
Abstract
Canine parvovirus (CPV-2) is an important cause of hemorrhagic enteritis in dogs. In Australia the disease has been associated with CPV-2a and CPV-2b variants. A third more recently emerged variant overseas, CPV-2c, has not been detected in surveys of the Australian dog population. In this study, we report three cases of canine parvoviral enteritis associated with CPV-2c infection; case 1 occurred in an 8-week-old puppy that died following acute hemorrhagic enteritis. Cases 2 and 3 were an 11-month-old female entire Saint Bernard and a 9-month-old male entire Siberian husky, respectively, both which had completed vaccination schedules and presented with vomiting or mild diarrhea only. Full genomic sequencing of parvoviral DNA from cases 1, 2, and 3 revealed greater than 99% homology to known CPV-2c variants and predicted protein sequences from the VP2 region of viral DNA from all three cases identified; glutamic acid residues at the 426 amino acid residue, characteristic of the CPV-2c variant. Veterinary professionals should be aware that CPV-2c is now present in Australia, detected in a puppy and vaccinated young adult dogs in this study. Further characterization of CPV-2c-associated disease and its prevalence in Australian dogs requires additional research.
Introduction
C
In this study, we report three cases of canine parvoviral enteritis associated with the CPV-2c variant, detected in veterinary clinics in Adelaide, South Australia. The clinicopathological features of disease associated with the CPV-2c variant are described in a fatal case of hemorrhagic enteritis in an 8-week-old puppy and two cases of nonfatal gastroenteritis associated with CPV-2c infection in young adult vaccinated dogs. In all three cases, full genomic sequence data for the associated CPV-2c variant are reported.
Case Reports
Case 1
Case 1 was an 8-week-old Staffordshire bull terrier female that was presented to the referring veterinarian in January 2015 with a 6 h history of lethargy and severe hemorrhagic diarrhea. On examination, the puppy was depressed with pale mucous membranes, dehydration was estimated to be greater than 10%, and rectal temperature was 36°C. Rectal examination revealed hemorrhagic diarrhea, however, the puppy tested negative for canine parvovirus using a commercially available patient-side Blot Test (IDEXX Laboratories, Maine) for detection of CPV-2. This pup had been vaccinated with a commercial vaccine against the CPV-2 strain 10 days previously, and no other puppies from the litter showed clinical signs. The pup died within 30 min of clinical examination, and the cadaver was referred to the University of Adelaide's Veterinary Diagnostic Laboratory for postmortem investigation the same day.
The puppy weighed 1.3 kg and was in lean to thin body condition with pale pink-gray mucous membranes, sunken eyes with bilateral prolapse of the nictitans, and tacky dry subcutaneous connective tissue, interpreted as hypovolemia and/or anemia and dehydration. The major gross findings at postmortem were melena, severe extensive ulcerative and hemorrhagic enteritis, most severe in the proximal to mid-small intestine, and hemorrhagic colitis. Representative tissues were collected for fixation and routine histological processing, and duplicate fresh tissues were frozen (−20°C) or chilled at 4°C. Histologically, sections of proximal and mid-small intestine showed moderate to severe necrotizing and fibrinohemorrhagic ulcerative enteritis with crypt necrosis and Peyer's patch lymphoid depletion and necrosis characteristic of canine parvoviral enteritis (Fig. 1). Lesions were less severe in the colon, characterized by mild to moderate diffuse fibrinohemorrhagic colitis. Moderate lymphoid depletion and necrosis were present in the spleen, and the thymus was unremarkable. Bone marrow was not examined. Bacteriological cultures from segments of affected small intestine revealed a heavy mixed growth of nonhemolytic Escherichia coli, Enterococcus sp., and Providencia sp. No Salmonella spp. was isolated from primary or secondary cultures, and no significant growth was seen on anaerobic cultures.
