
Abstract
Hepatitis C virus (HCV) signifies an important health issue as it is a globally prevalent pathogen and poses a great threat to human health. Direct antiviral therapy became a landmark in treatment against chronic HCV infection as they have proven to increase sustained virological response (SVR) rate, provide shortened and simplified regimens. This study aimed to evaluate efficacy of Sofosbuvir and classify factors of treatment success and their function in therapy continuation decision. We studied host and viral factors in 310 patients who received Sofosbuvir (DAA) at a dose of 400 mg daily along with ribavirin 10 mg/kg body weight for 24 weeks and followed by 12 weeks after completion of treatment. A total of 302 patients (97.42%) showed end-of-treatment response. However, 8 patients (2.58%) were virological nonresponders and 286 patients (94.70%) achieved SVR. Among 310 HCV positive, the percentage of viral genotype 3-infected patients was 89.6%, whereas only 10.32% were affected by HCV genotype 1. Multivariable analysis showed that baseline HCV RNA (≤8 × 106 IU/mL vs. >8 × 106 IU/mL) [95% confidence interval (CI), odds ratio (OR) 3.0, 2.0 to 8.4; p = 0.004], age (<50 vs. ≥50 years) (95% CI, OR 1.9, 3.0 to 10.1; p = 0.03), liver texture (normal liver vs. coarse) are related to virological response. None of the patients included in the study has S282T substitution in NS5b of HCV. No significant difference in response was observed in patients with different genotypes of rs12979860. Liver texture, age, and viral load are predictors of SVR. In this real-life data no substitution of S282T in NS5b was observed related to failure of therapy. Oral Sofosbuvir generally has a high tolerance and can effortlessly beat the safety concerns of past regimens.
Introduction
H
Chronic infection with HCV may cause liver cirrhosis and can lead to development of hepatocellular carcinoma. Because of unavailability of any protective vaccine, it is essential to successfully treat the infection, but it imposes huge medical and societal costs. The aim of successful treatment is to eradicate infection and to facilitate in acquiring a sustained virological response (SVR), which is defined as serum HCV RNA level undetectable after 6 months of treatment cessation that is tantamount to HCV cure. Patients who achieve an SVR showed best signs of successful treatment, lower mortality, and morbidity rates in comparison with nonresponders.
Pegylated-interferon (PEG) and ribavirin (RBV) was regarded as a standard of care for chronic HCV infection. Use of pegylated therapy is related with psychiatric issues and hematologic abnormalities (8,21). In addition, a considerable number of patients (15–30%) are resistant to interferon therapy. Various side effects have been accounted for the use of combination therapies, including first-generation direct acting antiviral with RBV and interferon (17). In contrast to first generation, the second-generation DAA showed minimal side effects and also had the advantage of shorter therapy duration with >90% of cure rates in phases II or III clinical trials (23). Furthermore, for HCV distinct protein targeting, combination therapy of multiple DAA can eliminate the need of interferon (7,26).
Recent development of direct antiviral drugs has revolutionized the HCV treatment. These therapies open era of new therapeutic approaches, targeting the viral genome which encodes proteins that have vital role in replication and assembly of HCV. Direct antivirals become a landmark in the treatment against HCV infection as they have proven to increase SVR rate, provide shortened and simplified regimens, while also lessening the side effects related to treatment (11,19,30). Sofosbuvir is a nucleotide inhibitor which directs chain termination in case of its use as false substrate by RNA polymerase. Additionally, it targets a highly conserved active site. This feature provides high barrier to resistance. It displays pan-genotyping activity against all genotypes (24,27). Moreover, it has a favorable safety profile (11,19,30).
