
Abstract
Toll-like receptors (TLRs) may play an important role in hepatitis-B pathogenesis. However, serum TLR-2 and TLR-4 levels and their association with serum liver enzymes, hepatitis B virus (HBV) DNA, quantitative HBsAg levels, and liver biopsy findings, are unknown. A total of naive 40 HBeAg (−) chronic hepatitis B (CHB) patients and 20 healthy control subjects were recruited in this study. Liver tests, HBV DNA, serum TLR-2 and TLR-4, and quantitative HBsAg levels were evaluated among all groups. The relationship among TLR-2, TLR-4, quantitative HBsAg levels and liver tests, and liver histological findings were investigated with correlation analysis. Serum TLR-2 and TLR-4 levels in HBeAg (−) CHB patients were higher than in the control group. There was a positive correlation between serum TLR-2, TLR-4, and HBV DNA and ALT levels. We have further demonstrated that serum TLR-2 levels are correlated with AST and quantitative HBsAg levels. However, TLRs levels were not linked to the liver biopsy findings. TLR can have an important role in hepatitis B pathogenesis. Liver injury in CHB may cause elevated TLR-2 and TLR-4 levels.
Introduction
H
Recently, researchers have shown an increased interest to clarify whether TLR-2 and TLR-4 may play a role in the pathogenesis of CHB. Previous studies have commonly focused on TLR expression in blood samples or tissues samples in CHB patients. However, there is still a discussion about the fact that TLRs are upregulated when the body becomes in CHB. There were some series of experimental studies reported on antigenic structure of HBV and TLR activation. In these studies, addition of HBeAg in cell cultures resulted in inhibition of TLRs (21). In HBeAg-positive patients, TLR-2 activation is significantly reduced compared with HBeAg-negative patients. There was no difference in TLR-4 expression. After HBeAg-positive patients receive treatment and become HBeAg negative and produce anti-HBe antibodies, a reincrease in TLR levels occurs (9). Previous study showed a positive correlation between HBV DNA and TLR, while another showed in a series of liver cirrhosis patients, although TLR expressions were elevated, they were negatively correlated with TLR-2, TLR-4, and HBV DNA levels (16,22). Expressions of TLRs are found to be increased in severe HBV infections and in cases of cirrhosis (5,12,13,16,30). It is a common finding in the literature that TLR-2 expression significantly increases in HBeAg (−) CHB patients, meanwhile inconsistent results are reported regarding TLR-4 expression (3,9,15,18,21,24, 29).
However, TLRs expression measuring methods are commonly difficult and complex analysis. In the same time, there is a lack of data in the relationship between TLRs expression levels and liver tests. Measuring of serum TLRs levels by enzyme-linked immunosorbent assay (ELISA) method is a simple method and provides quantitative values. However, TLR 2–4 serum levels have not been investigated in CHB patients until now (3,5,9,12,13,15,16,18,21,24,29,30).
Recent studies show that quantitative HBsAg levels play significant roles in CHB pathogenesis. Several reports have demonstrated the relationship between HBsAg and immune cells and several cytokines. TLRs increased expression of viral cytokines such as IFN, and proinflammatory cytokines such as TNF-α is observed after TLRs upregulation (24,26). Therefore, TLRs may be related to severity of CHB. However, the relationship between HBsAg quantitative levels and serum TLRs has not been investigated.
Our aim in this study is to evaluate quantitative HBsAg levels together with serum TLR-2 and TLR-4 levels in HBeAg-negative CHB patients and to find out their exact roles in HBV pathogenesis, hepatic histological activity, and fibrosis.
Methods
Subjects
HBeAg-negative CHB group
HBeAg (−) CHB patients aged between 18 and 70 years and admitted to gastroenterology outpatient clinics of Ankara Training and Research Hospital were included in this study. The HBeAg (−) CHB group constituted of patients who were HBsAg (+) previously for at least 6 months and kept being HBsAg negative for the last 6 months plus HBV DNA levels more than 2,000 IU/mL plus persistent or intermittent ALT elevation plus no previous treatment for CHB.
Control group
Control group subjects were randomly sampled from healthy individuals who were found to be HBsAg, Anti-HCV, and Anti-HIV negative on their routine controls.
Exclusion criteria
Healthy subjects and HBeAg (−) CHB patients with chronic renal insufficiency, coronary artery disease, vasculitis, diabetes mellitus, hypertension, cirrhosis were excluded from this study. We also excluded patients who were not using alcohol, had mass lesions on hepatobiliary ultrasonography, and had hepatocellular carcinoma.
