or dependent groups, respectively. To analyze more than two independent or dependent groups, the Kruskal–Wallis and Friedman tests were used, respectively. If the Kruskal–Wallis or Friedman p value was <0.05, Dunn's post hoc test was used. The degree of correlation between variables was determined using the Pearson (r) test. Fisher's test was used for frequency analysis. A p value <0.05 was considered significant.
Results
Patients included
This study included 94 children with confirmed acute DENV infection (20 primary and 74 secondary infections, as determined by the dengue-specific IgM/IgG ratio) and 20 healthy children as controls. The median (range) day of illness when the children with dengue were included was 5 (4 –8). Table 1 shows the age and the laboratory characteristics of the children included. As expected, the children with dengue had lower leukocyte and platelet counts than those of the healthy controls (p = 0.003 and p = 0.001, respectively, Mann–Whitney test, Table 1), but there were no differences in the levels of hemoglobin and hematocrit (p = 0.3 and p = 0.08, respectively, Mann–Whitney test, Table 1). In the adult patients with lung diseases (age, median [range]: 45 years [18–88]), 7 patients (14%) had active pulmonary tuberculosis (confirmed by mycobacterial culture and/or real time polymerase chain reaction), 33 patients (66%) had bacterial pneumonia, 5 patients (10%) had tumors, and 5 patients (10%) had pulmonary tuberculosis sequelae (data not shown).
Not all of the children with dengue or all of the healthy children were included in each reported experiment.
The level of TNF-α measured in plasma is comparable to that in serum
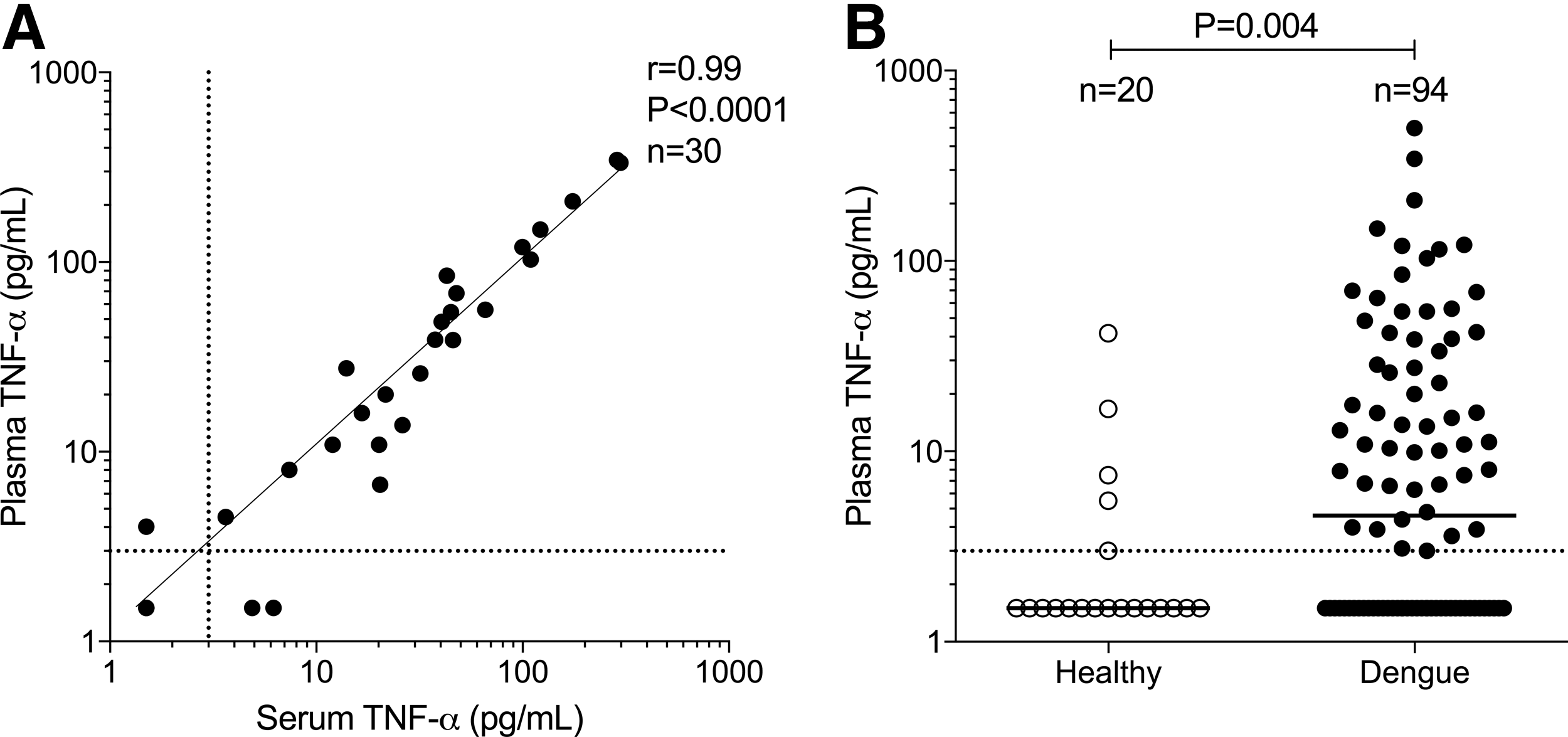
Although serum is frequently used for the measurement of CTs, its use does not allow for the isolation of peripheral blood mononuclear cells or other cellular analyses for which anticoagulated blood is required. Therefore, plasma in those cases is preferred over serum, and the comparison of its performance with that of serum is necessary. To determine whether plasma is comparable to serum for the detection of TNF-α, the concentration of this CT was determined by ELISA in both paired types