HCV is an RNA virus having six genotypes. According to treatment guidelines, HCV genotypes 2 and 3 were grouped together as “easy-to-treat” genotypes before the advent of direct-acting antiviral (7). But recent studies indicate that they show difference in responses. HCV genotype 3 is linked to immediate disease progression that leads to hepatic steatosis and the possibility of higher risk of hepatocellular carcinoma and lower treatment response rate as compared with HCV genotype 2 (1,12). Treatment of genotype 3 is the most advanced therapy to date as it is less susceptible to first generation of DAA and even also less susceptible to Sofosbuvir, which is a second-generation DAA and is considered the most advanced therapy to date (16). Globally, HCV genotypes 2 and 3 accounts for 30% of HCV infection; however, in Pakistan, genotype 3 constitute >80% of HCV infection (4). The efficacy of Sofosbuvir-based treatment regimens has been demonstrated in different trials (phases II and III) on preselected patient population that does not show a good representation in difficult-to-treat categories of patients.
The present study is based on the diverse patient's population with other variable factors to predict the efficacy in terms of sustained suppression of HCV RNA and identify the factors influencing antiviral therapy response rate. These data may add to available literature and may benefit in assessing its consistency in the real-life setting.
Materials and Methods
Study design
The present study was conducted on patients who showed presence of HCV RNA and presently opted direct antiviral treatment from May 2014 to December 2015. The study was approved by the Ethics Committee of Maroof International Hospital, Digestive Disease Study Group. Informed consent was taken from all patients included in the study. For this study, a total of 348 patients were enrolled. Patients included in this study were negative for hepatitis B virus. After seeing their profiles only 310 patients who fulfilled whole criteria for the study were selected for antiviral therapy. All patients had hemoglobin level >13 g/dL among males and >12 g/dL among females, total white blood cells count was >3,000 cells/mm3, and platelet count was >100,000 cells/mm3. Moreover, patients did not suffer from any comorbidity such as autoimmune disorders, depression, and cardiac disease or decompensated liver disorder. Pregnant females and patients <18 and >70 years of age were excluded. The baseline characteristics of patients are given in Table 1. During each patient visit, patient's complete blood count, prothrombin time, and alanine aminotransferase (ALT) were analyzed. After 4 weeks of treatment, HCV RNA analysis was conducted for detection of virological response. IL28B (rs12979860) polymorphism was detected at baseline and S282T substitution in NS5b was analyzed in nonresponders and relapse to therapy. The ultrasonic evaluation to determine the condition of liver in chronic liver disease was performed by assessing different factors. These included size of liver, coarseness of live parenchyma, liver edge bluntness, and size of lymph node around the hepatic artery. A double-blind trial method was used; each ultrasound report was performed by two qualified radiologists, independent of evaluation of others, to remove biasness. Patients were regarded as End Treatment Responders if negative for HCV RNA after their therapy completion. Only End Treatment Responder patients were given a follow-up visit. At each monthly or follow-up visit (after 24 weeks), detailed physical examination of each patient was done. Throughout the study, any adverse events were recorded up to 24 weeks of follow-up period.
ALT, alanine aminotransferase; BMI, body mass index; HCV, hepatitis C virus; ULN, upper limit of normal.
Drug administration
The enrolled patients were administered with Sofosbuvir at a dose of 400 mg daily along with RBV 10 mg/kg body weight for 24 weeks.
Efficacy assessment
Serum HCV RNA quantification was done in COBAS AmpliPrep/COBAS TaqMan HCV Quantitative Test, version 2.0 (Roche Molecular Systems) having 15 IU/mL as lower limit of viral detection after 4 and 12 weeks, at end, and 12 weeks posttreatment. Genotypes and subtypes of HCV were evaluated using Real-Time HCV Genotype (Abbott). Adverse effects resulting from treatment were noted and evaluated. The major endpoint of this study was the assessment of SVR, which is defined as HCV RNA undetectable in serum after 12 weeks of end of treatment. Whereas, rapid virological response (RVR) is mostly described as HCV RNA becoming undetectable after 4 weeks of continuous treatment. Another term, that is, patient relapse, is described as those patients who first achieved a state of complete negative HCV RNA after the therapy ended, but during follow-up time showed recurrence of HCV RNA (i.e., positive HCV RNA).