Biochemical measurements
Fasting venous blood samples were taken from all patients. Routine biochemical measurements were studied and remaining blood samples were centrifuged and stored at −80°C until the quantitative analyses of TLR-2 and TLR-4, and quantitative HBsAg measurements were performed. All biochemical measurements were undertaken by Abbott Architect C 8000—Abbott system. Viral serological tests were performed by ELISA method for HBsAg, anti-HCV, Vitros ECi Immunodiagnostic, and anti-HBe, antidelta antibodies, while HBV DNA was detected by BİORAD-iCycler İQ Multicolor Real-Time PCR Detection System. Quantitative HBsAg measurement was undertaken by Elecsys (Indianapolis, IN) device of Roche Diagnostics. Serum TLR-2 and TLR-4 levels were measured by ELISA method (Cusabio Biotech, Wuhan, China).
Liver biopsy
Patients in the HBeAg (−) CHB group underwent ultrasound-guided liver biopsy upon internalization into the gastroenterology inpatients clinics. All liver biopsies were evaluated by a single pathologist who did not know about the clinical status of the patients to whom the samples belong. All biopsies were scored using Knodell scoring system (11).
Statistical analyses
Data analyses were performed using SPSS 15.0 software. The normal distribution of the variables was analyzed with Kolmogorov–Smirnov test. Continuous variables are presented as mean ± standard deviation and categorical variables are presented as percentages (%). Parametric variables between the patients and control groups were compared using Student's t test. Nonparametric variables were analyzed with Mann–Whitney U test. The correlation between serum levels of TLRs and HBsAg was evaluated with Pearson correlation test. A p-value <0.05 was delineated as statistically significant.
Results
Study subjects demographical and biochemical results
A total of 60 patients aged between 18 and 70 were included in this study. The number of patients in HBeAg (−) CHB group and healthy control group were 40 and 20, respectively. There were no statistically significant differences between two groups in age, gender, and smoking status (p = 0.586, p = 0.675 and p = 0.458, respectively). The liver enzyme levels and other routine biochemical test results were compared between two groups. ALT, AST, and LDH levels were higher in HBeAg (−) CHB group than in control group (p = 0.001, p < 0.001, and p = 0.008, respectively). Other parameters (total bilirubin, direct bilirubin, urea, creatinine, glucose, GGT, and ALP) were comparably different between groups (all p > 0.05). Thrombocyte count in HBeAg (−) CHB group was significantly lower compared with control group (p < 0.001). Other parameters, erythrocyte sedimentation rate and C-reactive protein levels, were similar in two groups (p = 0.569 and p = 0.302) (Table 1). The HBV DNA level was measured to be 3,070,000 IU/mL (minimum = 4,759, maximum = 109 IU/mL) in HBeAg (−) CHB group. The median quantitative HBsAg level is 7,875 IU/mL (minimum = 413.8 IU/mL, maximum = 50,090 IU/mL) in HBeAg (−) CHB group. When HBV DNA and quantitative HBsAg levels were correlated, a statistically significant strong positive correlation was observed between HBV DNA and HBsAg levels (rho = 0.830, p < 0.001).
CHB, chronic hepatitis B; CRP, C reactive protein; HBV, hepatitis B virus.
Liver biopsy findings
Liver biopsy was performed to all 40 patients in HBeAg-negative CHB group. The median histological stage index was 5 (2 –10), and the median fibroblastic stage was 2 (0–4). When the findings of liver biopsy were correlated with HBV DNA and quantitative HBsAg levels, we observed a positive correlation of HBV DNA with HAI (rho = 0.403, p = 0.037), but HBV DNA levels were not correlated with fibroblastic stage (p = 0.180). Quantitative HBsAg levels did not show any correlation with HAI and fibroblastic stage (p = 0.375, p = 0.570).
Serum TLRs levels
TLR-2 levels were 0.88 ± 0.82 ng/mL and 1.39 ± 1.19 ng/mL, respectively, in control group and HBeAg (−) CHB group. There was statistically significant difference between HBeAg (−) CHB group and control group (p = 0.022) (Fig. 1). TLR-4 levels were significantly higher in HBeAg (−) CHB group compared with control group. TLR-4 levels were 0.14 ± 0.06 ng/mL and 0.55 ± 1.38 ng/mL (p < 0.001), respectively, in control and HBeAg (−) CHB group (Fig. 2).