of samples from the children with dengue. As is shown in Figure 1A, the levels of TNF-α evaluated in serum and plasma strongly correlated (r = 0.99, p < 0.0001, Pearson test), indicating that the detection of the CT in both types of samples is comparable. The evaluation of TNF-α in plasma also allowed for the determination of biological differences between the children with dengue and the healthy controls. Similar to the results of previous reports (2,39), low but detectable levels were obtained in the DENV-infected children when compared with those of the healthy controls (median pg/mL [range] 4.6 [1.5–499] and 1.5 [1.5–41.8], respectively; p = 0.004, Mann–Whitney test, Fig. 1B). Similar results were also obtained when the serum isolated from these two groups was evaluated (p = 0.004, Mann–Whitney test, data not shown).
Comparison of plasma and serum for the detection of TNF-α.
Efficiency of CBA and ELISA for the detection of TNF-α in plasma and buffer solutions
Plasma was comparable to serum for the detection of TNF-α by ELISA. Because CBA offers a large number of advantages over ELISA, we next determined whether CBA is comparable to ELISA for the measurement of TNF-α in plasma. For this purpose, the levels of the TNF-α were determined in the plasma from the children with dengue by ELISA and two available CBA formats (Th1/Th2 cytokine kit II and TNF-α Enhanced Sensitivity Flex Set). As shown in Figure 2A, the levels of TNF-α evaluated by the CBA Th1/Th2 kit II were below the assay's limit of detection in 93% of the samples, whereas 46% of the samples were undetectable by ELISA (p < 0.0001, Fisher's test), indicating a higher detection rate of TNF-α by ELISA. When the second CBA format was used in some samples, detectable but very low amounts (in femtogram range) of TNF-α were noted in 100% of the samples analyzed (Fig. 2B). However, there was no correlation between the levels of TNF-α in plasma detected by ELISA and the CBA Th1/Th2 kit II (r = −0.03, p = 0.8, Pearson test, Fig. 2A) or between ELISA and the CBA Enhanced Sensitivity Flex Set (r = −0.2, p = 0.5, Pearson test, Fig. 2B), indicating a low comparability between both assays for the measurement of this CT in plasma.