IL28B polymorphism (rs12979860)
Previous studies showed that IL28B types are correlated with therapeutic outcome (28,38). PCR amplification and sequencing of rs12979860 single-nucleotide polymorphism was used for genotyping of IL28B. Whole blood was collected in K2EDTA container and stored at OPERON (Ultra-low Temperature Freezer) −86°C for DNA extraction. DNA is amplified by using the method described by Aziz et al. (3). The amplified product was purified by using the QIAquick PCR Purification Kit from QIAGEN. The purified product was subjected for sequencing on ABI sequencer and electropherogram of nucleotide sequence was analyzed by using Chromas Lite software.
Detection of S282T in HCV NS5B
HCV NS5b sequence was amplified by using primers, forward primer 5-TGACTCCACAGTCACTGAGAGC-3, and reverse primer 5-CTCCGTGAAGGCTCACTTTC-3 purified using the QIAquick PCR Purification Kit from QIAGEN. The purified product was then sequenced using dye-deoxy terminator method on ABI Prism Sequencer (PE Applied Biosystems) using 5 pmol of either forward or reverse primers. Nucleotide sequence was compared with sequence of different genotypes obtained from NCBI by using CLC Work Bench Software.
Statistical analysis
Statistical analysis was done using SPSS v. 15.0 (SPSS, Inc., Chicago, IL). Categorical variables are expressed in this article as numbers and percentages. Significant differences between categorical variables were estimated using the Pearson's χ 2 test. A p-value <0.05 is a significant value. Potential variables were predicted using univariate and multivariate logistic regression analysis.
Results
A total of 348 patients were enrolled in the study for determining the efficacy of Sofosbuvir. Twenty patients refused to participate, and they were excluded. Another 18 patients could not meet inclusion criterion. Of the remaining 310 patients, 132 were male, whereas 178 were female. The mean age of study participants was 41.2 ± 13.5 years. HCV had been acquired in most of the patients through dental surgery (43.54%), surgery (19.3%), barber (14.5%), and blood transfusion (5.48%) whereas 17.09% patients were unaware of the source of infection. Table 1 summarizes the baseline characteristics.
Out of 310 patients, 302 patients (97.42%) showed end of treatment response and 8 (2.58%) were virological nonresponders, who showed detectable HCV RNA even at the end of treatment. Sustainable reduction in the viral load of HCV patients observed who received sofosbuvir–ribavirin therapy. Of these 302 patients, 286 (94.70%) achieved an SVR at 12 weeks after the cessation of the treatment. Further analysis showed that patient response to treatment varied with respect to their treatment history. Patients who were previously treated had lower virological response as compared with naive patients.
A total of 276 patients (89.1%) attained virological response at week ≤4. Among these, 258 (93.4%) patients achieved SVR, whereas 18 patients (6.52%) showed detectable viral load within 12 weeks of follow-up. While patients achieved virological response at >4 week, 28 patients (82.35%) achieved SVR. The rate of SVR was remarkably higher in patients with RVR in comparison to those without RVR (93.4% vs. 82.35; p < 0.04) (Table 2). According to HCV genotypes, the SVR among 278 HCV genotype 3-infected patients was 93.2% (259); however 84.37% (27) of patients infected with HCV genotype 1 showed SVR. Patients with normal liver sustained 97.35% (239/245) virological response (Fig. 1) as compared with 72.3% in the patients who have coarse liver texture.