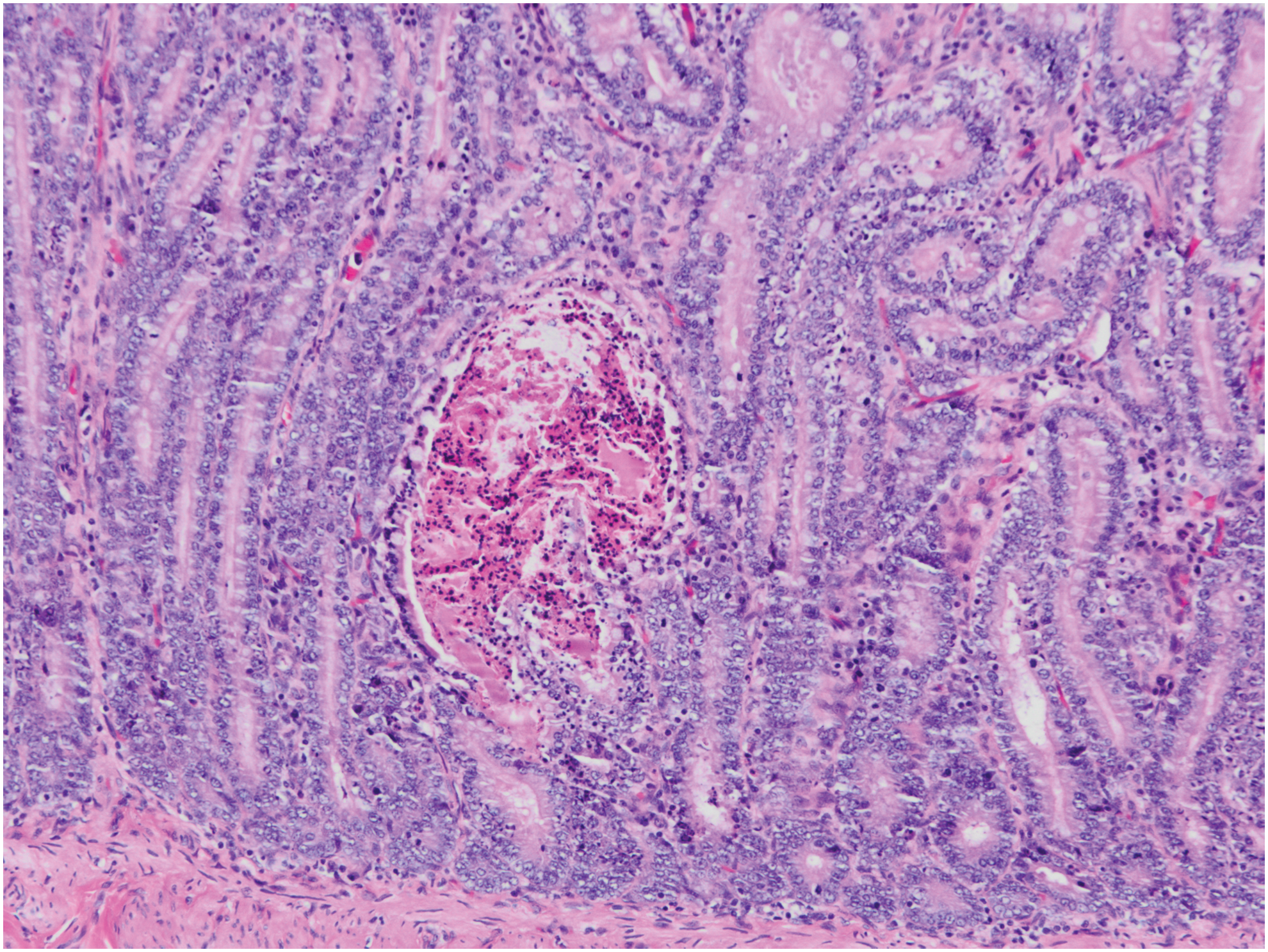
Photomicrograph of small intestine from CPV-2c-infected puppy (case 1). There is epithelial necrosis and dilation of crypts with accumulation of necrotic cell debris, protein, and inflammatory cells in the crypt lumen. Hematoxylin and eosin, 400 × . Color images available online at
Mucosal scrapings from fresh small intestine were subjected to DNA extraction using the QIAmp DNA Mini Kit (Qiagen, Germany) and an established polymerase chain reaction (PCR) assay for the detection of field and vaccine variants of canine parvoviruses (9). Primers F4 and R4 were selected, which amplify target DNA within the conserved VP2 region of the parvoviral genome (Table 1). Positive controls were 140 μL of CPV containing vaccines (Protech C3; Boehringer Ingelheim, Germany and Canigen DHA20; Virbac, France), and negative control was distilled water. The 442 bp PCR product from the intestinal sample and the CPV vaccines were submitted for sequencing. BLAST searches revealed that the amplified VP2 fragment from case 1 demonstrated 100% homology to the CPV-2c group (Accession number KM457142.1).