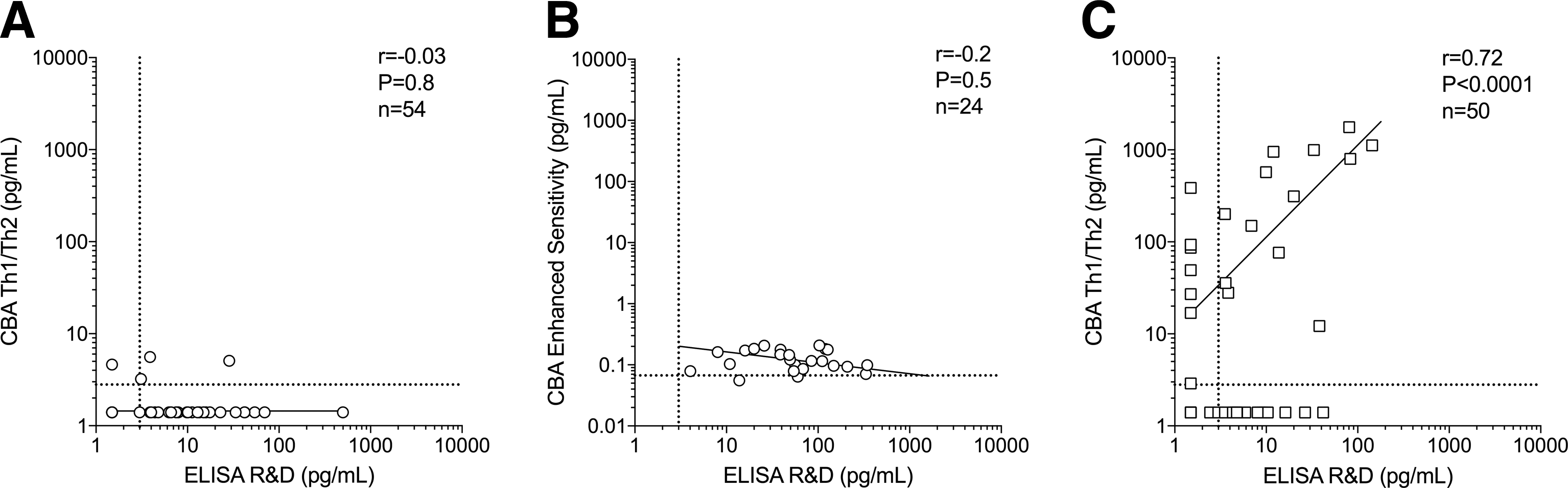
Comparison of ELISA and CBA by the detection of TNF-α in plasma and buffer solutions. Correlation between the levels of TNF-α in the plasma from children with dengue determined by ELISA from R&D and CBA Th1/Th2 kit II
CBA was less efficient than ELISA for the detection of TNF-α in plasma, and we determined whether this efficiency depends on the assay or the type of sample used. TNF-α levels in the BAL from the adult patients with lung diseases were measured by ELISA and CBA Th1/Th2 kit II. As shown in Figure 2C, high levels of the CT were obtained by both methods in the BAL samples, with a positive correlation (r = 0.72, p < 0.0001, Pearson test, Fig. 2C). Together, these results indicate that CBA has a low efficiency for the detection of TNF-α in plasma but not in BAL (a buffer-based solution). As ELISA was more efficient for detection of TNF-α in plasma, this assay was used for the subsequent set of experiments.
Plasma affects the recovery of hrTNF-α
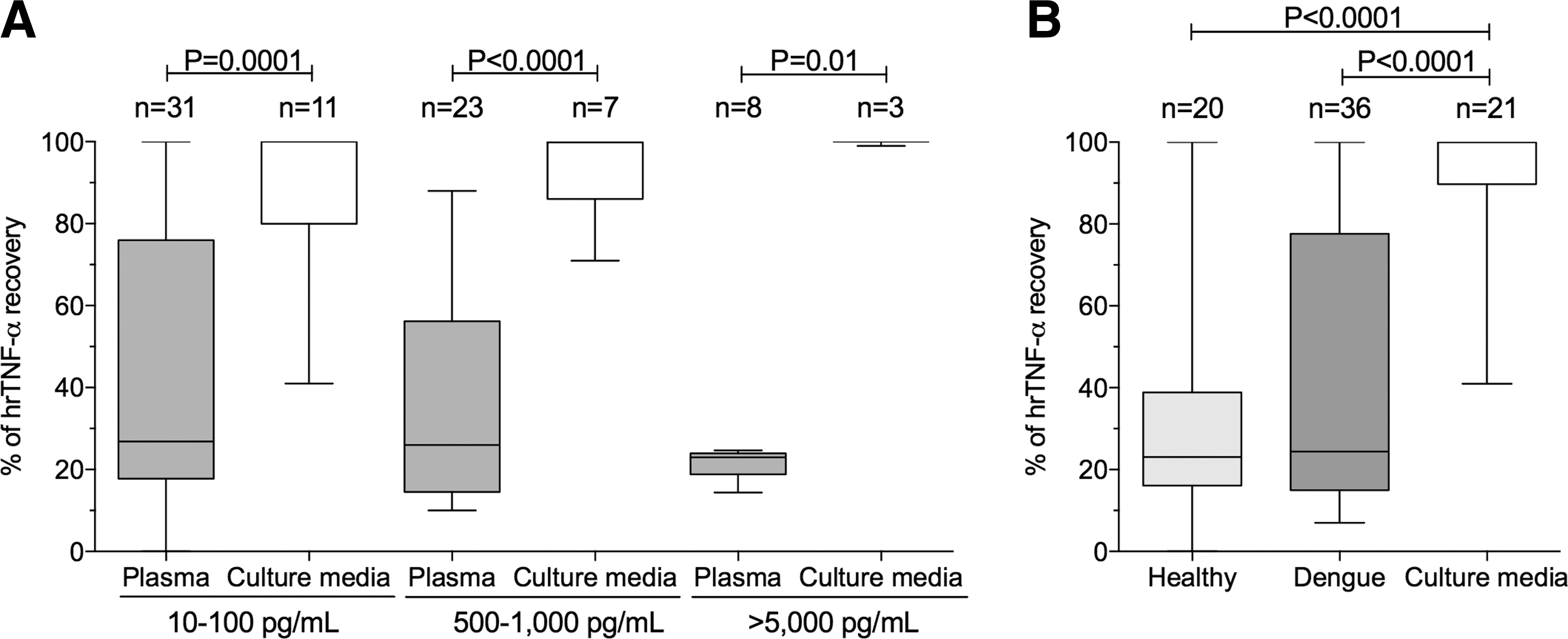
To evaluate the effect of plasma in the detection of TNF-α, known concentrations of the hrTNF-α were added to plasma samples or tissue culture media and then measured by ELISA, and the percentage of TNF-α recovery was determined. As shown in Figure 3A, in comparison with tissue culture media, a significantly lower percentage of hrTNF-α recovery was obtained in plasma (mixed children with dengue and healthy controls) when low (10–100 pg/mL), intermediate (500–1,000 pg/mL), and high (>5,000 pg/mL) concentrations of the recombinant CT were added (p ≤ 0.01, Mann–Whitney test; Fig. 3A), indicating that plasma largely affects the measurement of TNF-α. Similar results were obtained with CBA, using the hrTNF-α from both R&D and BD (n = 10, p ≤ 0.01, plasma versus tissue culture media, Mann–Whitney test, data not shown). However, it is possible that the effect is not due to the plasma itself but is due to the condition of the individual from whom the sample was taken. For example, in acute DENV infection, increased levels of the soluble TNF receptors (sTNFRs) are found (2), and these proteins could act as decoys for the soluble TNF-α and interfere with its detection (14). Hence, the percentage of hrTNF-α recovery (at the previously described concentrations) in the plasma from the children with dengue and the healthy controls was compared. As shown in Figure 3B, a higher percentage of hrTNF-α recovery was obtained in tissue culture media when compared with the plasma from the children with dengue and the healthy controls (p < 0.0001, Dunn's post-hoc test; Fig. 3B), but no difference was found between both pediatric groups (p = 0.9, Dunn's post-hoc test, Fig. 3B). In summary, plasma affected the detection of hrTNF-α, but this effect was independent of the condition of the individual from whom the sample was obtained.
Efficiency of the detection of TNF-α in plasma.
The low detection of TNF-α is not due to the presence of circulating immune complexes
In addition to the presence of circulating decoy receptors, the low detection of TNF-α in plasma could be explained by the binding of antibodies (such as low affinity natural antibodies) to TNF-α. To establish a mechanism explaining the low detection of TNF-α in plasma, we hypothesized that the presence of circulating immune complexes [e.g., increased auto-antibodies have been reported during DENV infection (44,50)] could interfere with the measurement of the CT (51). Thus, the recovery of TNF-α in plasma after the dissociation of immune complexes was evaluated. As shown in Figure 4A, the pH-based protocol for immune complexes dissociation was efficient, as higher DENV-specific IgM in the plasma from the children with secondary DENV infection was obtained when the samples were pH-treated in comparison with the nontreated samples (p = 0.0005, Wilcoxon test). However, the pH-based treatment did not improve the hrTNF-α recovery at both concentrations of 100 and 1,000 pg/mL of the added recombinant CT (p ≥ 0.3, Wilcoxon test, Fig. 4B). Therefore, the presence of circulating immune complexes does not explain the low detection of TNF-α in the plasma from the children with dengue.

