
Abstract
Besides liver cirrhosis and hepatocellular carcinoma, chronic hepatitis C virus (HCV) infection is associated with many extrahepatic manifestations (EHMs). HCV exhibits lymphotropism that is responsible for various EHM. An important characteristic of HCV is escape from the immune system, which enables it to produce chronic infections and autoimmune disorders along with accumulation of circulating immune complexes. These EHMs have large spectrum, because they affect many organs such as heart, lungs, kidney, brain, thyroid, and skin. HCV-related cardiac and pulmonary manifestations include myocarditis, cardiomyopathies, cardiovascular diseases (i.e., Stroke, ischemic heart disease), chronic obstructive pulmonary disease, idiopathic pulmonary fibrosis, asthma, and interstitial lung diseases. This review discusses etiology and pathogenesis of HCV-associated cardiac and pulmonary manifestations and how different genes, immune system, indirectly linked factors (mixed cryoglobulinemia), liver cirrhosis, and antiviral treatment are involved in HCV-related heart and lung diseases, however, their exact mechanism is not clear.
Introduction
H
The HCV infects about 3% of world population, while 17–37% HCV-infected people also suffer with HCV-related heart diseases (51). The most common cardiac manifestations are cardiomyopathies, myocarditis, atherosclerosis, cardiovascular disorders (stroke and ischemic heart disease), coronary artery disease (CAD), and peripheral artery disease (PAD) (28). Along with heart diseases, HCV-associated pulmonary complications are also reported. HCV-related lung pathologies could be the primary outcome of the infection, however, there are certain other pathologies such as pulmonary vasculature and damage of pulmonary parenchyma attributed to mixed cryoglobulinemia (MC), interferon therapy liver cirrhosis (60), hepatopulmonary syndrome, and portopulmonary hypertension (3). The primary or direct outcomes of the HCV infection on lung pathologies include the chronic obstructive pulmonary disease (COPD), idiopathic pulmonary fibrosis (IPF), asthma, and interstitial lung diseases (60).
In this study, we will discuss the etiology and pathogenesis of HCV-associated cardiac and pulmonary manifestations and how different genes, immune system, indirectly linked factors (diabetes and cryoglobulinemia), and antiviral treatment contribute to the HCV-related cardiopulmonary diseases.
HCV-Related Cardiomyopathies and Myocarditis
Cardiomyopathies can be defined as a group of heterogeneous diseases of myocardium. It includes idiopathic dilated, hypertrophic or restrictive disease cardiomyopathies, arrhythmogenic right ventricular cardiomyopathy, and inflammation of the myocardium or myocarditis (66). One of the major reasons of myocarditis is cardiotropic viruses (66) such as enteroviruses, coxsackievirus B, adenovirus, and parvovirus (52). Recently, a high prevalence of HCV infection has been noted in patients with hypertrophic cardiomyopathy, dilated cardiomyopathy (DCM), and myocarditis (49). Among all of the HCV-associated cardiac disorders, DCM is a relatively common disorder, which may lead to severe heart failure. Besides this, HCV infection causes induction of proliferative stimuli that lead to the formation of myocytes responsible for cardiomyopathy and hypertrophic cardiomyopathy (HCM). HCM refers to a heart defect characterized by increased thickness of the wall of the myocardium, mostly left ventricle, causing functional impairment of the heart.
It is possible that both direct viral cytotoxic and indirect immune-mediated mechanisms of myocardial tissue damage are crucial in the pathogenesis of viral-induced cardiac disease (40). Previously, immunological mechanisms were described for chronic liver disease-mediated myocarditis and cardiomyopathies. Patients having chronic HCV-mediated myocarditis had normal serum levels of hepatic transaminases, until the final stages of heart failure (51). In case of congestive hepatopathy, the main driver of this condition is activation of cytotoxic T cell response in liver tissue. When protein products of HCV stimulate the toll-like receptors, CD4+ cell-mediated T helper-1 (Th1) response is induced, which results in release of interleukin-12 (IL-12), interferon (IFN)-α and -β from monocytes, macrophages, and neutrophils. Highly activated CD4+ cells produce IFN-γ, which stimulates the macrophages to produce proinflammatory cytokines. IL-1 and tumor necrosis factor alpha (TNF-α) are the two major cytokines produced by macrophages, responsible for recruiting inflammatory cells and factors toward the myocardium (71). This mechanism suggests that chronic HCV can act as a risk factor for the development of myocarditis and subsequently to cardiomyopathies (Fig. 1).