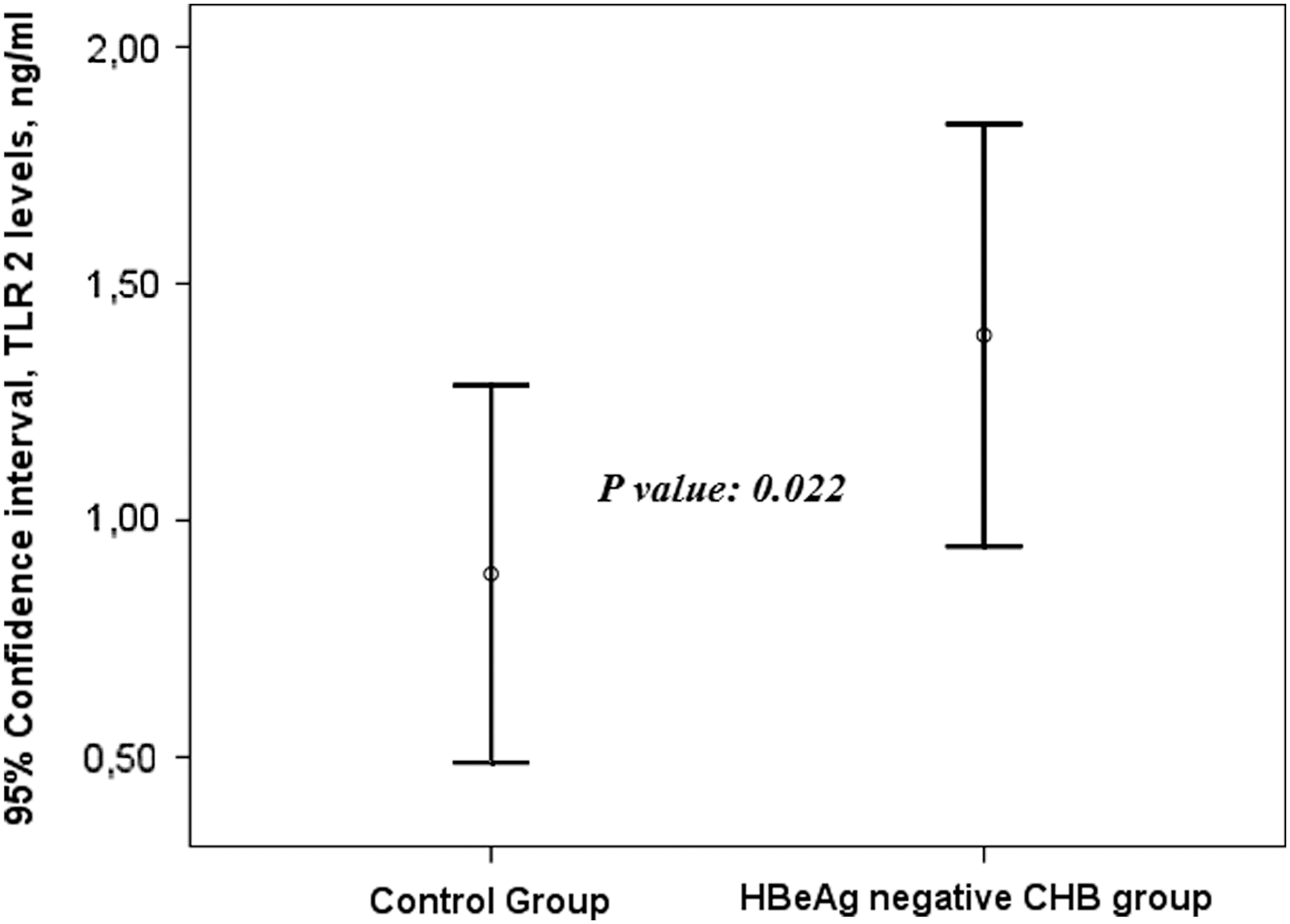
Serum TLR-2 levels show in control and HBeAg CHB patients. TLR, toll-like receptor; CHB, chronic hepatitis B.

Serum TLR-4 levels show in control and HBeAg CHB patients.
Correlation analysis
When the correlation of TLR-2 and TLR-4 levels with HAI, fibroblastic stage, quantitative HBsAg, HBV DNA levels, AST, and ALT were evaluated, TLR-2 positive correlated with HBV DNA (rho = 0.399, p = 0.005), ALT (rho = 0.302, p = 0.037), AST (rho = 0.285, p = 0.047), and quantitative HBsAg (rho = 0.432, p = 0.027) was noted. TLR-2 levels were not correlated with HAI and fibroblastic stage (p = 0.887, p = 0.804). We detected that a positive correlation among TLR-4, HBV DNA (rho = 0.447, p = 0.001), and ALT (rho = 0.386, p = 0.006), but there was apparently no correlation of TLR-4 with other parameters (Table 2).
TLR, toll-like receptor.