Effect of circulating immune complexes in the detection of TNF-α in plasma.
Plasma dilution improves the detection of hrTNF-α, but only at high concentrations of the CT
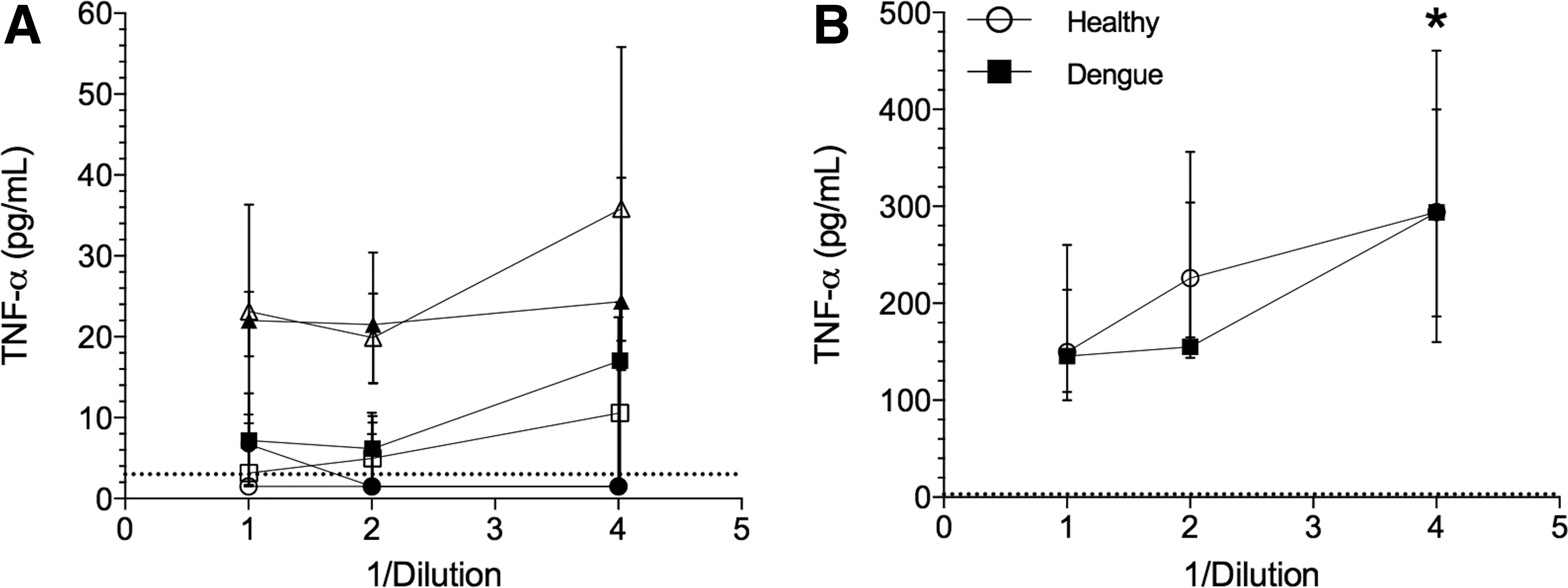
Together, the previous results showed that plasma affects the efficiency of TNF-α detection independent of the assay used or the condition of the individual, even after the addition of high concentrations of the human recombinant CT. The dilution of the sample, and thus the proteins and other soluble factors interfering with the TNF-α measurement, would improve the detection of this CT. Therefore, known concentrations of hrTNF-α were added to the plasma from the children with dengue and the healthy controls, two-fold serial dilutions of the samples were completed, and the TNF-α levels were measured by ELISA. As shown in Figure 5, there were no differences in the detection of hrTNF-α in any of the assessed conditions (undiluted, 1/2 and 1/4 diluted plasma) when the added concentration was low or intermediate (plasma without addition of hrTNF-α, 10 or 100 pg/mL) in the plasma from the children with dengue and the healthy controls (p ≥ 0.5, Friedman test, Fig. 5A). However, when 1,000 pg/mL of hrTNF-α was added, higher levels were recovered in the 1/4 dilution when compared with undiluted plasma in the DENV-infected and healthy children (p = 0.0008, Friedman test, Fig. 5B). In agreement with our previous results, lower than expected concentrations of TNF-α were obtained in each condition (median percentage of recovery of 35% and 28% in the children with dengue and the healthy controls, respectively). Thus, only in the presence of high TNF-α concentrations does plasma dilution improve its detection.