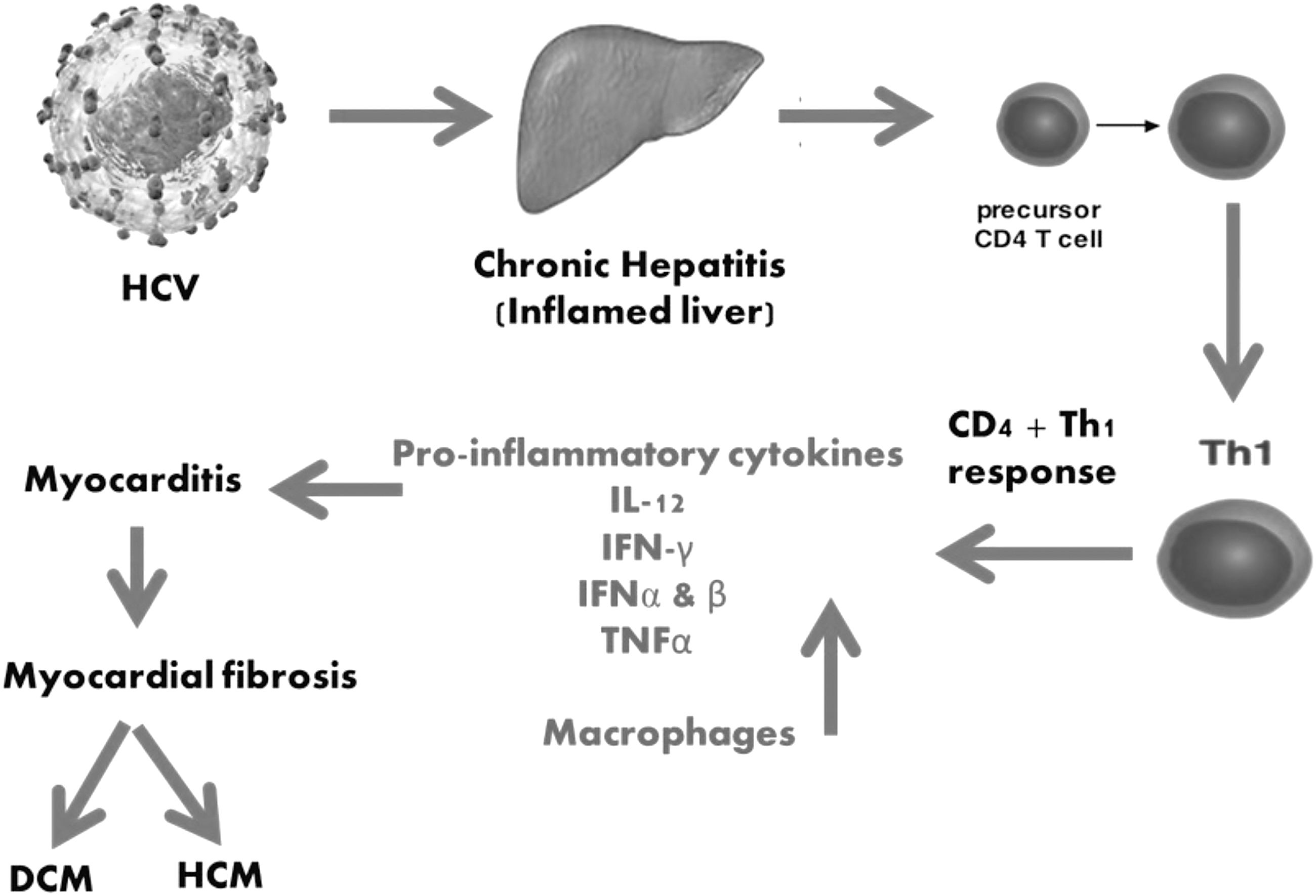
Postulated behavior of the HCV-mediated immune activation, resulting development of myocarditis, which ultimately leads to cardiomyopathies. DCM, dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy; HCV, hepatitis C virus; IFN-α, interferon alpha; IL-12, interleukin-12; Th1, T helper-1; TNF-α, tumor necrosis factor alpha.
Many studies have shown a stronger association between increased expressions of TNF-α and depressed myocardial function with its increasing concentrations in plasma and myocardium of patients. The TNF-α binds to two different receptors (TNF-α receptor 1 [TNFRI] and TNF-α receptor 2 [TNFRII]) present on the surface of cardiomyocytes, and cause negative inotropic effects. In cardiac myocytes, contraction and relaxation depend on cyclic release and removal of calcium ions from the sarcoplasmic reticulum (84). Extracellular calcium ions enter the cell via L-type Ca+2 channels during membrane depolarization and help in the release of calcium ions from the sarcoplasmic reticulum. The SR Ca+2/Mg+2-ATPase (SERCA) present in the sarcoplasmic reticulum of myocytes is involved in the calcium uptake during muscular movement and higher concentrations of TNF-α restrict L-type Ca+2 channels and affect the systolic phase by inhibiting high concentration of calcium ions (87). It also affects the relaxation phase by inhibiting SERCA (16).