Case 2
Case 2 was an 11-month-old female entire St Bernard that was presented to the referring veterinarian in October 2015 with diarrhea, vomiting, and anorexia, which were initially suspected to have been secondary to a gastrointestinal tract foreign body. The dog had received a complete vaccination schedule as a puppy using a commercially available vaccine according to the manufacturer's protocol. Following 3 days of conservative management, an exploratory laparotomy was performed based on a presumptive diagnosis of the presence of a gastrointestinal foreign body. An intraoperative diagnosis of parvovirus infection was made via in-house fecal canine parvovirus antigen testing (Anigen, Republic of Korea). The patient recovered from surgery and was immediately referred to the Companion Animal Health Centre (CAHC) at the University of Adelaide for postoperative care. On examination, case 2 was ambulatory but still mildly sedated. She was tachypnoeic but all other cardinal signs were within normal limits. In-house combined canine parvovirus and canine coronavirus (CCV) antigen testing (Anigen) was positive for CPV and negative for CCV. Blood and feces were submitted to the Veterinary Diagnostic Laboratory (VDL) on day 1 of hospitalization. Twice daily physical examinations were performed and blood collected for full hematology and biochemistry profiles and coagulation profiles once daily.
Hematological findings were initially unremarkable, showing a mild left shift-neutrophilia only, before progressing to a mild leukopenia and neutropenia, mild nonregenerative anemia, and mild hypoproteinemia on day 4 of hospitalization. During the period of hospitalization, serum biochemical analysis revealed mild hypoproteinemia only and coagulation profiles were unremarkable. Fecal material from case 2 was subjected to the PCR assay for the detection of field and vaccine variants of canine parvoviruses as described for case 1. The amplified fragment of the VP2 gene from case 2 demonstrated up to 99.8% homology to the CPV-2c group.
Treatment over the ensuing 4 days consisted of intravenous fluid therapy, broad-spectrum intravenous antibiotics, antiemetics, gastroprotectants, and analgesia. After initial stabilization, there were minor bouts of mild vomiting and diarrhea, however, this resolved by the end of day 2 and did not recur for the remainder of hospitalization. Throughout hospitalization, the patient was anorectic and appeared to be persistently nauseous. Small amounts of soft canned food were administered daily, and this was tolerated well. Over the course of hospitalization, the dog became subjectively brighter and by day 4 was transitioned to oral medication. By day 5, despite a reluctance to eat voluntarily in hospital, she was showing an interest in food and was discharged home from hospital on broad-spectrum antibiotics and antiemetics. The dog responded well to therapy and made a complete recovery.
Case 3
Case 3 was a 9-month-old male entire Siberian husky that was presented to the referring veterinarian in November 2015 with a 3-day history of anorexia and vomiting, but no history of diarrhea. The dog had received a complete vaccination schedule as a puppy using commercial vaccines against the CPV-2b strain according to manufacturer's recommendations. Fecal antigen CPV testing (Anigen) was performed at the referring veterinarian and, on returning a positive result, the patient was referred to the CAHC for management. On presentation, the dog was ambulatory and noted to be bright alert and responsive. In-house combined canine parvovirus and CCV antigen testing (Anigen) was positive for CPV and negative for CCV. Blood and fecal samples were taken from the patient on presentation. Twice daily physical examinations were performed and blood taken for full hematological and biochemical profiles once daily.