Discussion
To study for the first time, we investigated the serum TLR-2 and TLR-4 levels with ELISA method. We also evaluated serum TLR-2 and TLR-4 levels that associated with liver enzymes, HBV DNA, quantitative HBsAg levels, and liver histological findings. We detected that serum TLR-2 and TLR-4 levels increased in HBeAg (−) CHB patients, and they are also associated with ALT and HBV DNA levels. Indeed, serum TLR-2 levels are associated with quantitative HBsAg levels and AST levels. However, serum TLR-2 and TLR-4 levels are not linked to liver histological findings.
In our study, serum levels of TLR-2 were detected to be higher in HBeAg (−) CHB compared with the control group. Most probably, increased serum TLR-2 levels are reflecting to HBV antigenic stimulus. HBV DNA and HBsAg are important antigenic stimulus for started immunopathological response in CHB patients. The pathogenesis and clinical manifestations of hepatitis B are due to the interaction of the virus and the host immune system. The in vitro and in vivo studies to date show that TLRs can play an important role in the pathogenesis of HBV (9,11,13 –16,18,20,23,27 –30). Increased expression of TLR-2 in peripheral blood monocytes and liver biopsy specimens with CHB patients has been shown (14,18,21,24,26,31,32). Previous studies on HBV-infected cell cultures have shown that expression of TLR-2 is increased (5,8,12,13). TLR-2 plays an important role in the pathogenesis of HBV-related liver damage through increasing proinflammatory cytokines, IFN secretion, and activation of monocyte macrophage system. TLR-2-dependent induction of type I interferon occurred only in response to viral ligands and also in CHB induces the production of type I interferon (1).
There are few studies whether expression levels of TLR-2 can be related with HBV DNA and HBsAg levels. These studies have shown different results as these studies used different methods of measuring TLR-2 levels and at different stages of CHB. A study previously showed a positive correlation between HBV DNA levels and expression of TLRs (22). Another study showed expression of TLR-2 and TLR-4 negative correlated with HBV DNA levels in a series of liver cirrhosis patients (16). Our findings show that there is a significant positive correlation between serum TLR-2 and HBV DNA levels. Our results indicated that HBV DNA levels are an important factor for elevation of serum TLR-2 levels. Similar mechanisms can be said about TLR-4, because our study revealed that serum TLR-4 levels were positively correlated with HBV DNA levels. On the contrary, we did not detect that serum TLR-2 and TLR-4 levels were not linked to liver biopsy findings, histological activity, or fibroblastic stage. Only we showed that HBV DNA levels were related to HAI. Thus increased serum TLR-2 and TLR-4 levels did not seem a good estimate of the severity of liver biopsy findings.
HBsAg is the other important antigenic stimuli for TLRs activation. However, there was no study evaluating the relationship between quantitative HBsAg and TLR-2 or TLR-4. Wang et al. showed that the HBsAg was related to decreased cytokine production induced by the TLR-2 ligand from CHB (25). Our study results show that quantitative HBsAg are positively correlated with serum TLR-2 levels. Therefore, we think that increased HBsAg levels are related to immunological response in CHB patients. Our study demonstrated that TLR-4 levels were not associated with quantitative HBsAg levels. There might be several reasons for these results. First and more important cause, TLR-4 expression role of CHB pathogenesis are not clear compared with TLR-2 expressions. Previous studies showed that TLR-4 activation related to the induce of IFN-β. However, the relationship between increased TNF-β and inhibition HBV replication in hepatocytes is not exactly known (31). Other reason is that this study included relatively a small number of patients. It would be interesting to confirm these results with larger number of patients. In addition, this study did not include HBeAg-positive patients. HBeAg is one of the most important antigenic stimuli for started immune defense. Therefore, serum TLR-2 and TLR-4 levels would be performed investigating different stage of CHB. Another important result is that serum TLR-2 and TLR-4 levels are positively correlated with ALT levels. A previous study showed that serum TLR-2 levels were correlated with ALT levels in HBeAg (−) CHB patients (17). However, this study did not include control subjects. Our study serum TLR-2 and TLR-4 levels were associated with ALT levels in CHB patients; however, they were not linked in histopathological findings of liver biopsy.
In conclusion this study analyzed for the first time the serum TLR-2 and TLR-4 levels with ELISA method, and their relationship with HBV DNA, ALT, and quantitative HBsAg levels were analyzed in HBeAg (−) CHB patients. Serum TLR-2 and TLR-4 measuring with ELISA methods were similar to previous studies, which included TLR-2 and TLR4 expression in CHB patients. ELISA is a useful method to reflect TLR-2 and TLR-4 activation. Indeed HBV DNA and HBsAg play an important role in TLR-2 activation in HBeAg (−) CHB patients.
Footnotes
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
The authors declare no competing financial interest.