Effect of serial dilutions of plasma in the detection of TNF-α.
Discussion
Several factors affect the measurement of CTs. The type of sample is critical, and some aspects have to be kept in mind during the choice of method. For example, serum lacks coagulation proteins, fibrinogen, and platelets, which can interfere with the measurement, although during the process of coagulation, some CTs such as IL-1β could be released (9). In the case of plasma, the type of anticoagulant is also important, and the use of EDTA results in lower inter-assay variability versus heparin or citrate (20). Here, we observed that plasma strongly correlated with serum in the detection of TNF-α in children with dengue (Fig. 1A), and the evaluation of TNF-α in plasma revealed the biological differences classically reported during DENV infection (Fig. 1B). These data supported the usefulness of plasma, mainly in laboratories where cellular analyses are also performed. The moment of the day in which the samples are taken and their storage and handling also alter the levels of CTs. In this regard, it is advisable to take the samples at the same time of day, due to the circadian rhythm of CTs (48), to minimize the delay in sample processing, store the samples between −70°C and −80°C, and limit the freeze-thaw cycles (25).
The development of multiplexed bead-based assays has allowed the measurement of a high number of analytes in a low sample volume and a short time with acceptable inter- and intra-assay variability (37). Therefore, several reports have compared bead-based assays using the gold standard ELISA (17,26,32,40). Although good degrees of correlation between both methods have been observed, variability is always present, mainly due to the use of assays from different manufacturers and thus distinct antibodies, buffers, and blockers (19). In most cases, the antibodies are raised against recombinant forms of the CTs, and their abilities to detect natural forms of the proteins of interest are less efficient (4). This problem becomes even more complicated due to the large number of reported CT polymorphisms (22). The use of World Health Organization International Standards or Reference Reagents for CTs in all immunoassays could minimize the variability (4). In a large number of studies, the samples analyzed were supernatants from stimulated cultured cells (17,40) or serum from individuals who underwent an induced antigenic challenge (26) where high levels of CTs are expected. Similar to our findings, when low concentrations of plasma TNF-α were found, as in the case of individuals with metabolic syndrome, the CT was detected in the 100% of the samples by ELISA but in only 51% of the multiplexed bead-based assays (32). The variability in the reagents is reflected by these differences, for example, in the detection of two- to 10-fold higher levels of hrTNF-α by ELISA compared to a multiplexed bead-based assay (18), similar to the results reported here. Thus, in the context of a natural and dynamic infection or disease, the comparison between multiplexed bead-based assays and ELISA is challenging.
Most of the studies comparing multiplexed bead-based assays and ELISA used the Luminex technology, and few have evaluated CBA formats (13,52). Our results showed a lack of correlation between ELISA and two CBA formats for the detection of TNF-α in plasma from children with DENV infection (Fig. 2A, B), with a higher rate of CT detection by ELISA. However, these results are not due to a generalized low efficiency of the bead-based assay, as a positive correlation was obtained between both methods when TNF-α was evaluated in a buffer based-solution (Fig. 2C), which is similar to previous reports using tissue culture media (13) and BAL from mice and rats (52).