Another mechanism by which TNF-α affects the myocardium is by stimulating the production of nitric oxide (NO), which acts as an endogenous inhibitor and has a negative inotropic effect on the myocardium. In the presence of proinflammatory cytokine (TNF-α), the concentration of inducible nitric oxide synthase (iNOS), (calcium independent, a nonexpressive isoform of NO synthase) is increased. Expression of iNOS in the myocardium causes the decrease in the contractile function of the heart and isolated cardiomyocytes (71).
Autoimmunity is another important mechanism of HCV-linked myocarditis and DCM. The presence of some human leukocyte antigen (HLA) and non-HLA haplotypes genetically predispose some HCV patients toward HCV-associated cardiomyopathies (71). All human HLA class II loci (HLA-DP, HLA DQ. HLA-DR) show polymorphism, which affects the epitope's affinity to bind with different peptides involved in the pathogenesis of some autoimmune diseases (11). In HCV-related cardiomyopathies, certain genes have been found to play their roles. The gene for human major histocompatibility complex (MHC) is located on the short arm of chromosome 6 and encodes for several protein products involved in immune function, including complement, TNF-α, and HLA complex. Any polymorphism in this gene is proposed as determinant for the susceptibility to various diseases.
MHC class II genes may play their roles, in conferring susceptibility to HCV infection, and may influence the development of different phenotypes of cardiomyopathy (62). Recently, several studies have reported that dilated and hypertrophic cardiomyopathies are associated with certain alleles of the HLA system. For example, the HLA-DPB1*0901 and HLA-DRB1*1201 have been reported to be more prevalent in chronic HCV-infected patients who develop DCM, and HLA DRB1*0901 and DQB1*0303 haplotypes are more prevalent in chronic HCV-infected patients with hypertrophic cardiomyopathy (50). Another study described that HCV-linked DCM was due to alleles of non-HLA genes rather than with those of the HLA genes. Specifically, a group of investigators mapped the gene factor, responsible for HCV-related DCM at non-HLA gene locus spanning from the NF-kappa-B inhibitor-like protein 1 (NFKBIL1) to the MHC class I chain-related protein A (MICA) gene loci within the MHC class III-class I boundary region (78).
Cardiovascular Diseases
Chronic hepatitis C (CHC) is a major independent risk factor for the development of cardiovascular diseases (CVDs), including atherosclerosis, cardiovascular disorders (stroke and ischemic heart disease), CAD, and PAD (15). According to the World Health Organization, stroke and ischemic heart disease are the two major causes of death worldwide. People suffering from chronic HCV have increased risk of CAD, PAD, and cerebrovascular disease (28). CHC also develops the major risk factors for other metabolic diseases such as insulin resistance (IR), diabetes mellitus (DM), atherosclerosis, and hypertension (39).
It has been assumed that HCV promotes atherogenesis and causes CVDs by stimulating different biological mechanisms. These mechanisms involve liver steatosis, fibrosis, diabetes, IR, HCV colonization and proliferation within arterial walls, excessive and imbalance production of cytokines, oxidative stress, endotoxemia, and hyperhomocysteinemia (89). Among the various CVDs, HCV mainly promotes the atherosclerosis. Recent studies indicated that HCV is associated with carotid atherosclerosis and carotid intima-media thickness independent of other risk factors of CVDs (35). In a cross-sectional study, association between HCV and carotid artery plaques was indicated by the presence of anti-HCV antibodies and HCV core protein in the serum of HCV-affected patients (36). HCV infection is associated with coronary artery plaques and high levels of HCV-mediated plaque calcification.
HCV infection increases the risk of developing PAD. PAD responsible for the development of calcium and fat plaques in the arteries, which upon increase in size lead to atherosclerosis (32). Some data from a Taiwanese study indicated that HCV-infected patients are at higher risk of developing PAD compared with noninfected patients. The incidence of PAD development in HCV-infected patients occurs in the first and third years of disease (12). HCV chronic infection and related inflammation may be associated with several unfavorable pathologic conditions, including atherosclerosis (6). Chronic HCV infection causes liver fibrosis, which induces metabolic changes that are involved in the production of atherosclerosis (39). In HCV-infected patients, atherosclerosis is the main cause of strokes and heart attacks. It has been reported in different studies that HCV infection is an independent risk factor for strokes, cerebrovascular diseases, and ischemic heart diseases. HCV-infected patients showed a marked association between inflammatory markers and atherosclerosis (12).