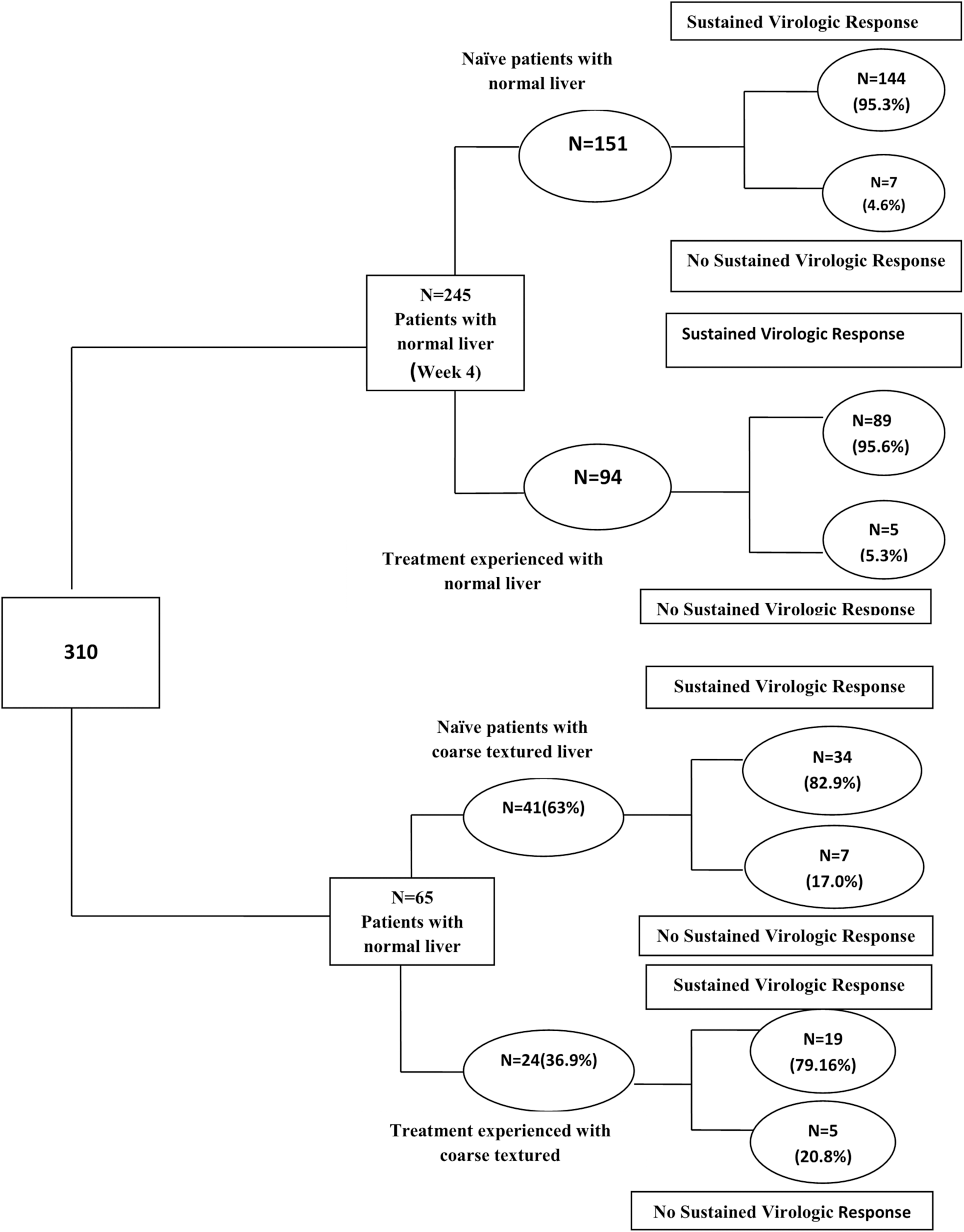
Schematic flowchart of the enrolled patients shows sustained virological response obtained in patients with normal liver compared with patients having coarse-textured liver. N shows number of patients along with their percentage in the studied population.
SVR, sustained virological response.
The SVR in different subgroups are given in Figure 1. The rates of SVR among patients who showed absence of coarse texture on abdominal ultrasound having previous treatment and among those who are naive (not received any previous treatment) were 90.0% and 93.2%, respectively (difference = 3.2%). SVR among naive patients with coarse-textured liver is 82.9%, whereas among treatment-experienced patients with coarse-textured liver is 79.16% (difference in response = 3.74%).
