
Abstract
Many emerging viruses such as Ebola and Lassa occur in resource-limited areas of the world. The advent of multiplex immunoassays has facilitated the study of biomarkers of disease since only small amounts of clinical material are required; however, such assays are designed and validated for only plasma or serum. This is a significant impediment when studying infectious diseases in the context of an outbreak in a developing nation. Plasma or serum can be difficult to obtain in the field due to the need for additional processing of infectious materials. Evaluation of multiplex immunoassays using frozen and thawed human whole blood (WB) would permit additional analysis using a more readily available human clinical sample. In this study, frozen and thawed human WB was directly compared with frozen and thawed plasma from normal healthy donors in a series of multiplexed immunoassays for 59 different biomarkers. We demonstrate that most important biomarkers can be evaluated using thawed WB, which will facilitate the study of human cytokine and other biomarker responses to viruses emerging in resource-limited regions.
Introduction
T
Methods
WB was obtained in acid citrate dextrose tubes from eight healthy donors as part of an approved human subjects research protocol for normal healthy donor phlebotomy (CDC IRB 1572). Blood from each donor was split into half: one half was aliquoted and frozen at −80
Results
Biomarker values were within the measurable range for the majority of the samples (>60% for both WB and plasma) for 35 of the 59 biomarkers evaluated. The 24 biomarkers that were below the limit of detection for most samples included IL-1β, G-CSF, IL-10, IL-13, IL-6, IL-17, GM-CSF, IL-5, VEGF, TNF-α, IL-2, IL-7, IP-10, MIG, IL-4, IL-8, Fractalkine, MCP-3, Granzyme B, sCD40 L, sFas-ligand, tissue factor, thrombomodulin, and IFN-β. This finding is consistent with earlier work conducted by our group using plasma from normal healthy humans with the exception of GM-CSF, IL-2, TNF-α, and IL-5 that were previously routinely detected above the assay limit of detection, although a different manufacturer's assay was used for these analytes in those previous studies. In this study, IFN-β was performed in a 2 h assay compared with previous work in which the assay was performed as an overnight incubation, which increases the sensitivity of the assay; this explains why IFN-β was below the limit of detection in our samples. Thrombomodulin was below the limit of detection in the samples used in this study but had been detectable in prior studies, possibly due to its membrane association and that these samples were centrifuged before analysis, which was not performed in previous work.
The differences that were observed between WB and plasma measurements were statistically significant for 21 of the 35 detectable biomarkers by the Student's t-test; this includes interferons, cytokines, chemokines, other inflammatory markers, markers of coagulopathy, markers of endothelial function, and growth factors (Table 1). All raw data are shown for each paired set of WB and plasma. The most notable differences were seen for IL-1RA that was a log higher in WB, and MCP-2 that was lower in WB than in plasma. These two analytes, along with IL-2R, which exhibited no statistical difference between WB and plasma, are depicted in Figure 1.
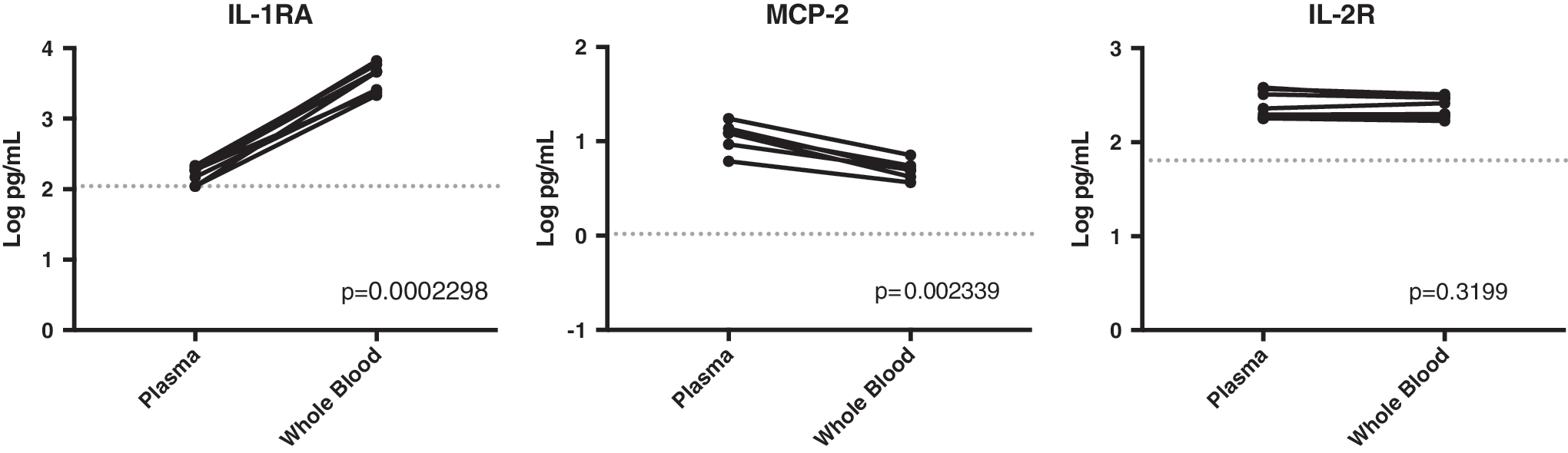
Representative graphic examples of whole blood versus plasma concentrations of several biomarkers. Examples of the three different outcomes are shown; IL-1RA was significantly higher in whole blood, MCP-2 was significantly higher in plasma, and IL-2R had no significant differences between measured levels in either matrix. Dotted line represents the limit of detection of the assay. p-Value obtained using the Student's t-test is noted on each graph. MCP, macrophage chemoattractant protein.