The liver is a major inflammatory regulator; it regulates both local and systemic inflammation by the production of molecules having inflammatory-inducing properties. When HCV infects liver, inflammatory cascade begins. Proinflammatory and inflammatory cytokines, including IL 1-β, TNF-α, and -β, are produced, which cause local inflammation and fibrosis (90). Steatosis is another factor that has contributed in the mechanism of EHM of HCV via the production of inflammatory markers such as IL-6 and TNF-α. These molecules play roles in the inhibition of insulin signaling pathway, and adiponectin levels subsequently results in the progression of steatosis and IR (43). In some HCV patients, a high level of inflammatory markers due to steatosis is a major cause of CAD (9). The other mechanism that causes inflammation due to HCV is oxidative stress. Imbalance between antioxidants and reactive oxygen species is linked with local and systemic inflammation. Other factors that are involved in oxidative stress damage include necrosis, tissue regeneration, apoptosis, ischemia, and fibrinogenesis (89) (Fig. 2).
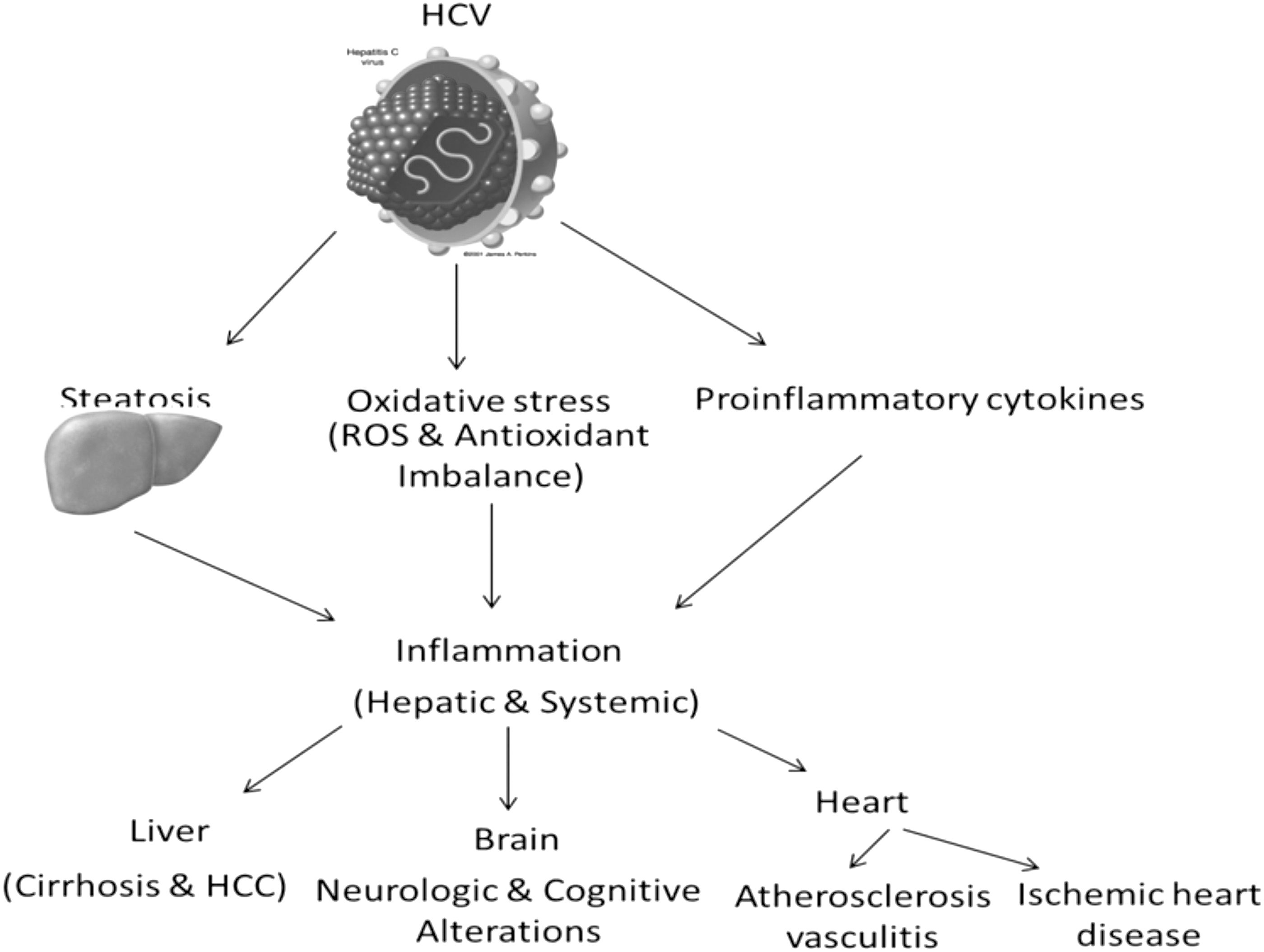
Factors related to HCV that cause chronic inflammation, which plays a role in hepatic and systemic manifestations. HCC, hepatocellular carcinoma.