Hematological results showed no significant findings initially, with eventual mild white blood cell line suppression only during the period of hospitalization. Serum biochemical and coagulation profiles were unremarkable. Fecal material was subjected to the PCR assay for the detection of field and vaccine variants of canine parvoviruses as described for case 1. The amplified fragment of the VP2 gene from case 3 demonstrated 100% homology to the CPV-2c group.
Treatment over the ensuing 3 days consisted of intravenous fluid therapy, broad-spectrum intravenous antibiotics, antiemetics, gastroprotectants, and analgesia. On initial presentation, the patient was dehydrated and fluid balance was corrected over 12 h. There was no vomiting noted during hospitalization and only mild diarrhea developed on day 2. The patient remained anorectic throughout, however, his normal diet was a very specific diet, and he did not usually eat any of the food offered to him in hospital; thus it was difficult to tell if his anorexia was related to nausea, diet, or both. By day 3, the patient was much brighter, was transitioned to oral medication (despite ongoing refusal to eat), and was discharged home on antiemetics, antibiotics, and analgesia. The dog responded well to therapy and made a complete recovery.
Full genomic sequencing of isolates from cases 1–3
For determination of entire genomic sequence of the CPV-2 isolates from cases 1, 2, and 3, long range PCR (LR-PCR) was performed on extracted DNA, using the primer sets listed in Table 1 (11). External primers were selected from previous publications (9), and internal primers were designed in regions of conserved sequences based on full genome sequence alignment of all available CPV-2 sequences in the GenBank. All primers were synthesized by GeneWorks Australia. Amplification was carried out in 50 μL reactions comprising 5 μL 10 × High Fidelity PCR Buffer, 3 μL 50 mM MgSO4, 2 μL 10 mM dNTP Mix, 2 μL 10 μM of each primer, 4 μL DNA template, and 0.5 μL Platinum® High Fidelity Taq DNA Polymerase (Invitrogen, California) and made up to 50 μL using distilled water. The PCR cycling conditions were 2 min at 94°C, followed by 35 cycles of denaturation at 94°C for 30 sec, annealing at 52°C for 30 sec, and extension at 68°C for 2 min, followed by a final extension phase of 68°C for 5 min. DNA segments were separated using 1% agarose gel electrophoresis and then extracted using QIAquick Gel DNA Extraction Kit. Each PCR product was submitted to Australian Genome Research Facility Ltd (AGRF) for Sanger sequencing.
Reconstruction of the full genome sequences from overlapping LR-PCR sequences was performed using BioEdit (v.7.0.4.1). Reference CPV-2a, -2b, and -2c genomic sequences were retrieved from GenBank for use in nucleotide alignments using Clustal-W program (6). A phylogenetic tree was generated using the neighbor-joining method within the MEGA program (Version 6.06). Open reading frames were determined using BioEdit package v.7.0.4.1 (4). The entire CPV-2 genome amplified from all cases was 4,269 bp in length and encoded four open reading frames, NS1, NS2, VP1, and VP2. Phylogenetic analysis revealed each of the three genomes located within the CPV-2c cluster (Fig. 2) and demonstrated more than 99% homology to known CPV-2c variants. In addition, the genome homology, the existence of a glutamic acid residue at the position of 426, a molecular marker for CPV-2c variants, was detected in all three samples. The full genome sequence data from each of cases 1, 2, and 3 were deposited in GenBank under accession number KU508691, KU508692, and KU508693, respectively.