The frequency of rs12979860 genotype was found to be: CC 55.1%, CT 36.4%, and TT 8.38%. SVR achieved in 93.3% patients have favorable genotype CC of rs12979860, whereas non-CC genotype patients achieved 90.16% SVR (p = 0.09). Amino acid sequences of 229–326 were analyzed and aligned with reference sequences extracted from NCBI. These regions fall in Motif B, C, and D and they form the fingers and palm region of the HCV NS5B polymerase sequences. Motif B (Fig. 2) includes 282–292 sequence (i.e., SGVLTTSCGNT) and Motif C regions are 317–319 (i.e., GDD). Motif D forms the main palm region, whereas from Motif D only 326, that is, S, aa was analyzed. Motif C, here, is of great importance as it is a highly conserved site with sequence GDD; it forms the triad catalytic site. Our samples showed few mutations at different sites. For genotype 1a (Fig. 2b) mutations were C243S, R300Q, M313K, V321F, I323V/F, C324A/N, and E325G. For genotype 3a they were E246D, S269R, A272D/L, R278S, A303S, G306V, L308F, R309K, D312S, L314R, and V315L. For genotype 1b, mutations (Fig. 2a) identified were at region N231S, V235T, S238A, C243S, A246D, E248Q, Q251V, R254K, I262V, K270R, Q272E, Y284V, L297I, S300Q, K307G, M313K, V321F, I323F, and E325G. Alignment of sequence of nucleotide codon was compared. This study reports no S282T variant of NS5b region of HCV found in either responder or nonresponder group.