Idiopathic Pulmonary Fibrosis
IPF is a chronic disease of the lungs that includes low-grade inflammation of alveoli, leading to the derangement of lung interstitium. IPF usually develops in cases of chronic HCV infection (19). It is characterized by the accumulation of extracellular matrix, impaired gas exchange, and worsening dyspnea (58,88). Various pathologic features of IPF include epithelial cell injury, diffuse alveolar damage, variable inflammation, lung damage and fibrosis, and temporal and spatial heterogeneity in lung areas (27,58). The precise cause for the IPF is unknown (67), however, HCV is said to be a triggering agent for inflammation in the lung interstitium that leads to lung fibrosis (23,64). The relationship between HCV infection and IPF was confirmed by a retrospective study, which reports 11% of patients with HCV-induced cirrhosis, who also showed obstructive airway disease (4).
There are many factors that contribute to the chronic lung diseases such as persistent antigens, viral infection, lung injury, and immune cell activation (47). HCV-related IPF is said to be an outcome of occult infection, in which virus (an inflammatory agent) disrupts the normal healing process of the lung, resulting in lung fibrosis (70). In case of IPF, both lytic and latent viruses have found to play their roles in causing lung fibrosis. In case of IPF, HCV RNA is also detectable in bronchoalveolar lavage (BAL) fluid, and in lung biopsies of patients, indicating the direct involvement of the virus in IPF (8), however, the presence of HCV-RNA at lower quantity is indicative of virus airway transmission; as no difference was found between the T cell and B cell populations among the cases and controls (34). Certain other immune cells, such as neutrophil, eosinophil, macrophages, mast cells, and fibroblast cause some nonspecific inflammatory reactions (47), ultimately resulting in lung fibrosis. In HCV patients, immune complexes found to have no role in causing the IPF, because fluorescence microscopy of the lung biopsies has not revealed any immune complex.
There was a high prevalence of anti-HCV antibodies against the C100-3 antigen (a polypeptide containing 363 amino acids) of HCV in the sera of IPF patients (82). In HCV-related IPF, virus-induced immune-mediated fibroblast activation is thought to have a key role in pathogenesis (17), as these fibroblast cells are activated after the viral infection. With these activated fibroblasts, epithelial cells, mast cells, monocytes, and macrophages have found to release higher levels of IL-10, IL-13, and IL-4 (47). IL-4 and IL-13 act as proinflammatory mediators and either directly or indirectly affect the fibroblast activation (85). In this type 2 cytokine environment, an increase in the levels of IL-4 and IL-13 results in the production of increased extracellular matrix proteins and fibroproliferation. Excessive deposition of the extracellular matrix proteins in the lungs causes pulmonary fibrosis (85).
IPF can also be an outcome of autoantibodies produced in response to the HCV infection as there is a relationship between the Jo-1 autoantibody and IPF (83).
From the published data, various evidences have been provided for viral etiology of IPF. The conditions of IPF+HCV patients were improved when treated with antivirals, valacyclovir and ganciclovir (58,88). In addition to this, IPF+HCV patients have higher mean age suggestive of the immunosenescence, particularly in case of viral infections (25,59), along with different spatial or temporal morphology of the lung indicative of reminiscent infection (27,58). Besides this, a large population of activated lymphocytes is observed in the BAL fluids of IPF patients with enhanced expression of the host defense genes (58,59,86).
Chronic Obstructive Pulmonary Disease
COPD is characterized by a chronic inflammation of the lung parenchyma tissue with varying degree of airway obstruction (60). COPD can be a result of spontaneous pulmonary reactions, or sometimes it develops in response to certain medical treatment. In 1990, COPD was considered as the sixth most common cause of death that is estimated to be the third most common cause of death in 2020 (79). COPD is characterized by the fixed airflow restriction and forced expiratory volume (FEV) as these factors can be used as prognostic markers for the disease (79). Various viral infections aggravate the previously caused COPD and asthma (58). HCV can either initiate or increase the severity of the disease, as HCV+COPD have reduced values for pulmonary function tests, including FEV1 and carbon monoxide diffusion capacity of the lungs (DLCO) values, compared with the HCV-COPD patients (79).