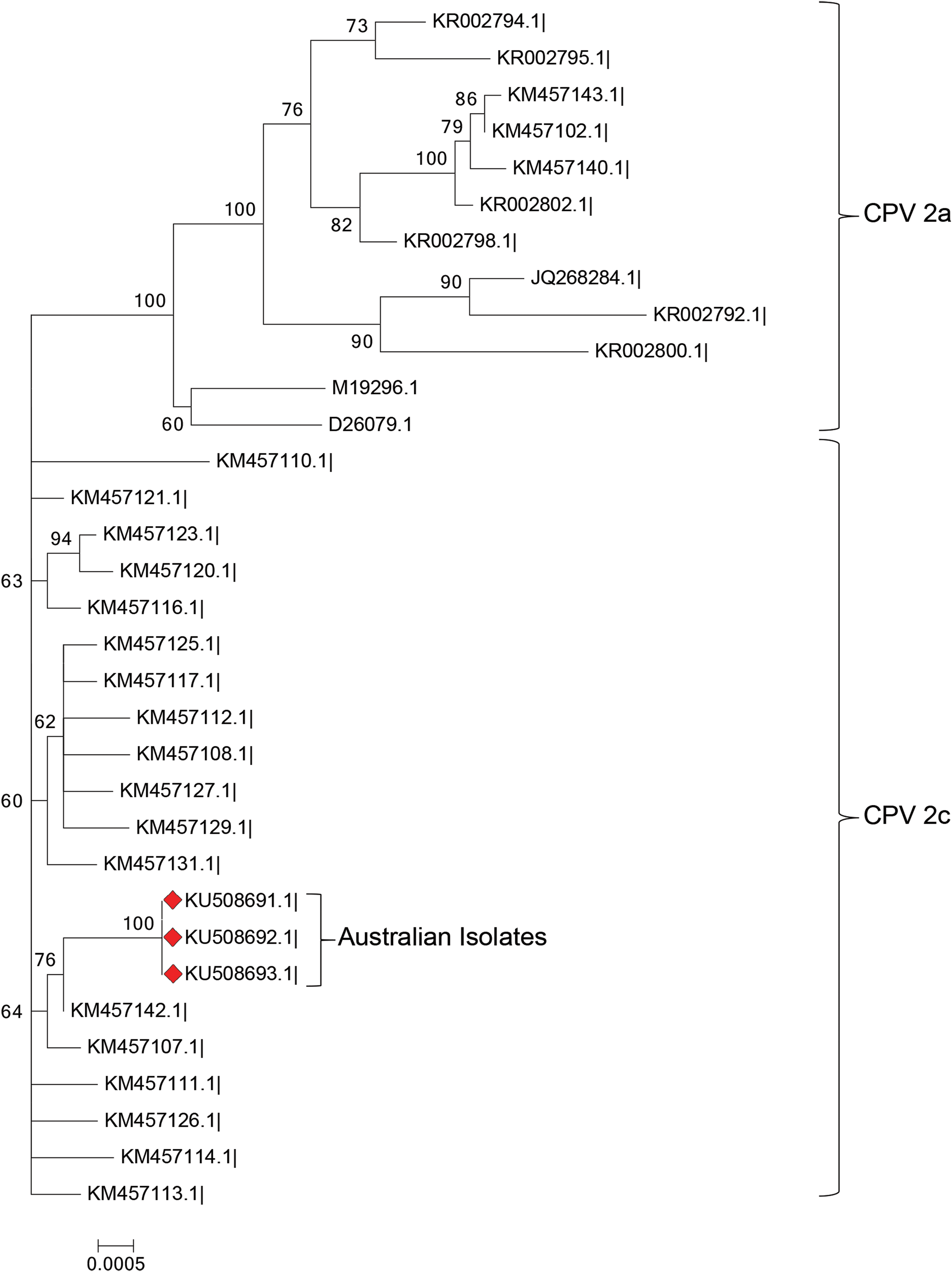
Neighbor-joining phylogenetic tree constructed using MEGA program (Version 6.06) comparing the amplified parvovirus genome from cases 1–3 (KU508691, KU508692, and KU508693) with known CPV-2a, CPV-2b, and CPV-2c sequences. Color images available online at
Predicted viral VP2 amino acid sequence analysis
Predicted protein sequences for the VP2 gene amplified from all cases were determined using BioEdit package v.7.0.4.1. Analysis of predicted amino acid sequences of VP2 gene fragments identified during initial PCR analysis for all cases identified glutamic acid at amino acid residue 426, consistent with previously characterized CPV-2c isolates (Fig. 3).