Starred (*) analytes indicate a p-value <0.05 as determined by the paired Student's t-test.
LOD, limit of detection; IFN, interferon; IL, interleukin; GRO, growth-regulated protein; MIP, macrophage inflammatory protein; MCP, macrophage chemoattractant protein; RANTES, regulated upon activation, normal T cell expressed and secreted; CFH, complement factor H; CRP, c-reactive protein; TNF, tumor necrosis factor; ADAMTS, a disintegrin and metalloproteinase with thrombospondin motifs; PAI, plasminogen activator inhibitor; PF, platelet factor; tPA, tissue plasminogen activator; vWF, vonWillebrand factor; PE-CAM, platelet and endothelial cell adhesion molecule; VCAM, vascular cell adhesion molecule; EGF, epidermal growth factor; FGF, fibroblast growth factor; HGF, hepatocyte growth factor; ICAM, intracellular adhesion molecule, did have detectable levels in all samples but was excluded from this analysis due to insufficient bead counts.
Discussion
The process of freezing WB results in lysis of the RBCs and white blood cells (WBCs) that are contained within the sample. Any biomarker contained within the cell would be released into the supernatant during this process and could affect the results. This is most important when assaying for biomarkers that might be produced by WBCs, such as cytokines and chemokines, or when assaying for iron storage products that might be higher in RBCs. This seems to be the case for IL-1RA, but was not as obvious with any of the other measurable immune markers, despite the fact that some differences were statistically significant. An additional consideration is that plasma constitutes ∼55% of blood volume, whereas the cells are ∼45%. Therefore, measurements made in WB might be “diluted” relative to the plasma since the volume used in each assay was identical.
Each of these assays uses two antibody pairs to detect a given analyte. One antibody is coupled to a unique magnetic bead and captures the analyte that is present in the sample. The second antibody is coupled to biotin and the complex is detected with a streptavidin molecule linked to the fluorophore phycoerythrin. When a particular manufacturer develops a commercial assay, they may not use the same two antibodies for capture and detection as another manufacturer, and this could influence the sensitivity of the assay. This has been observed in our studies and underscores the importance of establishing a series of normal values for any particular sample type in a given assay to permit appropriate interpretation of the results. Since most analyses are conducted in patients with different diseases, it is always helpful to have a cohort of normal healthy subjects for comparison.
The most important finding in this study was that frozen and thawed human WB is an acceptable matrix for multiplex immunoassays. The fact that there are statistically significant differences between the concentration values obtained in WB versus plasma underscores the importance of including a cohort of normal healthy subjects using the same sample matrix for comparison. The normal values obtained from frozen and thawed WB samples in these assays only apply to these specific manufacturers' assays performed with the same incubation duration, and should not be extrapolated to other manufacturers' assays or to different incubation times. These assays were not performed on fresh WB. Fresh WB contains cells with intact membranes that have the ability to respond to stimulation and the potential to release additional biomarkers that could complicate interpretation of the data.
For investigators who study emerging viruses such as the hemorrhagic fever viruses or other contagious pathogens that occur in spontaneous outbreaks in the developing world, this study will prove quite useful. It solves one issue related to the limited resources that are found in the developing world outbreak scenario—no need for additional manipulations or centrifugation of the samples, thus making the process of storing samples safer and easier. Freezing of the sample will still be necessary for integrity of the assays and for the intentional lysis of the cells contained within a WB preparation. This protocol does not obviate the need to transfer the sample to a laboratory with appropriate containment and technical resources, but it makes collection of the sample in the field much more practical.
Going forward it will be important to conduct these same assessments in stimulated samples to permit for analysis of additional biomarkers that were not detectable in normal healthy humans. In addition, greater samples sizes and evaluation of the effects of different coagulants on the measured concentrations are also needed.
Footnotes
Acknowledgments
The views expressed in this article are those of the authors' and do not represent the official position of the U.S. CDC. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. This work was performed while Anita McElroy held an NIH K08 (AI119448) and a Burroughs Wellcome CAMS (1013362.01).
Author Disclosure Statement
All authors declare that no competing financial interests exist.