HCV exacerbates the COPD directly by causing chronic inflammation due to latent viral infection and indirectly by triggering the HCV-specific T-Lymphocytic response. Besides this, HCV infection reduces the lung functions in patients suffering from COPD. In patients with COPD, the disease conditions mainly worsened due to the chronic HCV conditions. In a study, various anthropological factors such as mean age, sex, exposure to environmental pollutants, risk factors for acquisition of HCV, and smoking habits were assessed to find their associations with HCV. A significant difference has been found only in the mean age of the two groups, as patients with HCV and COPD have higher mean ages compared with those with HCV and no COPD (77), thereby suggesting an association between chronic HCV, with longer duration to COPD. In patients with HCV and increased mean ages, there is a long period of immune activation and inflammation due to chronic viral infection that aggravates the COPD. Because of long-term viral replication in the body, the expression of CD8+ T lymphocytes is upregulated. This upregulation activates a cascade of inflammatory pathways resulting in the release of inflammatory mediators, which causes the airway obstruction in COPD (60). In addition, in HCV patients, increased level of IL-8 causes the inflammatory response in the body as well as suppresses the action of IFN-γ (79).
Mixed Cryoglobulinemia
Cryoglobulinemia is a blood disorder, characterized by the presence of special blood immunoglobulins called cryoglobulins. The MC is a systemic vasculitis with various clinical symptoms (23). Cryoglobulins are common in the blood of HCV patients, as MC is found to be the most common and severe EHM of HCV infection (70). The association of MC with HCV has been defined on the basis of its higher prevalence and pathogenesis in HCV patients (93). Cryoglobulins starts to precipitate or deposit in the vessels when blood is chilled (below 37°C), thus restricting the blood flow in vessels resulting in vasculitis (24,94). Longer duration of HCV infection and clonal B cell expansion in hepatocytes is among the many factors that cause MC (68,75). Along with many other complications of MC, pulmonary hemorrhage and cardiovascular disorders are found to be common in HCV patients (65). Among the patients of HCV, percentage of MC-affected patients is 19–50% (26), however, its prevalence varies with the geographical heterogeneity. In HCV patients the organs that are mostly affected by MC include the lungs, joints, nerves, and kidneys (70).
In HCV patients, MC is the result of antigen-driven lymphoproliferative process of B cells. HCV is known to reside on the peripheral lymphocytes circulating in the body where it replicates and increases its number. HCV has ability to bind with the CD81 ligand present on the B-Lymphocyte through E2 protein. E2 protein present on viral envelope mimics the human IgS (26), thus, it activates complement cascade, resulting in the formation of immune complexes upon its binding to CD81 (33). Furthermore, this binding triggers expression of a special set of genes encoding the variable region (VH, VK) of immunoglobulins and of those involved in production of IgM-RF with cross-reactive WA-idiotype (69,94). In type 2 MC, gene expression results in the production of polyclonal antibodies (IgG) followed by production of monoclonal antibodies (IgG, IgM, and IgA) after the emergence of a single-type dominant B cell. While in case of type 3 MC, only polyclonal (IgG, IgM) antibodies are produced (26). In addition, the presence of cryoglobulins mainly complexed with HCV RNA (70) in patients of HCV+MC further indicates the involvement of HCV in causing MC.
Cardiovascular manifestations of MC include ischemic heart disease with coronary vasculitis, valvular heart disease with mitral valvular damage, pericarditis, acute myocardial infarction, congestive heart failure, and dilative and hypertrophic cardiomyopathies (5). Pulmonary alterations that are mostly resulted from MC are mild in nature, while sometimes they lead to the severe outcomes such as diffuse alveolar damage and organizing pneumonia. In HCV patients, various cytokines, inflammatory cells, and immune complexes act as major contributors of heart diseases, however, in the serum of MC+HCV patients, there is a direct involvement of viral antigens (bind with immunoglobulins) and various immune complexes that ultimately deposit in lung interstitium (23).
In patients with HCV and MC, various B cell subsets and autoantibodies are observed, which cause lung fibrosis. CIC comprises IgG, IgM, IgA, C3, and C4 and were detected in HCV patients with heart diseases in different proportions. For example, patients with valvular disease present high levels of C3, however, the levels of IgM are higher in patients with myocarditis (14). Cytokine zTNF4 (a member of the tumor necrosis factor family) was found at higher levels in patients with MC-linked HCV. CXCL10-mRNA is overexpressed in hepatocytes in HCV patients and plays a role in the pathogenesis of disease through recruitment of inflammatory cells (T cells) to the site of inflammation. Presence of high levels of CXCL10 in serum results in histological severity and globular inflammation. In HCV+MC patients, certain genetic mutations also play their roles in overexpansion of the B cell community. Among these mutations, there includes translocation of the bcl2 gene. This mutation results in the overexpression of antiapoptotic bcl2 gene, resulting in increased survival of B cell populations (76,94).