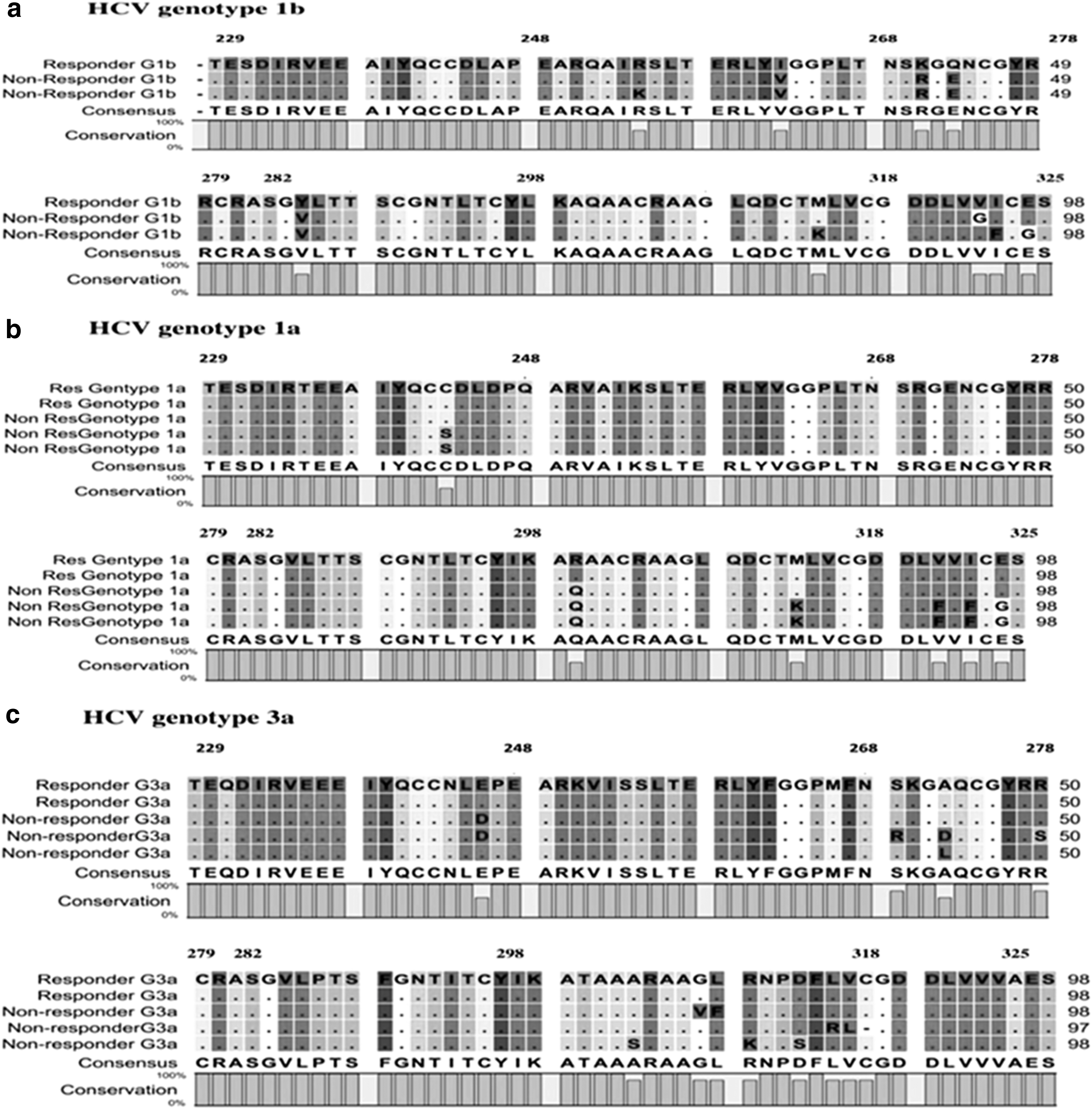
Amino acid analysis of NS5b sequence using CLC sequence software.
Factors that contributed to therapy response were analyzed using univariable and multivariable logistic regression analysis. In univariable logistic regression, the following independent variables were included: sex, age, viral load, RVR, HCV genotypes, body mass index, IL28B genotype, S282T in NS5B region, pretreatment ALT, previous response to therapy, and liver texture. Among these four factors, age <50 years [95% confidence interval (CI), odds ratio (OR) 1.9, 3.0 to 10.1; p = 0.03], RVR (95% CI, OR 3.1, 0.78 to 3.21; p = 0.7), normal liver versus coarse texture (95% CI, OR 2.9, 4.1 to 5.66; p = 0.005), and baseline HCV ≤8 × 106 IU/mL (95% CI, OR 3.0, 2.0 to 8.4; p = 0.004) showed significant impact on response to therapy. IL28B genotype has no relation with response to therapy. Multivariable logistic regression followed univariable analysis for identification of factors associated with clinical response. Multivariable analysis showed that baseline HCV RNA (≤8 × 106 IU/mL vs. >8 × 106 IU/mL), age (<50 vs. ≥50 years), and liver (normal liver vs. coarse texture) are associated with virological response (Fig. 3).