We measured low levels of TNF-α in the plasma from children with acute DENV infection using both ELISA and CBA, indicating that kinetics, interaction with proteins, lipid concentrations, or CT polymorphisms may affect the measurement (7). TNF-α is produced within the first 3 h after the administration of endotoxin in healthy humans (26) or within 6 h of the inoculation of bacteria in the central nervous system in a murine model of bacterial meningitis, and its levels are undetectable after 24 h (5). As all patients included in this study were between their fourth and eighth days of the illness, their TNF-α concentrations were likely returning to basal levels, and this would, at least in part, explain the low or undetectable concentrations found in plasma (Figs. 1 and 2). To overcome this issue and to explore the effect of plasma on the detection of TNF-α, spike recovery assays were performed and also resulted in low percentages of recovery in the plasma in comparison with that of the tissue culture media (Fig. 3A). The low efficiency in the detection of TNF-α in plasma after the spike recovery assays was independent of the immunoassay, as low percentages of recovery were also obtained by CBA. Together these results indicate that one or more plasma components are affecting the detection of the CT. In contrast, a previous study found high percentages of hrTNF-α recovery through a multiplexed bead-based assay, but this result may rely on the type of detection system used (41).
DENV infection did not affect the poor detection of TNF-α in plasma, ruling out a possible interfering effect of the high levels of sTNFRs in circulation in these children because similar percentages of hrTNF-α recovery in plasma were obtained in healthy controls (Fig. 3B). Previously, it was shown that TNF-α–sTNFRs complexes affect TNF-α quantification (14,36). Additionally, the levels of IL-18 in plasma have been found to be unmodified in DENV or Leptospira infections due to the increase of the antagonist IL-18 binding protein (35). Thus, although we did not directly explore this issue, the interactions of CTs with their soluble receptors or binding proteins should be contemplated, and the simultaneous assessment of both is advised.
False positive or negative results can be caused by the presence of heterophilic- and auto-antibodies in the plasma or serum, which can crosslink capture and detection of antibodies (15). Moreover, the presence of circulating immune complexes, which can act in a manner similar to that of heterophilic antibodies, is another source of assay variability. As increased levels of circulating immune complexes and auto-antibodies have been found in acute DENV infection, mainly in secondary infections (27), these molecules could interfere with the measurement of TNF-α. However, we did not find any difference between the samples with and without immune complex dissociation (Fig. 4B), thus disproving this possibility. In addition, we did not find any difference when the absolute amount or recovery of TNF-α was analyzed between children with primary and secondary DENV infections (data not shown). Of note, the levels of TNF-α naturally induced tended to be lower in the pH-treated versus nontreated samples (data not shown), indicating that the acid treatment could degrade the natural but not the human recombinant CT, which may have affected the results of studies in which this protein was used (16).
To overcome the effect of plasma on the detection of CTs, it would be reasonable to dilute its components with buffer solutions, as recommended by most ELISA and CBA manufacturers (R&D ELISA Reference Guide & Catalog and BD Human Th1/Th2 Cytokine Kit II Catalog) and in previous reports (51). However, although the dilution of plasma improved the recovery of TNF-α, this was only observed when the CT concentration was high (Fig. 5D), which is rarely found during natural DENV infection in children. Indeed, when pure plasma was diluted, the low but detectable levels present in the samples became undetectable (Fig. 5A), which worsened the problem. Thus, this issue remains to be solved, and studies that evaluate this issue are more than necessary.
In summary, our results highlight the factors that affect the detection of TNF-α in plasma from children. A major element is the type of sample, as plasma affected the performance of the ELISA and particularly the CBA. This effect has to be considered when analyzing this CT in plasma.
Conclusions
ELISA was better than CBA for the detection of TNF-α in plasma from children with dengue. Plasma dramatically affects the measurement of TNF-α independent of the condition of the individual or the assay used. This effect of plasma can be partially solved with the dilution of the sample, but only when high concentrations of the CT are expected. The lower efficiency of the detection of TNF-α in plasma should be taken into account when using this type of sample from children with dengue. The effect of serum in the measurement of this cytokine deserves to be carefully addressed in future studies. Thus, the accurate detection of TNF-α in the plasma of children with dengue has shown to be more than a challenge.
Footnotes
Acknowledgments
We would like to acknowledge all the patients who participated in the study, the Departamento de Pediatria and Neumologia, Hospital Universitario de Neiva and Harrison Herrera, Diana Castañeda, Jairo A. Rodríguez, Rocío Vega, and Giovanni Lastra for the recruitment of children and adult patients. This work was supported by COLCIENCIAS, grant code 0735–2013 and the Vicerrectoría de Investigación y Proyección Social, Universidad Surcolombiana (both to CFN).
Author Disclosure Statement
The authors declare that there are no conflicts of interest.