Cardiopulmonary Diseases Related to Liver Cirrhosis
HCV is one of the major causes of liver cirrhosis in the world. Chronic liver inflammation is responsible for liver cirrhosis that leads to severe liver diseases such as liver cancer and liver failure. Cardiac and liver diseases are mutually interrelated (63). The major cardiac manifestations that arise due to liver cirrhosis are cirrhotic cardiomyopathy (CCM), pericardial effusion, systolic and diastolic dysfunction, and noncirrhotic high-output heart failure that occurs due to hepatic arteriovenous shunts. The exact definition of CCM was reported in 2005 by experts in annual meeting of the World Gastroenterology Organization (57). The main clinical features of CCM are cardiac dysfunction (systolic and diastolic), hyperdynamic circulation, and abnormal electrophysiological findings (73).
In patients suffering from chronic liver diseases, cardiac dysfunction is the main heart problem that depends on many factors. These factors include defects in the cardiac β-adrenergic receptor system, plasma membrane fluidity, abnormalities in the membrane calcium channels, and pathological effects of many humoral factors such as NO, cytokines, carbon monoxide, and endocannabinoids (56). HCV-related CCM shows three major pathophysiologic abnormalities, which include cardiac electrophysiological abnormalities, structural and functional ventricular abnormalities, and abnormal ventricular response to stress (44). Other cardiac manifestations related to cirrhosis are endocarditis, arrhythmias, and tachycardia (45). Arrhythmias are associated with hepatic pulmonary syndrome. In liver cirrhosis, different markers such as natriuretic peptides, cytokeratin 18, TNF, and microRNAs are produced in high number. These biomarkers are used to access cardiac diseases due to chronic liver diseases (61). Despite many pulmonary diseases that are attributable to the lymphoproliferative nature of HCV, certain pulmonary alterations can be the direct outcome of advanced liver diseases such as liver cirrhosis in HCV patients. Among these outcomes, there include hepatopulmonary syndrome and portopulmonary hypertension (29).
Hepatopulmonary syndrome is characterized by altering gas function in the lungs and shunting of blood from right to left side because of the intrapulmonary vascular dilatations. Any level of liver damage, including liver cirrhosis and portal hypertension, contributes to disease. Among the HCV patients, it is more prevalent among those who are suffering from the advanced liver diseases (20,29). Until now, endothelial cell injury in the lungs has been said to be a main reason for the intrapulmonary vascular dilatations. In HCV patients, endothelial cell injury occurs due to increased levels of bile acid and cytokines (TNF-α). Bile acids are produced due to liver cirrhosis, while cytokines mainly result from HCV-induced immune activation (29,30). TNF-α is known to perform the proinflammatory function that further promotes the leukocyte–endothelium interaction or sometimes activates the arachidonic acid pathway (70). The second outcome of advanced liver diseases is portopulmonary hypertension. It is characterized by the altered pressure in the pulmonary arteries and veins. About 5% of the patients suffered from cirrhosis also develop portopulmonary hypertension (29).
HCV Antiviral Therapy and Cardiopulmonary Complications
Before 2011, the approved therapies for treating the chronic HCV infection include IFN, PEGylated IFN-α alone, or in combination with ribavirin (RBV) (42). IFN and RBV combination is in use for treating the HCV infection, however, PEGylated IFN α-2b is approved for the treatment of chronic HCV as a monotherapy. Antiviral-related lung pathologies are mostly rare, but are potentially fatal with an incidence of 0.4% to <1% (13). The spectrum of these pathologies includes diverse outcomes such as interstitial pneumonitis, bronchiolitis obliterans organizing pneumonia (BOOP) (secondary organizing pneumonia), pulmonary sarcoidosis, pleural effusion, and exacerbation of asthma (13). Interstitial pneumonia (IP) and sarcoidosis are among the well-documented complications of the IFN therapy of HCV patients (3). The incidence rate of IP is estimated to be 0.01–0.3% (37).
The exact mechanism for the toxicity of lungs by IFN-α is not well understood, however, IFN-α causes the inhibition of suppressor T cells and enhances the expression of cytotoxic T cells (55). In addition, it increases the release of fibrinogenic cytokines, thus causing the lung injury. In the presence of higher level of type 2 cytokines (IL-13 and IL-4), the extracellular matrix proteins produced by activating myofibroblast cells start to deposit in the lung tissues, thereby causing the lung tissue fibrosis (85). Pulmonary sarcoidosis is another IFN-α-related complication resulted from the stimulation of Th1 response and macrophages, along with the induction of autoantibodies due to IFN therapy (2). The mechanism is known to cause pulmonary sarcoidosis, granuloma formation in lung tissues, and macrophage activation due to dysregulated IFN-γ.