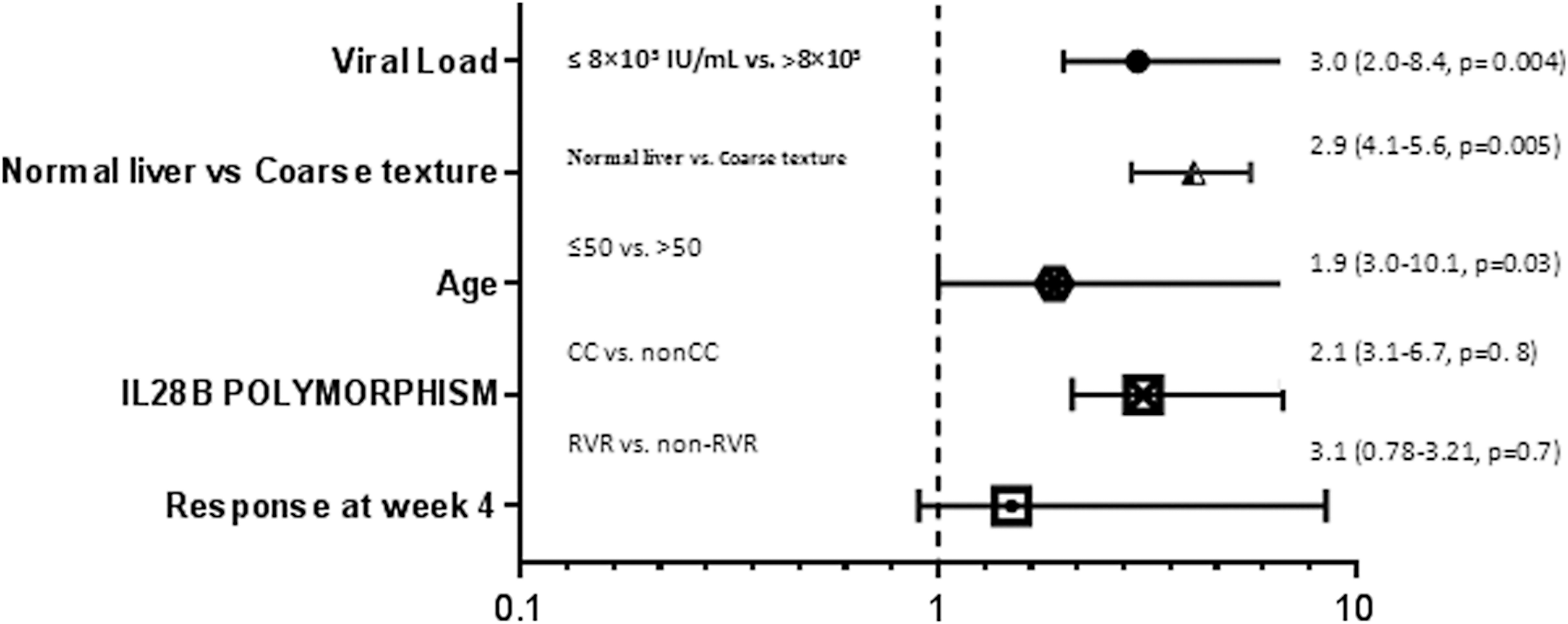
Multivariable logistic regression model predicts sustained response. CC, genotype of rs12979860 IL28B; non-CC, CT, and TT genotypes of rs12979860 IL28B; RVR, rapid virological response.
There were few adverse events that were associated with the combination therapy of sofosbuvir and ribavirin (400 mg +10 mg/kg body weight daily for 24 weeks); none of the adverse events associated with therapy was severe. There were total of 40 patients receiving combination therapy who suffered with headache, 11 with nausea, 30 with anemia, dyspnea was seen in 7 patients, 25 patients suffered with fatigue, and only 1, 2, 3, and 4 patients showed neutropenia, vomiting, pruritic rash, and dizziness, respectively.
Discussion
A promising novel NS5B region inhibitor showing high antiviral activity, wide-range genotype coverage, with low resistance, has been introduced for the treatment of chronic HCV (11,20). Sustained viral suppression is one of the therapeutic goals in HCV patients. Presently, the approved antiviral regimens are not effective uniformly for all HCV genotypes. DAA drug treatments for HCV gained widespread acknowledgement. In this study, high rates of SVR in HCV patients were observed regardless of patients having previous treatment history or not. According to Cha et al. (5) no prominent difference in SVR was observed in different genotype groups. All three clinical trials, that is, The FISSION Trial, The NEUTRINO Trial, and The FUSION trial were conducted and SVR in ∼1,500 patients was above 93% (5). In this study, an overall SVR rate was observed in 92.26% of patients. Among patients who were previously treated had lower virological response (90.68%) as compared with naive patients (93.2%). This was in accordance with previously reported study that higher SVR was observed in previously untreated patients (93%) than treated patients (91%) (9). Patients having RVR showed considerably higher SVR. In the present analysis, 89% of patients achieved RVR and SVR rate were significantly higher among these (93.4%) as compared with the patients who did not achieve RVR (82.3%). This finding is in accordance with Steinebrunner et al. (34), who reported higher SVR in patients having virological response at week 4 (70 vs. 30, p = 0.006). By 4th week, the virological suppression rates in HCV-infected patients were 93–99% (16).