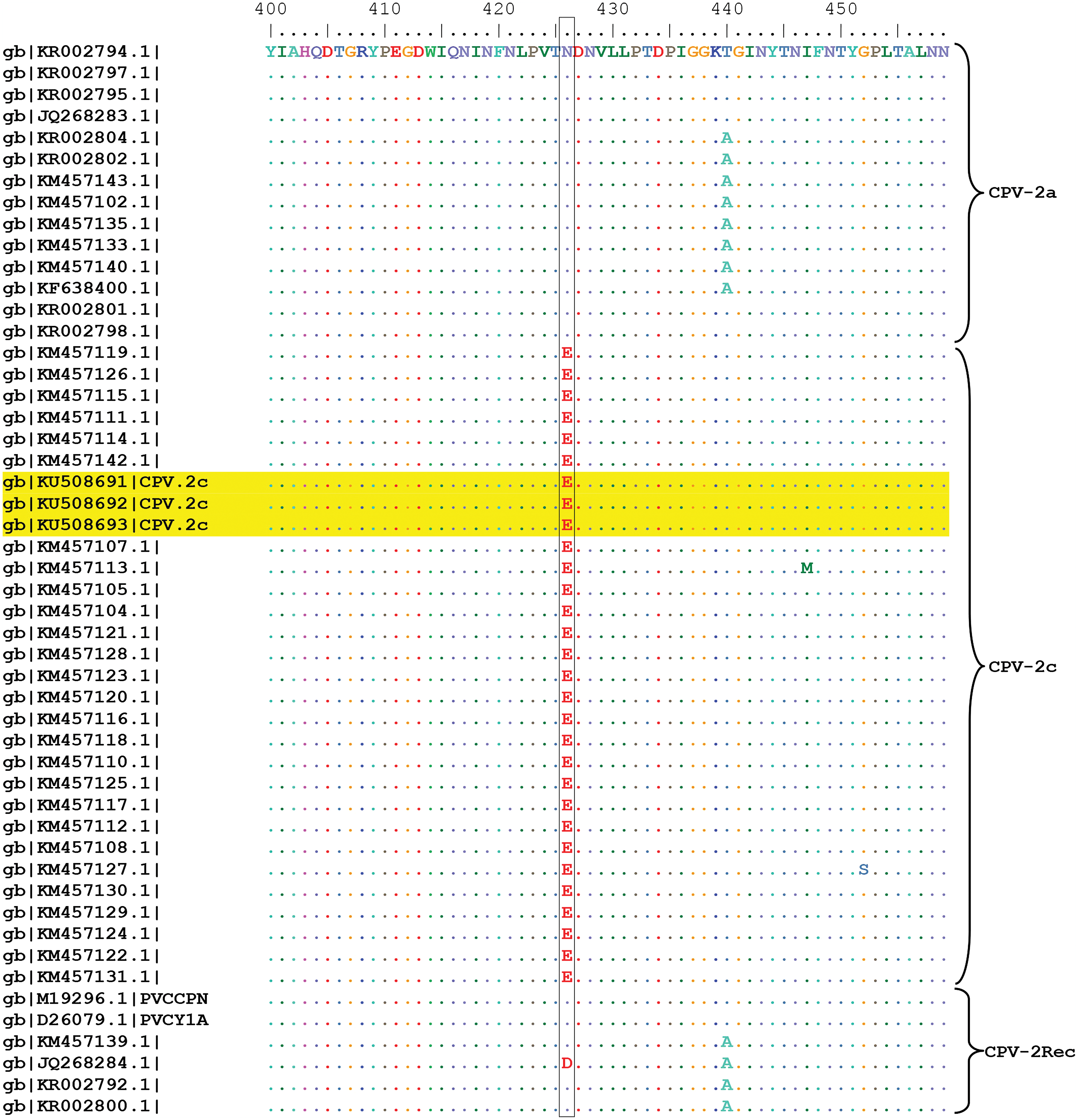
Predicted protein sequence for the VP2 region of known CPV isolates accessed from GenBank and the isolates from cases 1–3 (KU508691, KU508692, and KU508693). Glutamic acid (E) is present at amino acid residue 426 in predicted protein sequences from viral genomes amplified from all cases, supporting their classification as CPV-2c variants. Color images available online at
Discussion
Recent epidemiological surveys demonstrate that the prevalence of CPV-2c is expanding worldwide, and findings from this study indicate that this variant is now present in the Australian dog population. CPV-2c is reportedly associated with disease in adult dogs, as well as in dogs that have completed the vaccination protocols (1). Consistent with these reports, two of the cases presented in this study occurred in young adult, vaccinated individuals. The young adult dogs were presented with nonspecific gastrointestinal-related clinical findings (i.e., vomiting without diarrhea or mild diarrhea only and with little to no evidence of bone marrow suppression). From a clinical perspective, the vaccination status and age of a canine patient presenting with nonspecific gastrointestinal signs have traditionally been used as criteria to down grade CVP-2 infection on the list of differential diagnoses, however, these findings demonstrate that clinicians need to preserve parvoviral infection in their list of differential diagnoses for acute gastrointestinal disease, regardless of age, vaccination status, and severity of clinical signs. The reason for the milder clinical signs presented by each of the young adult dogs compared with typical parvoviral enteritis (i.e., severe hemorrhagic diarrhea, vomiting, and bone marrow suppression), is not known. Possible reasons include partial immunity conferred by previous vaccination schedules or possibly reduced virulence of the CPV-2c variant. Relative virulence of CPV-2c variant compared with other variants has not been established experimentally or on the basis of field observations overseas, with variable pathogenicity reported in experimental studies (2,12), and further investigations are required. As for other variants, pathogenic potential of CPV-2c is most likely influenced by factors such as age, immunological status, environmental stressors, and so on (1).