To date, only few cases of IFN-related sarcoidosis have been reported in patients of myelogenous leukemia, multiple myeloma, and HCV (1,2,54). IFN treatment is also responsible for causing pulmonary arterial hypertension (PAH) in HCV patients (72). Cardiovascular complications due to PEG-IFN-α include congestive heart failure, myocardial infarction, life-threatening arrhythmias, ischemic heart disease, CAD, pericarditis, and DCM (38). These cardiac complications occur only after prolong treatment of IFN-α therapy. Anemia is a common outcome of Peg-IFN/RBV treatment in many HCV patients, however, some patients who have CAD cannot tolerate anemia (18). Besides this, DCM was completely resolved when Peg IFN-α and RBV therapy was stopped (92).
In the United States, the triple therapy, including the RBV, PEGylated IFN, and protease inhibitors (boceprevir and telaprevir), has been adopted in 2011 (80). The direct acting antivirals (DAAs) reduced the duration of therapy up to 24–28 weeks in ∼50% of patients, while responsible for the improvement in sustained virological response (SVR) rate in naive and experienced patients. These benefits could be achieved only when DAAs are used in combination with peg-IFN/RBV (91), but the treatment is not effective in case of patients suffering with cirrhosis. In last 3 years, DAAs revolutionized the treatment of HCV by using multiple classes of DAAs in IFN-free regimens (46).
Until now a large number of antivirals have been approved by the European Medicine Agency (EMA) and the Food and Drug Administration (FDA) starting with boceprevir and telaprevir in 2011 for the treatment of HCV genotype 1, followed by the approval of four new protease/polymerase inhibitors: sofosbuvir, simeprevir, daclatasvir, and ledipasvir, and a NS3/4A protease inhibitor asunaprevir in 2014 (74). A new combination of ombitasvir/paritaprevir was also approved as a treatment option for HCV in the year 2015. Recently in 2016, another combination of grazoprevir/elbasvir has been recommended by EMA. These antivirals are associated with higher SVR rate (90–100%) as it has been proven from various pivotal studies (53). Use of multiple classes of the DAAs has been proven to be effective in cirrhosis patients because short and tolerated regimens increased the SVR rate up to 95% (22). This treatment has limited EHMs, but mostly it affects the kidneys.
Although the efficacy of DAAs therapy is higher, it has some severe side effects such as lymphopenia, hemolytic anemia, and decomposition of cirrhosis (80). These side effects also favor the lung infections by bacterial pathogens such as mycobacterium abscessus (80). Pneumonia is another outcome of cirrhotic HCV patients who were given DAA therapy. DAAs are responsible for the cardiovascular manifestation in those HCV patients suffering with DM (48). The most common side effects of the DAAs include fatigue, headache, nausea, and insomnia. Percentage of HCV patients suffering with anemia is lower when treated with simeprevir/sofosbuvir compared with the RBV, however, two serious complications, including renal failure and aspiration pneumonia, were considered for treatment-related patients' death. Besides, this simeprevir and sofosbuvir were also associated with pulmonary manifestations, including mild diffuse emphysema, PAH, and interstitial pneumonitis (31,81). Among various DAAs, ombitasvir/paritaprevir/ritonavir and dasabuvir were found to have serious pulmonary and cardiac complications, including acute respiratory failure, sinus tachycardia, ventricular extrasystoles, and acute transient stroke (21).
Conclusion
Although HCV causes the liver cirrhosis and hepatocellular carcinoma, chronic HCV infection is involved in many EHMs that affect every organ specially heart and lungs via a variety of mechanisms. The crucial cardiopulmonary diseases related to HCV include myocarditis, cardiomyopathies, CVDs, strokes, COPD, IPF, asthma, and interstitial lung diseases. Mostly cardiopulmonary manifestations of HCV are immune-mediated and some occurred due to chronic inflammation. Cryoglobulinemia, liver cirrhosis, and HCV antiviral therapy are the most significant source of HCV-related lung and heart diseases in those persons suffering with advanced liver diseases. The classic anti-HCV therapy (IFN-RBV) is also linked with many adverse effects, however, with the discovery of new directly acting anti-HCV compounds the IFN-RBV-mediated side effects will be decreased with the more efficient viral control.
Footnotes
Acknowledgment
IQ received funding from KACST large grant #162-34.
Author Disclosure Statement
No competing financial interests exist.