HCV genome is heterogeneous and classified into six genotypes and several subtypes. Distribution of HCV genotype varies with geographical region. As previously reported, HCV genotype 3 is an endemic in south eastern countries, including Pakistan, where higher percentage of viral suppression was observed in HCV genotype 3 patients in comparison with other group of genotypes. In agreement with earlier studies, we observed that HCV genotype 1 patient showed response (84.37%) not as good as HCV genotype 3 (93.16%) and were hard to cure reflected by Steinebrunner et al. (34), and Sulkowski et al. (35). In a subgroup analysis, patients were divided according to previous treatment experience and coarse texture of liver (on ultrasound abdomen). Previously treated patients with coarse-textured liver had lowest rate of sustained response (79.16%) as compared with naive patients with coarse-textured liver (82.9%) (Fig. 1). These results are in agreement with Zeuzem et al. (41), who reported 62% SVR in previously treated HCV genotype 3-infected patients with liver cirrhosis. In another study, Lawitz et al. (24) found SVR 92% (95% CI 89–95) among patients without cirrhosis and 80% (95% CI 67–89) among those with cirrhosis. The exact mechanism which causes decrease in SVR rate associated with advanced liver diseases is not well established. A possible mechanism can be that advanced liver diseases prevent antiviral drug perfusion, thus forming pockets with decreased drug concentration where HCV persists. Also patients suffering from cirrhosis also suffer from other infections due to impaired immunity.
Significant association of baseline viral load with response to sofosbuvir was observed. Patient having baseline viral load >6 log10 showed lower response as compared with patients who have baseline viral load <6 log10. Hartman et al. (13) reported that increased viral load is another factor contributing to treatment failure. Earlier studies showed that SVR rate was significantly lower in 89.62% of patients with high viral load than patient with low viral load (i.e., 95.28%) (10).
Numerous interferon-based studies showed difference in response between elderly and nonelderly patients and relationship of IL28b genotypes with response to therapy, but this difference is diminished with the use of interferon-free direct antiviral therapies. The lower response may be due to hepatocyte senescence that leads to the failure of interferon therapy (6,15,37). Substitution at codon 282 S → T has been experienced in vivo during different opted treatments, including sofosbuvir (11,14,25,31,36). In addition, scientific literature reported that variants (G/C/R) of codon 282 of NS5b confer resistance to sofosbuvir presented in in silico model (18). However, our detailed analysis of samples showed that there was no S282T mutation in responder and nonresponder HCV-infected patients, neither was any other mutation seen in close proximity of this region, except in genotype 1b mutation, that is, Y284V, which is close to S282. This shows that S282 position in NS5B region is highly conserved. From already published data, genotype 1a showed mutations at position 321; all other mutations in this study are new and not reported previously.
Conclusion
Liver texture, age, and viral load are predictors of SVR. In this real-life data, no substitution of S282T in NS5b was observed related to failure of therapy. Antiviral therapy with sofosbuvir once daily with RBV 10 mg/kg body weight resulted in high SVR rate in naive patients as compared with those treated previously. Potential drug resistance substitution S282T to Sofosbuvir was not detected. Treatment with Sofosbuvir lasts for 12–24 weeks, which is half the time of the treatment with interferon. Oral Sofosbuvir generally has a high tolerance and has fewer side effects as compared with past regimens.
Footnotes
Author Disclosure Statement
No conflicts of interest related to this article.