The two young adult dogs had completed puppy vaccination schedules, and the 8-week-old puppy had received a single vaccination only. Many potential causes of vaccine failure exist, including (but not limited to) improper administration technique or inappropriate vaccine handling, interference with the immune response by maternal antibodies, environmental pathogen load, the degree of attenuation of the vaccine virus, and the variant of the virus used. A recent systematic review examining the efficacy of currently available vaccines to provide protection against the CPV-2c variant was inconclusive (5), therefore, vaccine failure due to inadequate coverage for this variant cannot be excluded. In the case of the puppy, it is also possible that infection occurred prevaccination.
The source of CPV-2c in each case is unknown. Case 1 was from a large dog breeding facility; information on the origin of the breeding stock at this facility was not available, and it cannot be excluded that breeding stock imported from interstate and overseas were present within the facility. No molecular investigations into circulating CPV variants had been previously performed at the property. Case 2 was from a single dog home. Case 3 lived with two other vaccinated dogs and had no socialization with other dogs, however, did go for walks in public reserves. Cases 2 and 3 were both examined at a veterinary clinic with a large clientele of dog breeders.
Future research directions aim to determine the prevalence of CPV-2c in the Australian canine population and examine the sensitivity and specificity of commercially available patient side tests for detection of the CPV-2c variant. Patient demographics, clinical presentation, and pathological features of CPV-2c-associated disease in Australian dogs will also be investigated.
Footnotes
Acknowledgments
With thanks to the referring veterinarians and owners for inclusion of case material in this report. Thanks to Adrian Hines for assistance in necropsy, Cheryl Day for production of histology slides, and Ken Lee for bacteriological investigations.
Author Disclosure Statement
No competing financial interests exist.